
Abstract
Mesenchymal chondrosarcoma is a malignant tumor that arises from cartilage-forming cells and typically affects the bones, but in rare cases also the lungs. Due to its rarity, there is limited knowledge about the clinical presentation, diagnostic challenges, and treatment options for primary pulmonary chondrosarcoma. We conducted a comprehensive literature search through PubMed, EMBASE, Scopus, Clinical Trial Gov, and Google Scholar using search terms such as “primary pulmonary/lung chondrosarcoma.” We also present our case study. In our case, the chondrosarcoma was discovered incidentally during a Computer Tomography (CT) scan. It was located in the middle lobe and was historically characterized as low-grade. After surgical removal, no recurrence was detected during follow-up examination. In the literature reviewed, the most common symptoms of primary pulmonary chondrosarcoma were cough and dyspnea. Radiologic features included well-defined margins, a central location, and calcifications. Histopathological examination revealed either hyaline or myxoid structures, with the myxoid type being more aggressive. Surgical resection is currently the preferred treatment method with a recurrence rate of approximately 21%.
Primary pulmonary mesenchymal chondrosarcoma remains a rare and challenging diagnosis, typically presenting with non-specific symptoms. Surgical resection is the primary treatment method. Further research is needed to establish standardized diagnostic criteria and treatment protocols.
Points for clinical practice
- Primary Pulmonary Chondrosarcoma is a rare lung tumor with no specific symptoms.
- Radiologically, calcifications and a central location may be indicative of this condition.
- Surgical resection is the preferred treatment method.
Introduction
Primary pulmonary mesenchymal chondrosarcoma is a rare malignant cartilage tumor that originates in the lung or occurs as a metastasis of a primary bone chondrosarcoma. It is characterized by the formation of neoplastic cartilage and differs from other sarcomas in its slow growth and resistance to conventional chemotherapy and radiotherapy. While primary pulmonary chondrosarcoma is extremely rare, metastatic lung involvement is more commonly observed in advanced chondrosarcomas originating in the axial skeleton and craniofacial bones. 1
The diagnosis of pulmonary chondrosarcoma is challenging due to its radiologic and histopathologic features, which overlap with those of other lung tumors. Although mesenchymal chondrosarcoma mainly affects teenagers and young adults, it can occur at any age, and neither sex is particularly predisposed to this disease.2,3 Early detection and appropriate surgical intervention remain the mainstay of treatment, as these tumors usually respond only to a limited extent to systemic therapies. In this article, we will first describe our case and then summarize the existing literature on pulmonary chondrosarcoma, including its clinical presentation, diagnostic modalities, and therapeutic approaches.
Case report
We would like to present a 52-year-old Caucasian male patient, who has been treated at our department since 2021 for Obstructive Sleep Apnea Syndrome (OSAS). Comorbid conditions include Stage I/A Chronic Obstructive Pulmonary Disease (COPD), diabetes mellitus, and obesity. A Pulmonary mass was first detected in 2020 during a High-Resolution Computed Tomography (HRCT) scan performed to evaluate parenchymal changes following COVID-19 (Figure 1). At the time of presentation in February 2024, the patient reported no significant respiratory impairment, no fever, and no weight loss. The new CT scan was performed to re-evaluate the existing pulmonary mass. Until 2024, the most significant finding had been a nodular lesion measuring approximately 2–3 mm located on the anterior wall of the right intermediate bronchus (Figure 2). A biopsy was taken by bronchoscopy, although the lesion was extremely hard when cut with the forceps (Figure 3). Histopathological examination revealed the presence of an atypical cartilage tumor with increased cell density, cellular atypia of the chondrocytes with loosening in chromatin structure and binucleated cells, embedded in hyaline cartilage matrix. It was classified as a low-grade chondrosarcoma (Figures 4(a) and (b)). A CT scan of the abdomen and a bone scintigraphy revealed no other organ involvement. Subsequently, a radical mediastinal lymphadenectomy and lobectomy with bronchial cuff resection were performed thoracoscopically. Follow-up examinations, including bronchoscopy at 1 month, CT scan at 6 months, and clinical evaluation at 12 months after surgery, demonstrated good postoperative healing with no signs of recurrence (Figures 5(a) and (b)).

CT scan from COVID-19 infection in 2020.

CT scan from March 2024.

Bronchoscopic view of the lesion in the bronchus intermedius.
