
Abstract
Background:
Asthma is a chronic inflammatory disease of the respiratory system characterized by wheezing, shortness of breath, and chest tightness. Although effective medications are available to control symptoms and prevent exacerbations, optimal outcomes depend largely on adherence to evidence-based treatment guidelines.
Objectives:
This study aimed to evaluate prescriber adherence to the Global Initiative for Asthma (GINA) guidelines, assess its impact on asthma symptom control, and identify challenges and barriers influencing guideline adherence.
Design:
A sequential explanatory cross-sectional study supplemented with qualitative interviews was employed.
Methods:
The study was conducted from May 16 to August 30, 2023. Quantitative data were obtained through structured medical chart abstraction, followed by semi-structured interviews to explore barriers to guideline adherence. Data were analyzed using SPSS version 25, and associations between independent variables and asthma control were examined using ordinal logistic regression. Statistical significance was set at p < 0.05.
Result:
Findings revealed that patients managed by prescribers not adhering to GINA guidelines had 72% lower odds of achieving symptom control (AOR = 0.28, 95% CI: 0.12–0.65, p = 0.003). Positive predictors of symptom control included monthly income of 5501–7000 ETB (AOR = 2.12, 95% CI: 1.02–4.40), mild persistent asthma compared with severe asthma (AOR = 2.63, 95% CI: 1.00–6.89), and use of low- or medium-dose budesonide plus formoterol inhalations daily (AOR = 8.26, 95% CI: 3.26–29.1, p = 0.001; AOR = 10.3, 95% CI: 3.27–32.6, p < 0.001, respectively). Conversely, married (AOR = 0.49, 95% CI: 0.25–0.98, p = 0.045) and divorced patients (AOR = 0.39, 95% CI: 0.19–0.81, p = 0.012), those prescribed medium-dose beclomethasone with salbutamol (AOR = 0.18, 95% CI: 0.07–0.45, p < 0.001), and patients with poor medication adherence (AOR = 0.36, 95% CI: 0.22–0.61, p < 0.001) showed significantly lower odds of symptom control. Qualitative findings highlighted barriers such as the extensiveness of the GINA guidelines, limited availability of recommended medications, and insufficient prescriber knowledge and training.
Conclusion:
Prescribers’ non-adherence significantly compromised asthma control. Strengthening guideline implementation requires improving medication accessibility, training healthcare providers, and enhancing awareness to optimize asthma management.
Plain language summary
Asthma is a common long-term disease that causes inflammation in the airways and cause to breathing problems such as shortness of breath, wheezing, and chest tightness. Medicines are often prescribed to control these symptoms and prevent future asthma attacks. This study aimed to find out whether physicians are following the Global Initiative for Asthma (GINA) treatment guidelines and how their adherence affects asthma symptom control among patients. It also explored the reasons why some providers do not fully follow the guidelines. The study used both quantitative and qualitative methods. From May 16 to August 30, 2023, researchers reviewed patient medical charts to collect important information and conducted interviews with healthcare providers to understand barriers to using the GINA guidelines. Data were analyzed using SPSS version 25, and relationships between variables were tested using ordinal logistic regression, with a significance level of p < 0.05. The findings showed that patients treated by physicians who did not follow the GINA guidelines were 72% less likely to have good symptom control of their asthma symptoms (AOR = 0.28, 95% CI: 0.12–0.65, p = 0.003). Better asthma control was linked with: Having a moderate monthly income (5501–7000 ETB) compared with higher income (>7001 ETB), having mild persistent asthma rather than severe asthma, and using budesonide plus formoterol inhalers daily, either in low or medium doses. Poorer asthma control was observed among: Married and divorced patients compared to single individuals, those using beclomethasone plus salbutamol inhalers, patients not adhering to their medications, and those treated by non-adherent prescribers .Interviews with prescribers revealed that poor adherence to the GINA guidelines was mainly due to: The complexity and length of the guidelines, limited access to recommended medications, and lack of training and awareness among prescribers.
