
Abstract
Background:
Noninvasive ventilation (NIV) is frequently employed for acute hypoxemic respiratory failure, yet optimal intubation timing for high-risk NIV failure patients remains uncertain.
Objectives:
To investigate mortality outcomes associated with early versus late intubation in high-risk NIV failure patients.
Design:
Secondary analysis of a multicenter observational cohort study.
Methods:
Patients with high NIV failure risk (updated HACOR score ⩾11 after 1–2 h of NIV) were enrolled. We defined that intubation was needed in these high-risk patients. Intubation occurring within 12 h of NIV initiation was classified as early intubation, while intubation after 12 h was designated as late intubation. Primary outcomes were intensive care unit (ICU) and hospital mortality. In sensitivity analyses, patients who achieved NIV success were categorized into the late-intubation group. Due to baseline imbalances, propensity score matching was performed with covariate adjustment.
Results:
Among the study population, 171 patients underwent early intubation and 222 underwent late intubation. Despite greater baseline severity in the early intubation group, ICU mortality (36% vs 58%, p < 0.001) and hospital mortality (38% vs 58%, p < 0.001) were significantly lower compared to the late-intubation group. In sensitivity analyses, 190 patients with NIV success were included in the late-intubation group, further accentuating the severity disparity between groups. After propensity matching (220 patients: 110 per group), most of the baseline characteristics were comparable. The early intubation group had a 100% intubation rate versus 71% in the late-intubation group, with the latter exhibiting higher mortality (ICU: 46% vs 32%, p = 0.052; hospital: 50% vs 34%, p = 0.020).
Conclusion:
In patients at high risk for NIV failure, early intubation is associated with reduced mortality.
Plain language summary
Many patients with severe breathing problems caused by low oxygen levels in the blood need respiratory support. Noninvasive ventilation is one of the main ways to give such support and help patients breathe easier. However, this treatment doesn’t always work. And if patients whose treatment fails don’t get more advanced treatment quickly, their chance of dying goes up even more. This study wanted to figure out the best time to step up treatment for these high-risk patients. We discovered that starting more advanced treatment within 12 hours could lower the death rate compared to starting it later.
Introduction
Acute hypoxemic respiratory failure (AHRF) represents a frequent clinical condition in intensive care units (ICUs).1,2 High-flow nasal cannula (HFNC) and noninvasive ventilation (NIV) serve as the primary modalities of noninvasive respiratory support for AHRF patients.3,4 Physiological studies have demonstrated that NIV produces significantly greater reductions in esophageal pressure compared with HFNC.5,6 Consequently, NIV is more frequently employed in AHRF patients exhibiting increased work breathing. Nevertheless, NIV failure rates remain substantial, ranging from 40% to 54%,7 –9 and such failure is associated with increased mortality.10,11 These findings underscore the importance of appropriate patient selection for NIV therapy.
The updated HACOR (Heart rate, Acidosis, Consciousness, Oxygenation, and Respiratory rate) scoring system demonstrates high predictive value for differentiating between successful and failed NIV outcomes in AHRF patients. 12 Patients achieving a score ⩾11 points after 1–2 h of NIV therapy are considered at high risk for treatment failure, with a high probability of requiring intubation. However, clinical decision-making regarding intubation timing shows considerable variability among physicians managing comparable cases. 13 While early intubation may result in unnecessary invasive procedures for some patients, delayed intubation carries the risk of patient self-inflicted lung injury. 14 This clinical dilemma highlights the current uncertainty surrounding optimal intubation timing. The present study aimed to investigate whether early intubation was associated with reduced mortality among AHRF patients identified as high risk for NIV failure based on HACOR criteria.
Methods
We conducted a secondary analysis of a multicenter prospective observational study (NCT03250416) with the aim of updating the HACOR score for predicting NIV failure. 12 This study was carried out in 17 hospitals in China and 1 hospital in Turkey from September 2017 to September 2021. A high risk of NIV failure was defined as an updated HACOR score of ⩾11 after 1–2 h of NIV. In the present study, we defined the need for intubation in these high-risk patients. Referring to previous studies, intubation within 12 h of starting NIV was defined as early intubation, while intubation occurring more than 12 h after starting NIV was defined as late intubation.15,16 The reporting of this study complies with the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guideline. 17
The inclusion criteria were as follows: (1) hypoxemic respiratory failure, (2) an updated HACOR score of ⩾11 after 1–2 h of NIV, (3) age >16 years. The exclusion criteria were as follows: (1) application of NIV following planned or unplanned extubation, (2) use of NIV due to acute exacerbation of chronic obstructive pulmonary disease, (3) use of NIV as a result of HFNC failure, (4) prior receipt of NIV for more than 2 h before admission to the participating center, (5) patients with treatment limitations (i.e., refusal of intubation despite need).