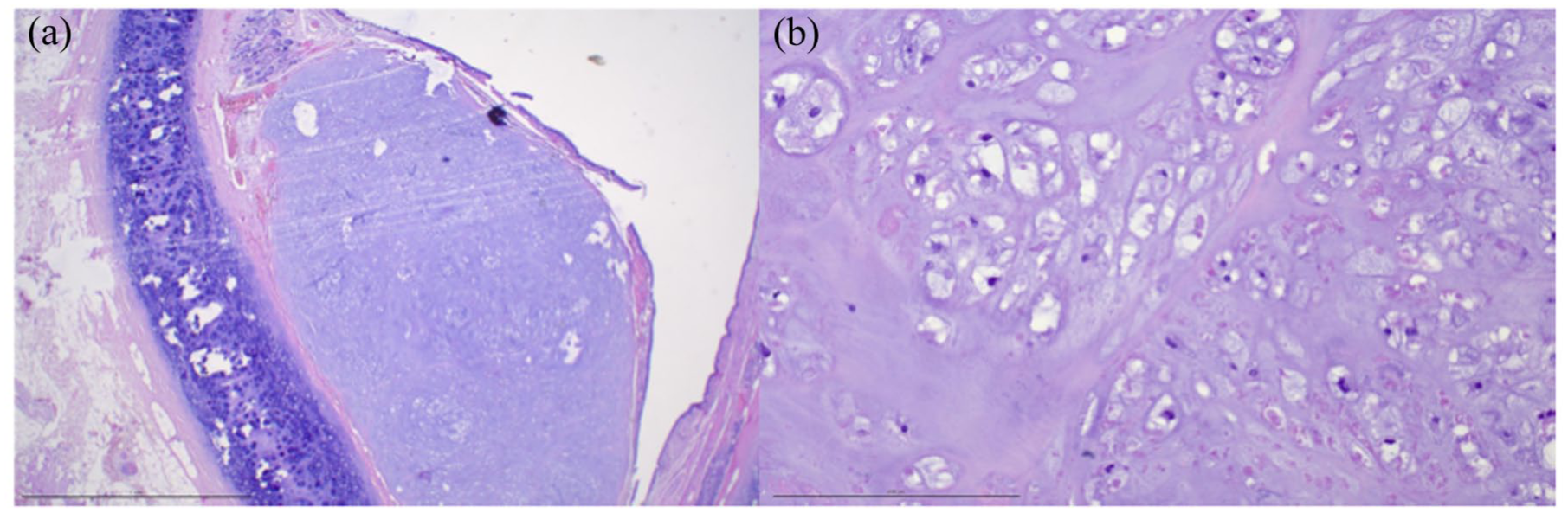
(a, b) Representative images of biopsy and resection specimen. Images Hematoxylin and Eosin stain, original magnification 4× and 20×. The tissue is composed of well-differentiated cartilaginous matrix with mild to moderate cellular atypia. The chondrocytes show enlarged nuclei and some binucleated chondrocytes. There is no significant nuclear pleomorphism.

(a, b) Postoperative bronchoscopy in 1 month and CT scan 6 months after surgery.
Methods
The literature search was conducted independently by two authors (CM and YM) using databases of PubMed, SCOPUS, Clinical Trial gov, EMBASE, and Google Scholar with the terms “primary AND pulmonary OR lung AND chondrosarcoma” in the abstract, the title, or the keywords. The survey produced 971 articles with the last access date August 5, 2025. After removing duplicates, titles and abstracts were screened by two independent reviewers (AP and DG) After initial screening based on title and abstract, 42 articles were found eligible. We only included articles written in english and/or german language. Articles with a focus on primary pulmonary chondrosarcoma were reviewed. Articles dealing with tracheal chondrosarcoma or vascular chondrosarcoma, or myxoid sarcoma were excluded. The search strategy is shown in Table 1. After reviewing these manuscripts, three additional suitable articles were included. A total of 45 articles were found to be eligible and included in this systematic review, as analyzed in Table 2. The reporting of this study conforms to the CARE checklist (see Supplemental Material). 4
Searching strategy.

Three additional articles were found through search of the included articles.
Data from included studies.

LLL, Left Lower Lobe; LUL, Left Upper Lobe; M, Man; ML, Middle Lobe; RLL, Right Lower Lobe; RMB, Right Main Bronchus; RUL, Right Upper Lobe; W, Woman.