Introduction
Asthma is a common non-communicable disease characterized by chronic airway inflammation that affects individuals across all age groups. The World Health Organization (WHO) estimates that more than 260 million people are currently living with asthma worldwide, making it one of the most prevalent chronic respiratory conditions. 1 The disease is characterized by airway symptoms such as wheezing, shortness of breath, chest tightness, and cough, which vary in severity and duration over time and are associated with variable expiratory airflow limitation. 1 These symptoms are triggered by a range of factors, including allergens such as pollen, exposure to environmental pollutants, respiratory infections, and physical exercise. 2 Globally, asthma remains a leading cause of morbidity and mortality, imposing a significant health and economic burden on individuals, families, and healthcare systems. 3 Uncontrolled asthma contributes to reduced quality of life, absenteeism from work and school, frequent hospital visits, prolonged hospital admissions, and preventable deaths across all age groups. 4
Effective asthma control is therefore essential to reducing exacerbations, improving quality of life, and preventing long-term complications. 5 To achieve this, clinicians rely on standardized treatment guidelines that promote consistent, evidence-based management through both pharmacological and non-pharmacological interventions. Among these, the Global Initiative for Asthma (GINA) guidelines are the most widely used guideline worldwide and are updated annually. GINA provides a comprehensive, patient-centered, stepwise approach to asthma diagnosis and management, emphasizing both symptom control and the reduction of future risks. 6 Notably, recent updates recommend the use of inhaled corticosteroid (ICS)–formoterol as a maintenance and reliever therapy, reflecting growing evidence of its superiority over short-acting beta-agonists (SABA) alone. 7
Despite their global importance, numerous studies have documented a persistent gap between guideline recommendations and routine clinical practice. 8 This discrepancy is driven by several interrelated factors, including inadequate knowledge or training among healthcare professionals, system-level barriers, limited availability and affordability of essential medications, and challenges related to patient adherence.9,10 Importantly, prescriber-level non-adherence to GINA recommendations has been strongly associated with poor asthma outcomes, including higher rates of uncontrolled symptoms, frequent exacerbations, and increased hospitalizations. 11 In low- and middle-income countries, including Ethiopia, where healthcare access and resources are often constrained, understanding the degree of prescriber adherence to GINA guidelines is particularly important. However, local data on prescriber practices remain scarce despite the growing burden of asthma. Furthermore, disparities in medication availability, especially in rural areas, and the high cost of controller therapies, such as ICS–LABA combinations, further complicate asthma management. 12
This study, therefore, aims to assess the level of prescriber adherence to GINA guidelines in Ethiopia, examine the relationship between guideline adherence and asthma symptom control, and explore provider-reported barriers to adherence. By identifying existing gaps and contextual challenges, the findings seek to inform strategies to strengthen guideline uptake, improve patient management, and ultimately reduce the burden of asthma.
Methods and materials
Study area
The study was conducted in public hospitals located in the South Gondar Zone. Debre Tabor is the capital city of the South Gondar Zone and is located approximately 665 km from Addis Ababa, the capital of Ethiopia, and 103 km from Bahir Dar, the capital city of the Amhara Regional State.
Study design and period
A sequential explanatory mixed-methods study design was conducted among adult asthma patients. The study comprised a quantitative cross-sectional phase followed by a qualitative phenomenological phase. In the quantitative phase, a structured chart review was conducted to assess prescriber adherence to the GINA guidelines and to evaluate its association with patients’ asthma symptom control. Following analysis of the quantitative findings, the qualitative phase was undertaken, during which prescribers were purposively selected for semi-structured interviews to explore underlying reasons for non-adherence. The reporting of this study conforms to the Guidelines for Reporting Mixed Methods Studies (GRAMMS) checklist, 13 ensuring transparency and completeness in describing both quantitative and qualitative components. The study was conducted from May 16 to August 30, 2023.
Source and study population
For the quantitative component, all adult asthma patients attending outpatient clinics in the selected public hospitals constituted the source and study population. For the qualitative component, clinical practitioners working in the same public hospitals during the study period were included as the source and study population.
Inclusion criteria
All patients with a physician-confirmed diagnosis of asthma who met the inclusion criteria were included in the study. Eligible participants were adults aged 18 years or older, on active follow-up, and receiving asthma treatment for at least 6 months. For the qualitative component, prescribers with more than 1 year of experience in asthma management at the study hospitals were included.
Exclusion criteria
Patients whose medical records contained incomplete or missing data, as well as those who declined to participate in the study, were excluded. Additionally, prescribers who were not directly involved in asthma care or who were unavailable during the study period were excluded.
Sample size and sampling procedure
A total of 312 patient medical records were included in the quantitative phase of the study. A formal sample size calculation was not performed because a census sampling approach was employed, whereby all patients who met the inclusion criteria during the data collection period were consecutively included. This approach was used to minimize sampling bias and to ensure comprehensive representation of asthma patients managed in the six selected hospitals during the study period. For the qualitative component, the number of prescribers was determined based on data saturation.
Data collection procedures and instrument
Data were collected after providing training to three pharmacy professionals on medical chart review using a structured data abstraction format and on conducting in-depth interviews based on a semi-structured interview guide. Written informed consent was obtained from patients and clinical practitioners prior to recruitment.
Quantitative instruments
A structured data abstraction tool was used to collect data from medical charts to assess prescribers’ adherence to GINA guidelines and the availability of anti-asthmatic medications. Data collected included sociodemographic characteristics (age, sex, residence, educational level, marital status, monthly income, and occupation) and clinical characteristics (history of cigarette smoking, current smoking status, asthma triggers, hospitalization, asthma exacerbations in the past year, comorbid conditions, asthma severity, and type of anti-asthmatic medication prescribed).