Review of the literature
Historically
The first case described in the literature as “primary osteoid chondrosarcoma of the lung” was published in 1933 by Edward B. Greenspan from the Laboratories of the Mount Sinai Hospital in New York. 5 However, Hamilton Roe had already described a case similar to Greenspan’s in 1866, involving a lung tumor with «nucleated and granular cells imbedded in a dense fibrous matrix» in a 23-year-old patient who had died of cachexia and chronic productive cough. 6 In 1968, Dume and Hueber, and shortly afterwards in 1970, Rees made the first attempts at a literature review together with the presentation of their cases.7,8 But it was not until 1972 that Morgan and Salama presented an overview of seven case reports together with data on gender, age, presenting symptoms, tumor progression, and surgical treatment, follow-up care, location, size, and spread of the tumor. 9
Age, gender, comorbidities, presenting symptoms
54% of the patients were male (25/46) with a median age of 52 years (20–83). Cough (45%) was the predominant symptom in most cases, followed by dyspnea (32%), chest pain (26%), haemoptysis (24%), and weight loss (8%) were the most common symptoms leading to a medical consultation. This could be explained by the fact that the tumor is usually large and centrally located. However, in 26% of the case reports, pulmonary chondrosarcoma was the incidental finding on chest X-ray or a CT scan performed for other reasons.
Radiologic features
Radiologic assessment plays a crucial role in the diagnosis of pulmonary chondrosarcoma. CT and magnetic resonance imaging (MRI) are commonly used to assess the size, location, and characteristics of the tumor, including calcifications that indicate a cartilaginous origin. In some cases, the tumor is discovered incidentally during imaging procedures performed for other conditions.10,11
A brief analysis of the included studies revealed that in 28% of patients, the tumor was located in the left upper lobe and the average size was approximately 7 cm (see Table 2). Most of the case-studies showed a central location of the tumor,7,11–37 while a few showed a peripheral lesion.8,9,38–47 Further reports suggest that calcifications may be indicative of pulmonary chondrosarcoma, 26 whereas pleural effusion, although uncommon, is sometimes associated with tumor-induced atelectasis of a lobe. 31,45,48
In the MRI, the tumor appears to have moderate signal intensity on T1-weighted images and high signal intensity weighted images on T2-weighted images, which could be considered as a bronchogenic cyst in differential diagnosis. 19
However, it is imperative to screen for extrapulmonary metastases using abdominal CT and bone scintigraphy with Tc-99m. The use of Positron Emission Tomography (PET)/CT to detect possible metastases is not specifically addressed in the literature. However, according to a meta-analysis by Zhang et al, the sensitivity and specificity of Fludeoxyglucose F 18 (18F-FDG)-PET/CT in the staging of chondrosarcomas are 94% and 89%, respectively. 49
Differential diagnosis
In patients with clinical symptoms and radiological signs of a pulmonary mass, it is crucial to rule out common forms of lung cancer by means of bronchoscopic, CT-guided, or Video-Assisted Thoracoscopic Surgery (VATS) biopsy. The definite diagnosis of primary pulmonary chondrosarcoma requires: (1) a thorough clinical history excluding: (a) previous skeletal tumors, (b) limb amputations, and (c) teratomas, (2) a neoplasm of the chest and the Carney triad—pulmonary chondroma, gastrointestinal stromal tumor, and extra-adrenal paragangliomas—must be carefully excluded, 50 and (3) all cases must be confirmed histologically.26,51
Histopathologic findings
Chondrosarcoma accounts for approximately 20%–27% of all primary bone sarcomas, but primary pulmonary chondrosarcoma is extremely rare. 10 The etiology of this tumor remains unclear, although genetic mutations in the Isocitrate Dehydrogenase 1 (IDH1), IDH2, and Collagen type II Alpha 1 chain gene (COL2A1) have been linked to its pathogenesis. 52 The tumor arises from cartilaginous elements and can either develop de novo or result from the malignant transformation of an existing benign cartilage lesion, such as an enchondroma or osteochondroma. 53
Two types of pulmonary chondrosarcoma have been described in the literature: the hyaline and the myxoid type. The hyaline type has well-differentiated cells with hyperchromasia and no mitotic activity, while the myxoid type appears to be more aggressive and is characterized by a biphasic morphology, with islands of neoplastic hyaline cartilage, occasionally calcified, mixed in with small, round, undifferentiated cells. 51 An examination of myxoid chondrosarcoma reveals an abnormal proliferation of small, spherical blue cells that are packed together into nests and strands and a characteristic translocation of t(9:17)(q22;q11.2) or EWSR1-NR4A3 fusion. This type of myxoid sarcoma will not be described in detail here, as it lies outside the scope of the present review.