Asthma control test (ACT)
The ACT was used to measure asthma symptom control. It consists of five items assessing daytime symptoms, nighttime awakenings, activity limitation, rescue medication use, and patient-rated asthma control over the past 4 weeks. 10 Each item is scored from 1 to 5, resulting in a total score ranging from 5 to 25. Scores were categorized as controlled (20–25), partly controlled (16–19), and uncontrolled (5–15). The ACT has demonstrated good construct validity and internal consistency in a prior study conducted in Ethiopia. 11
Medication adherence reporting scale (MARs)
The Medication Adherence Reporting Scale is a 10-item questionnaire used to assess patient adherence to asthma medication. 12 The instrument has shown strong construct and criterion validity in previous studies. 25 Patient adherence was calculated as the mean score across all items and dichotomized using a cutoff value of 3.73. Scores ⩾3.73 indicated good adherence, while scores <3.73 indicated poor adherence.
Prescriber adherence to the GINA guidelines was assessed using a structured, stepwise methodology. Adherence to the GINA 2023 guidelines was evaluated using predefined clinical indicators derived from the guideline recommendations. Specifically, adherence was assessed across the following components: (1) appropriateness of stepwise pharmacologic therapy based on asthma severity and level of control; (2) selection of recommended controller and reliever medications; (3) appropriateness of prescribed dose and dosing frequency by converting in to beclomethasone HFA equivalent doses; and (4) alignment of treatment regimens with GINA-recommended treatment steps. Prescriber adherence was defined as concordance between the prescribed regimen and the corresponding GINA 2023 treatment step for each patient.
Qualitative instruments
A semi-structured interview guide was developed to explore prescribers’ knowledge, awareness, and perceived barriers to adherence to GINA guidelines. The guide was developed through a review of relevant literature14,15 and pilot-tested with a small group of prescribers to ensure clarity and relevance. It was translated into Amharic and back-translated into English by independent experts to ensure accuracy and consistency. All questions were open-ended to facilitate in-depth exploration of participants’ experiences and perspectives.
Operational definition
Asthma symptom control implies the extent to which the various manifestations of asthma are reduced or removed by medication.
Adherence to GINA guidelines: Adherence to guidelines is the degree to which a practitioner’s behavior corresponds with the collaborative agreed recommendations from GINA, 2023.
Adherence to medication: it indicates the behaviors of patients who take a medication properly according to prescription. 16
Data processing and analysis
Quantitative analysis
Data were entered and analyzed using SPSS version 27 after checking for completeness and consistency. Descriptive statistics, including frequencies, percentages, means, and standard deviations, were used to summarize dependent and independent variables. Overall adherence rates to GINA guidelines, patient medication adherence, and availability of prescribed anti-asthma medications were calculated. Prescriber adherence rates were also computed for each asthma severity category.
Ordinal logistic regression was applied to examine factors associated with asthma symptom control, categorized as uncontrolled, partly controlled, and controlled. Bivariate ordinal logistic regression was initially performed, and variables with a p-value < 0.20 were included in the multivariable model. In the final multivariable ordinal logistic regression analysis, statistical significance was set at p < 0.05. Independent variables included sociodemographic factors (e.g., monthly income, marital status), clinical factors (e.g., asthma severity), and medication-related factors (e.g., type of medication prescribed, patient adherence, and prescriber adherence to GINA guidelines). Multicollinearity diagnostics and the proportional odds assumption were assessed to ensure model validity.
Qualitative analysis
For the qualitative component, all in-depth interviews were audio-recorded, transcribed verbatim, and reviewed multiple times for accuracy. Interviews conducted in Amharic were translated into English, with back-translation performed to ensure consistency of meaning. Data were analyzed using thematic analysis. Initial open coding was conducted manually, followed by grouping codes into categories and themes. To enhance reliability, two researchers independently coded the data, and discrepancies were resolved through discussion until consensus was achieved. Data saturation was confirmed when no new themes emerged. Two major themes were identified: challenges to prescriber adherence (including limited awareness, resource constraints, and workload issues) and prescribers’ knowledge and familiarity with the GINA guidelines.
Results
Sociodemographic characteristics of patients
The study population was predominantly middle-aged, with the highest proportion falling between 41 and 50 years (32.1%), while only 7.4% were above 61 years. Males slightly making up 54.8% of participants, and 81.4% of participants resided in urban areas. In terms of household income, the largest segment earned between 5501 and 7000 ETB (29.5%), whereas only 18.9% reported earnings above 7001 ETB. Related to educational attainment, 29.5% and 29.2% finished higher education and primary school, respectively. Marital status revealed that most respondents were married (43.6%). Government employees formed the largest occupational group (33%), compared to housewives who accounted for just 11.5%. Concerning household energy, slightly half of the participants reported not using biofuels as an energy source (53.2%); among those who use biofuels, charcoal (19.2%) was the most common fuel, while kerosene (2.2%) was the least. 90.1% of participants had no history of smoking, and only 4.2% were current smokers (Table 1).
Sociodemographic characteristics of adult patients with Asthma attending Public Hospitals found in South Gondar Zone, Amhara region, Ethiopia, 2023 (N = 312).

Clinical characteristics and medication-related information of the patients
Among the participants, 43.3% of participants had a severity of asthma were moderate persistent asthma, while severe persistent asthma was the least common (14.1%). In terms of hospitalization history within the past year, the majority of patients had not been admitted (85.9%). Regarding treatment, the most frequently prescribed regimen for treatment of asthma was low-dose beclomethasone inhalation daily for a month combined with salbutamol as needed (25.3%), while the least prescribed was low-dose budesonide with formoterol inhalation daily for a month (8.3%). Availability of prescribed medications revealed that unavailability was more frequently reported (56.4%). With respect to adherence, most patients adhered to their treatment regimens (58%; Table 2).
Clinical characteristics of the patients with asthma attending the Public Hospitals of South Gondar Zone, Amhara Region, Ethiopia, 2023 (N = 312).

Adherence of prescribers to guideline
Out of the total prescriptions reviewed, 57.7% (n = 180) did not adhere to the established guideline. In contrast, only 42.3% (n = 132) were found to be in alignment with the recommended standard (Figure 1).
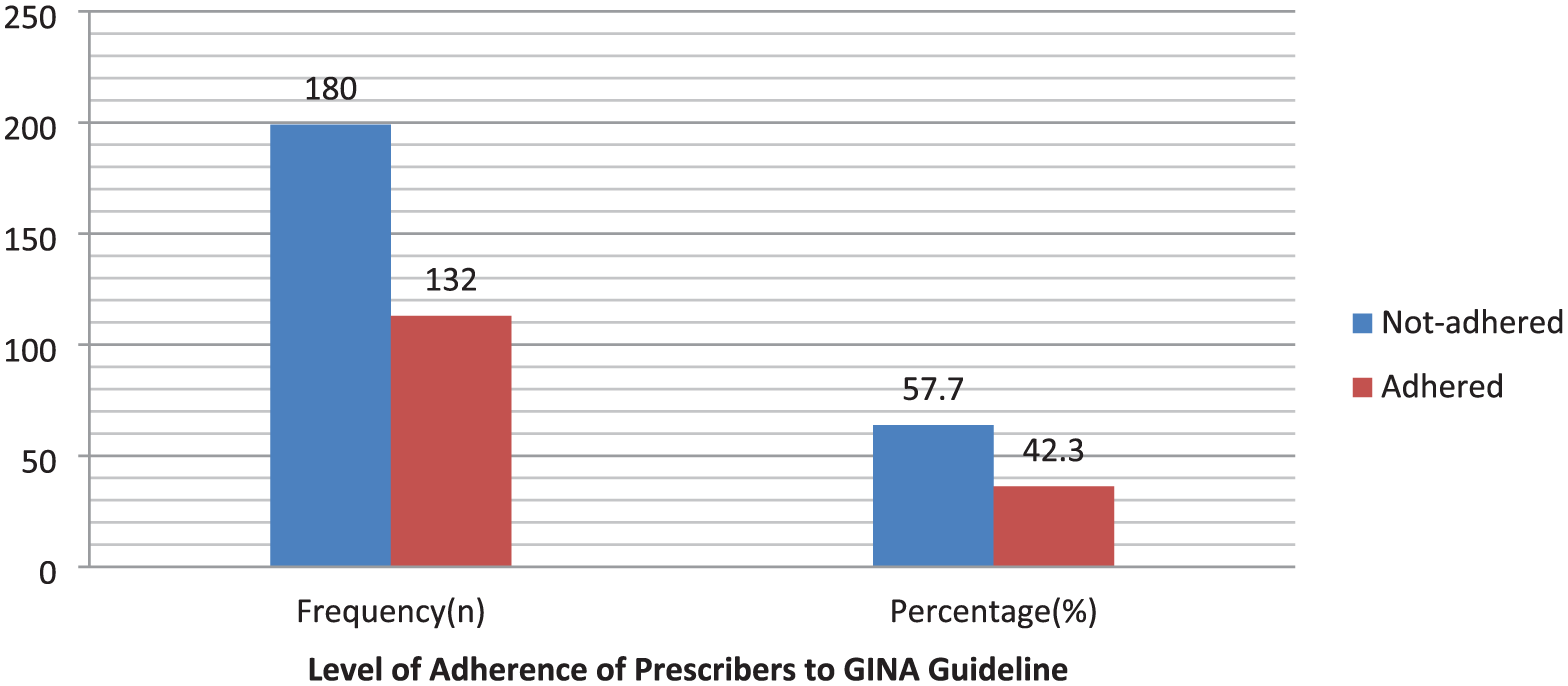
Practitioner adherence to prescribed medication according to the GINA asthma guideline for asthma patients visiting public hospitals found in South Gondar Zone, Amhara Region, Ethiopia, 2023.