The neoplastic cells show in immunohistochemical staining no reaction for cytokeratin AE1/AE3, Anti-Cytokeratin Mouse Monoclonal Primary Antibody (CAM5.2), synaptophysin, chromogranin, Thyroid transcription factor-1 (TTF-1), napsin A, Platelet endothelial cell adhesion molecule (PECAM-1), also known as cluster of differentiation 31 (CD31), p40 and desmin and sometimes a positive reaction for S-100.3,26
The differential diagnosis appears to be rather limited due to the characteristic form of the tumor. However, small biopsies can be interpreted in a broader spectrum of differential diagnoses, such as small cell carcinoma, rhabdomyosarcoma, neuroblastoma, Ewing’s sarcoma, and even histological variations of synovial sarcoma, solitary fibrous tumor, and osteosarcoma with small round cell morphology. 54 The key component is the result of a multiplex Polymerase Chain Reaction (PCR) test targeting specific gene fusions and rearrangements associated with mesenchymal chondrosarcomas that have a recurrent HEY1::NCOA2 gene fusion, which produces an mRNA product with an in-frame fusion of NCOA2 exon 13 and HEY1 exon 4. 3
Therapy and outcome
The prognosis of pulmonary chondrosarcoma depends largely on the histological grade and extent of disease at the time of diagnosis. Low-grade tumors show relatively favorable results with surgical treatment, while high-grade variants have a higher tendency to metastasize and recur. 55
Most patients (80%) underwent surgical treatment. Table 2 details whether additional treatment methods, such as radiotherapy or chemotherapy, were performed before or after surgery. The recurrence rate was approximately 21% and the average time to recurrence was 21 months, but these data should be interpreted with caution, as many authors do not provide such detailed follow-up data on their patients after the surgery. Complete surgical removal, such as lobectomy or pneumonectomy, is often necessary to achieve negative margins. 56 Unlike many other malignant tumors, chemotherapy and radiotherapy have shown limited efficacy due to the inherent resistance of the tumor. However, new reports suggest chemosensitivity to IDH1 inhibitors, while other new therapies, such as PIK3-AKT-mTOR inhibitors or cell cycle inhibitors, appear promising. 57
Discussion
Pulmonary chondrosarcoma is a rare form of malignant tumor that originates from cartilage-producing cells and usually affects the bones, but in very rare cases, also the lungs, either as a primary tumor or as a metastasis from other areas of the skeleton. Due to its rarity, descriptions of the pathology come almost exclusively from case reports.
Many sources state that pulmonary chondrosarcoma mainly affects young adults, 26 but as shown in this review, it can occur at any age. The incidence of primary pulmonary chondrosarcoma is difficult to estimate, as its pathology is often misdiagnosed and requires a detailed medical history and diagnostic evaluation to rule out other primary causes; therefore, it may be underrepresented in the literature. Through our review, we found a slight predisposition for the development of pulmonary chondrosarcoma in middle-aged men (54% male; median age 52 years). The most common symptoms were cough (45%) and dyspnea (32%), with pulmonary chondrosarcoma being an incidental finding in 26% of cases during chest X-ray or CT scan, performed for other reasons, as was the case with our patient. This could indicate that chondrosarcomas do not frequently cause obstructive pneumonia, even though they are usually centrally located.
Radiologically, chondrosarcoma shares common features with other lung tumors in CT scans, but differs in its clearly defined margins, central location, and calcifications. 26 The central location and calcifications can be explained by the probable origin of the tumor in the cartilage tissue.
In the present case, histology revealed a spherical tumor formation consisting of a hyaline cartilage matrix with increased cell density. The chondrocytes showed significantly enlarged plum cell nuclei with a loosened chromatin structure and repeated binucleated cell elements. These findings are consistent with the descriptions in the literature. 51
To rule out extrapulmonary manifestations, further radiological examinations with abdominal CT and bone scintigraphy using Tc-99m are essential. The use of 18-FDG PET-CT to detect possible metastases is not specifically addressed in the literature, but could be a valuable alternative. 49
Surgical resection remains the primary treatment for localized pulmonary chondrosarcoma as radiotherapy and chemotherapy are only of limited effectiveness due to the low susceptibility of chondrosarcoma to these forms of therapy. Recently, targeted therapies based on molecular alterations have been investigated as possible treatment approaches. 57
Conclusion
Primary pulmonary chondrosarcoma is a rare tumor that is calcified, relatively large, and centrally located, which can occur with or without respiratory symptoms. Both a histopathologic diagnosis and the exclusion of other tumor-affected organs by imaging are essential for diagnosis. The treatment of choice is surgical removal.
In summary, further systematic reviews of case reports, or case series, and a multidisciplinary approach are needed to establish reliable diagnostic criteria and treatment recommendations.
Supplemental Material
sj-pdf-1-tar-10.1177_17534666251406045 – Supplemental material for Primary pulmonary chondrosarcoma: clinical case and review of the literature
Supplemental material, sj-pdf-1-tar-10.1177_17534666251406045 for Primary pulmonary chondrosarcoma: clinical case and review of the literature by Christopher Milacek, Yasmin Merza, Felicitas Oberndorfer, Konrad Hoetzenecker, Daniela Gompelmann, Marco Idzko and Anastasia Papaporfyriou in Therapeutic Advances in Respiratory Disease
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.