Commonly violated GINA recommendations
The figure shows that the most common violation of GINA guidelines was omission of LABA in combination with inhaled corticosteroid, accounting for nearly half of all violations (46.1%). This was followed by prescribers omitting both doses of medication and without LABA (23.9%), inappropriate medication use (16.7%), and missing both dose and frequency of medications (13.3%; Figure 2).

Commonly violated GINA recommendations by prescribers for asthma patients visiting public hospitals found in South Gondar Zone, Amhara Region, Ethiopia, 2023.
Asthma symptoms control on patient with asthma medications
Asthma symptom control among 312 patients shows that 28% of patients have uncontrolled asthma, 51% have partly controlled asthma, and 21% have controlled asthma among patients visiting hospitals (Figure 3).

Asthma control level of patients visiting the public hospital found in South Gondar Zone, Amhara Region, Ethiopia, 2023.
Factors that affect asthma symptom control
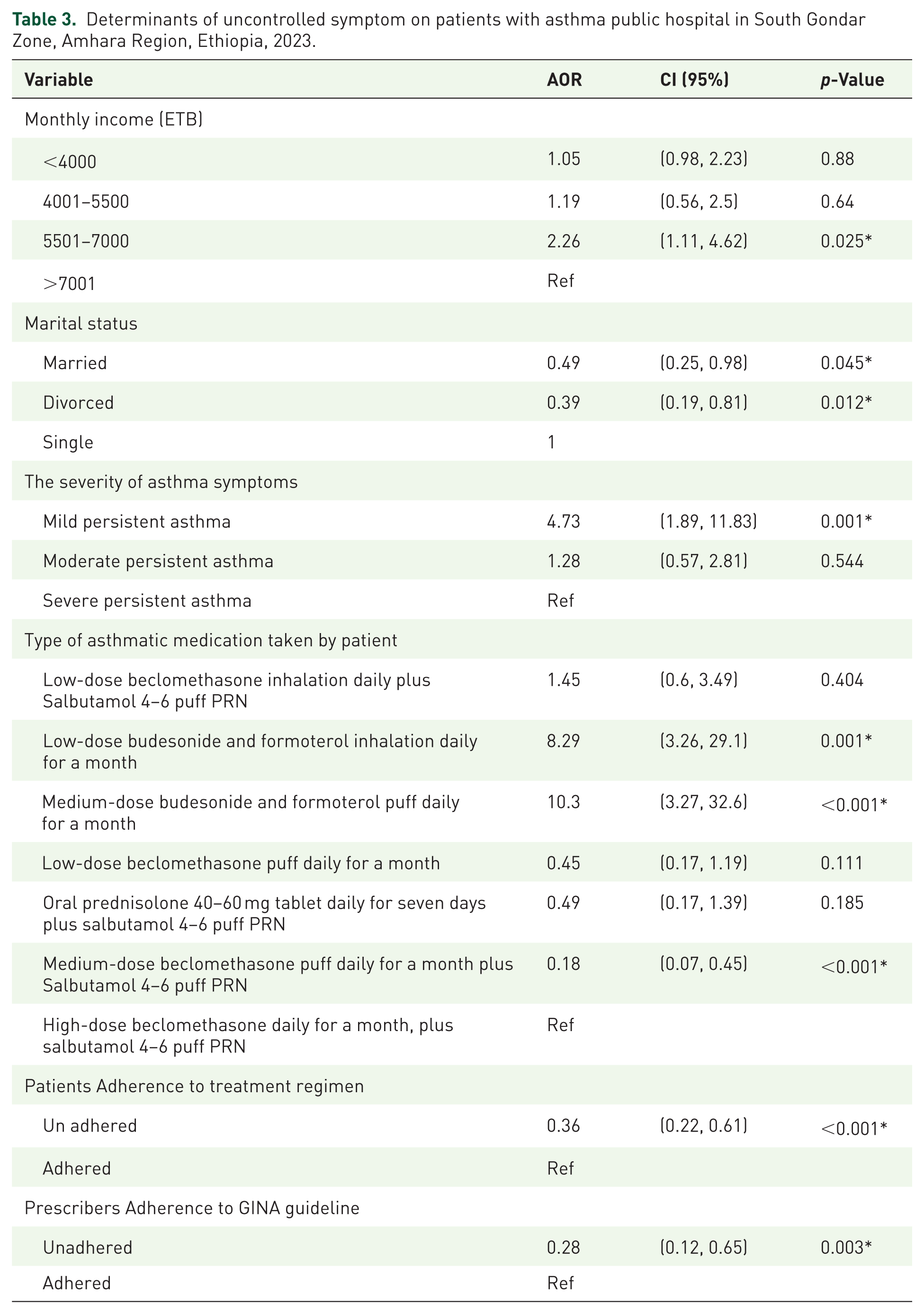
Patients with a monthly income of 5501–7000 ETB had more than twice the odds of achieving better asthma control compared with those earning above 7001 ETB (AOR = 2.26, 95% CI: 1.11, 4.62, p-value = 0.025). Married and divorced marital status was significantly associated with lower odds of symptom control compared with single status, married individual had 51 % (AOR = 0.49, 95% CI: 0.25–0.98, p-value = 0.045) and divorced one had 61% (AOR = 0.39, 95% CI: 0.19–0.81, p-value = 0.012) lower odds of symptom control compared with single participants. Mild persistent asthma was associated with significantly higher odds of good control compared with severe persistent asthma (AOR = 4.73, 95% CI: 1.89, 11.83, p-value = 0.001). Patients using low-dose budesonide and formoterol and medium-dose budesonide with formoterol inhalations daily for a month had 8 times (AOR = 8.26, 95% CI: 3.26–29.1, p-value = 0.001) and 10 times (AOR = 10.3 CI = 3.27, 32.6, p-value ⩽ 0.001) had a good control of symptoms compared with those on high-dose beclomethasone inhalation daily. Conversely, patients treated with medium-dose beclomethasone puff daily for a month plus salbutamol 4–6 puff PRN (AOR = 0.18 CI = 0.07, 0.45, p-value ⩽ 0.001) had lower odds of asthma control than patients receiving high-dose beclomethasone inhalation daily for a month. Non-adherent patients had significantly lower odds of achieving asthma control than adherent patients, with about 60%reduced likelihood (AOR = 0.36, 95% CI: 0.22, 0.61, p-value ⩽ 0.001). Prescriber adherence to the GINA guideline emerged as the strongest predictor. Patients managed by prescribers who did not adhere to the guideline had 72% lower odds of achieving good asthma control (AOR = 0.28, 95% CI: 0.12, 0.65, p = 0.003; Table 3).
Determinants of uncontrolled symptom on patients with asthma public hospital in South Gondar Zone, Amhara Region, Ethiopia, 2023.
Qualitative findings
Participants
A total of 18 practitioners were approached between August 10 and 30, 2023, of whom 11 consented and met the inclusion criteria (10 male, 1 female). Seven were excluded due to lack of consent or not meeting eligibility criteria. Participants’ ages ranged from 25 to 34 years. One participant was a specialist in internal medicine, while the remaining 10 were general practitioners. Their work experience ranged from 1 to 7 years.
Theme 1: Familiarity with GINA guidelines
Most practitioners reported being aware of the existence of the GINA guidelines; however, familiarity did not necessarily translate into routine use in clinical practice. Practitioners often referred to the guidelines only occasionally or in specific situations, such as managing refractory asthma cases.
One practitioner explained: Yes, I am familiar. But that does not mean I used the GINA guideline as a basic guideline for the diagnosis and management of patients’ health conditions. (Cp-7)
Another practitioner noted limited use in practice: I don’t use it heavily; I would refer to it once a week. Most of the time I refer to the guideline to treat patients with refractory asthma. (Cp-6)
Theme 2: Challenges to prescriber adherence to GINA guidelines
Practitioners identified several barriers that hindered consistent adherence to the guidelines. These challenges were categorized into three subthemes:
Subtheme 2a: Broadness and complexity of the guidelines
Participants reported that the comprehensive and detailed nature of the GINA guidelines made them difficult to apply quickly during routine clinical care.
GINA guidelines are so broad that it is difficult to summarize them in a short period of time and use in clinical practice day to day. (Cp-13)
Subtheme 2b: Unavailability of recommended medications
A major barrier was the lack of essential asthma medications in hospitals, which limited prescribers’ ability to follow guideline-based recommendations. Several practitioners emphasized that patients could not afford private purchase, leading physicians to rely on cheaper and available alternatives: The majority of medications used to treat asthma are not available in hospitals, particularly inhaled corticosteroids combined with long-acting beta agonists. Patients are often unable to purchase them from private pharmacies due to cost, so we prescribe the cheapest available alternatives. (Cp-7)
Subtheme 2c: Lack of awareness and training
Practitioners reported insufficient formal training on the GINA guidelines during both undergraduate education and continuing professional development. In addition, there was little institutional emphasis on guideline use: During our medical education, we received little to no training on GINA, and we were not encouraged by our trainers to use the guideline. (Cp-10)
Discussion
The primary aim of the GINA guidelines is to standardize and improve asthma diagnosis and treatment. The findings of this study revealed that adherence to GINA guidelines among practitioners in the hospitals studied was suboptimal, with only 42.3% of patients receiving medications aligned with guideline recommendations. This highlights a significant gap in the delivery of guideline-based asthma care. Comparisons with previous studies show variability in adherence rates: a study reported in Italy 79% adherence rate 17 and in Nigeria reported 59.1% adherence 18 and in Italy, which is higher than our finding and may reflect differences in resource availability or methods for assessing prescriber adherence, a study in Italy reported a lower rate of 28%, 19 this difference might be potentially suggest that differences in healthcare infrastructure, sample size, and prescriber assessment methods influence findings. These discrepancies highlight the influence of local healthcare infrastructure, resource availability, and methodological approaches on guideline implementation. Resource limitations, unavailability, and unaffordability of essential medications were identified as major barriers to adherence. Key informants noted that medications for moderate and severe persistent asthma, particularly those containing long-acting beta-agonists (LABA), were often unavailable or financially inaccessible to patients. Such constraints highlight the impact of local healthcare infrastructure on the practical implementation of GINA guidelines and patient access to appropriate care.
Provider adherence to GINA guidelines was strongly associated with improved asthma outcomes. Patients treated by prescribers who followed guidelines had higher odds of achieving effective symptom control, whereas those managed by non-adherent providers experienced higher rates of uncontrolled asthma. International evidence supports this statement; a study from Italy 19 demonstrates that adherence to guideline-based prescribing improves symptom control, reduces emergency visits, and optimizes patient outcomes. Beyond clinical benefits, guideline adherence also offers economic advantages: by reducing exacerbations and severe episodes, it decreases hospitalizations, emergency department visits, and the need for urgent medications, a consideration particularly relevant in low- and middle-income countries where asthma imposes substantial financial burdens on families and healthcare systems. Qualitative findings provided further insight into barriers to adherence. The broad scope and complexity of the GINA guidelines were reported as challenging for routine use in busy clinical settings, making rapid decision-making difficult. Limited availability and high cost of essential medications forced patients to rely on private pharmacies, often at unaffordable prices. In addition, inadequate training and continuing education on updated GINA guidelines constrained prescribers’ ability to apply best practices. These factors collectively impact both individual patient care and broader public health outcomes, emphasizing the need for targeted interventions to improve guideline uptake.
Other determinant symptom control: The study found that individuals with a monthly income of 5501-7000 ETB had significantly higher odds of better asthma outcomes compared to those earning >7001 ETB. However, this contrasts with some studies that suggest higher income is generally associated with better asthma symptom control.20,21 One possible explanation for this inconsistency is that higher-income patients in our study had worse asthma symptom control; patients in the middle-income bracket may allocate more resources toward essential medications and regular clinic visits compared to higher-income patients, who may be more mobile, busier, or less adherent to daily controller therapy, all of which can impair asthma control.
Disease severity was another determinant of outcomes; patients with mild persistent asthma were more likely to achieve good control than those with severe persistent asthma. Severe asthma is characterized by persistent symptoms, frequent exacerbations, reduced lung function, corticosteroid resistance, and comorbidities, which together reduce responsiveness to standard therapies and complicate management. 22 The findings of this study indicate that patients using low-dose budesonide/formoterol and medium-dose budesonide/formoterol combination inhalations daily for a month had significantly better asthma control, with 8- and 10-fold higher odds of good symptom control compared to those on high-dose beclomethasone/salbutamol combination inhalation. This aligns with global evidence showing that combination therapy with budesonide and formoterol improves asthma control more effectively than simply increasing the dose of inhaled corticosteroids. 23 Studies have demonstrated that budesonide/formoterol therapy enhances lung function, reduces exacerbation rates, and provides better overall symptom management, supporting its use as both maintenance and reliever therapy. 24
Finally, the current study found that patients who did not adhere to their prescribed asthma medications had significantly lower odds of achieving asthma control compared to adherent patients. This finding is consistent with evidence from various studies demonstrating that poor medication adherence is strongly associated with uncontrolled asthma. A multicenter study in Northwestern Ethiopia reported that non-adherence was associated with a reduction in the odds of symptom control. 25 Similarly, research from Eastern Ethiopia found that patients with poor adherence were more than twice as likely to have uncontrolled asthma. 26 Non-adherence reduces the effectiveness of therapy and result increases the risk of exacerbations, frequent hospitalizations, and decreased quality of life. 16 The pharmacological rationale is clear: without regular use, inhaled corticosteroids and other controller medications cannot exert their anti-inflammatory effects, leading to poor symptom control. Importantly, interventions such as patient education, adherence counseling, and support programs have been shown to improve adherence and, consequently, asthma outcomes. 27 These findings highlight the critical role of adherence in effective asthma management and underscore the need for strategies to promote consistent medication use among patients.
Conclusion
Only 42.3% of prescribers adhere to GINA standards. There is a strong link between non-adherence to GINA guidelines and poorer asthma symptom management. Patients with a monthly income of 5001 to 7000 ETB, asthma severity level being the mild persistent level of asthma, medication taking low-dose budesonide/formoterol inhalation, and medium-dose budesonide/formoterol inhalation are major positive factors influencing asthma control. Uncontrolled asthma, on the other hand, was found to be strongly associated with the use of particular medications with a specific dose (medium-dose beclomethasone with salbutamol inhalation), prescribers’ non-adherence with GINA guidelines, and patient non-adherence to prescribed therapy. Reasons for non-adherence of GINA guideline by prescribers that identified were broadness of the scope of the GINA guidelines, difficulties in getting medications recommended by guideline by patients, and lack of training were identified as significant causes of non-adherence to GINA guidelines by prescribers. To control asthma symptoms for patients and improve health outcomes, the findings of this study highlight the necessity of GINA guidelines adherence, improve prescriber training, and increase access to necessary medications.
Recommendation
The findings show that stronger prescriber adherence to GINA guidelines is necessary to improve asthma management and patient outcomes. It is crucial to set up continuing professional development (CPD) programs that provide structured and up-to-date training on the practical implementation of GINA guideline recommendations to make sure prescribers are aware of changes and can apply them to their everyday work activity. GINA recommendations may also be streamlined and tailored at the institutional and national levels to facilitate their application in high-stress clinical situations. Efforts should be made to improve the availability and affordability of necessary asthma medications, particularly inhaled corticosteroid combinations with long-acting beta2 receptor agonist (ICS/LABA combination medicines), by improving supply chain management and adding them to lists of essential medicines for healthcare facilities. Since both prescriber and patient adherence are necessary for the best results, patient-centered education and counseling should be improved to increase patient adherence to recommended medications. Furthermore, system-level measures such as mentorship, frequent clinical audits, and incorporating adherence to guidelines into quality assurance frameworks may encourage accountability and long-term practice improvement.
Strength and limitation
This study provides valuable insights into prescribers’ perspectives on non-adherence to GINA guidelines in a resource-limited setting with incomplete data. Only prescribers’ opinions were included; the perspectives of administrators and pharmacists, who may also influence adherence, were not captured. In addition, potential biases such as selection bias, reliance on self-reported adherence, and unavailable medication stock data may have affected the findings. Addressing these limitations helps contextualize the results and provides a clearer understanding of factors influencing guideline adherence.
For future research
To obtain a more comprehensive understanding of the barriers to GINA adherence, future research should include the perspectives of pharmacists and health system administrators, as their insights can reveal system-level and interdisciplinary challenges. The generalizability of findings would also be strengthened if studies were conducted across multiple locations and diverse types of healthcare facilities. Moreover, intervention-based research, such as piloting training programs or other practical strategies, is needed to test and identify effective methods for improving adherence to asthma management guidelines.
Supplemental Material
sj-pdf-1-tar-10.1177_17534666261436694 – Supplemental material for Prescriber adherence to asthma treatment guidelines and its impact on symptom control in Ethiopia: a mixed-methods study
Supplemental material, sj-pdf-1-tar-10.1177_17534666261436694 for Prescriber adherence to asthma treatment guidelines and its impact on symptom control in Ethiopia: a mixed-methods study by Abraham Nigussie Assefa, Muluken Adela Alemu, Tesfaye Yimer Tadesse, Amanuel Tadesse Aklog, Getachew Yitayew Tarekegn, Tilaye Arega Moges and Samuel Berihun Dagnew in Therapeutic Advances in Respiratory Disease
Footnotes
Acknowledgements
We would like to thank hospital administrative for their collaboration during conducting this research. Our gratitude also goes to our data collectors and study participants for their willingness to participate in the study. We would like to forward our special thank and sincere appreciations to our friends who gave advice and comment throughout the whole research activities.
Declarations
Supplemental material
Supplemental material for this article is available online.
Publisher’s note
The authors alone make all of the claims made in this article; the publisher, editors, reviewers, and any related organizations do not necessarily endorse them.