The indications for NIV were as follows: (1) tachypnea (respiratory rate >25 bpm), (2) clinical presentation of respiratory distress at rest (such as active contraction of the accessory inspiratory muscles or paradoxical abdominal motion), and (3) PaO2 <60 mmHg at room air or PaO2/FiO2 <300 mmHg with supplemental oxygen. The management protocol for NIV has been described previously. 12 In cases where respiratory failure showed progressive deterioration, intubation for invasive mechanical ventilation was carried out. Respiratory or cardiac arrest, PaO2/FiO2 <100 mmHg after NIV, requirement of intubation to protect the airway (coma or seizure disorders) or to manage copious tracheal secretions, and hemodynamic instability without response to fluids or vasoactive agents were major criteria for intubation. PaO2/FiO2 <150 mmHg after NIV, respiratory rate >35 bpm, lack of improvement in respiratory muscle fatigue, and acidosis with pH <7.35 were minor criteria for intubation. Intubation was considered when one major criterion or more than two minor criteria were met. However, the final decision to intubate was left to the discretion of the attending physician.
Data collection
Baseline demographic data were retrieved from the medical records. Heart rate, acidosis status, level of consciousness, oxygenation, and respiratory rate were measured before and 1–2 h after the initiation of NIV. Acidosis was evaluated based on the pH value. The level of consciousness was assessed by means of the Glasgow Coma Scale. Using these data, the HACOR score was calculated. 12 The updated version takes the original HACOR score and carries out the following operations: +0.5 × SOFA + 2.5 (if pneumonia is diagnosed) – 4 (if cardiogenic pulmonary edema is diagnosed) + 3 (if pulmonary acute respiratory distress syndrome (ARDS) is present) + 1.5 (if immunosuppression is present), and +2.5 (if septic shock is present) (Supplemental Table 1). Disease severity was evaluated using the Sequential Organ Failure Assessment (SOFA) score. The outcome measures included NIV failure, ICU mortality, in-hospital mortality, length of stay in the ICU, and length of hospital stay.
Statistical analysis
Data were analyzed using the Statistical Package for the Social Sciences (IBM SPSS Statistics, version 25.0). The Shapiro-Wilk test was employed to determine the distribution of continuous variables. For normally distributed continuous variables, Student’s t-test was utilized, and results were reported as means and standard deviations. In the case of non-normally distributed continuous variables, the Mann–Whitney U test was applied, with results presented as medians and interquartile range (IQR) values. Categorical variables were analyzed using the chi-square test or Fisher’s exact test, as appropriate. The crude and adjusted odds ratios of death in the ICU or hospital were also computed. Adjusted variables included age, sex, SOFA score, presence of septic shock, presence of ARDS, ICU types, diagnosis, underlying disease, vital signs, arterial blood gas test results, and updated HACOR score. A p value of less than 0.05 was regarded as statistically significant.
In theory, some patients in the late-intubation group might have the potential to avoid intubation. Therefore, for sensitivity analyses, patients in whom NIV was successful were classified into the late-intubation group. To balance the baseline data, propensity score matching was employed. Propensity scores were estimated through logistic regression, incorporating covariates including age, sex, SOFA score, presence of septic shock, presence of ARDS, ICU types, diagnosis, underlying disease, vital signs, arterial blood gas test results, and the updated HACOR score. After calculating the propensity scores, patients in the early- and late-intubation groups were matched based on similar propensity scores at a 1:1 ratio. The nearest neighbor method without replacement and a caliper width of 0.05 were utilized for this matching process.
Results
A total of 2179 patients were screened (Figure 1). Among these, 729 patients were at high risk of NIV failure. Among these high-risk patients, 146 patients who refused intubation were excluded. Actual intubation within ⩽12 h was carried out in 171 patients. The time from the initiation of NIV to intubation had a median of 3 h (IQR: 2–7). Actual intubation after >12 h (median 47 h, IQR: 24–101) was performed in 222 patients.

Flow chart of the study.
The demographic data are presented in Table 1. The primary diagnosis was pneumonia. Patients who underwent early intubation had higher respiratory rates (before NIV: 35 ± 10 vs 31 ± 8 bpm; after 1–2 h of NIV: 35 ± 10 vs 30 ± 8 bpm; all p values < 0.001 unless otherwise specified) compared with those who had late intubation (Table 2). In addition, these patients exhibited elevated heart rates and greater HACOR scores following 1–2 h of NIV. However, the mortality rate was lower in the early intubation group (ICU mortality: 36% vs 58%, p < 0.001; and hospital mortality: 38% vs 58%, p < 0.001; Table 3). The crude and adjusted ORs also indicated that the early intubation strategy was a protective factor against the late-intubation strategy (Table 4).
Demographic characteristics.

ARDS, acute respiratory distress syndrome; ICU, intensive care unit; NIV, noninvasive ventilation; SOFA, sequential organ failure assessment.
Variables collected before and after 1–2 h of NIV.
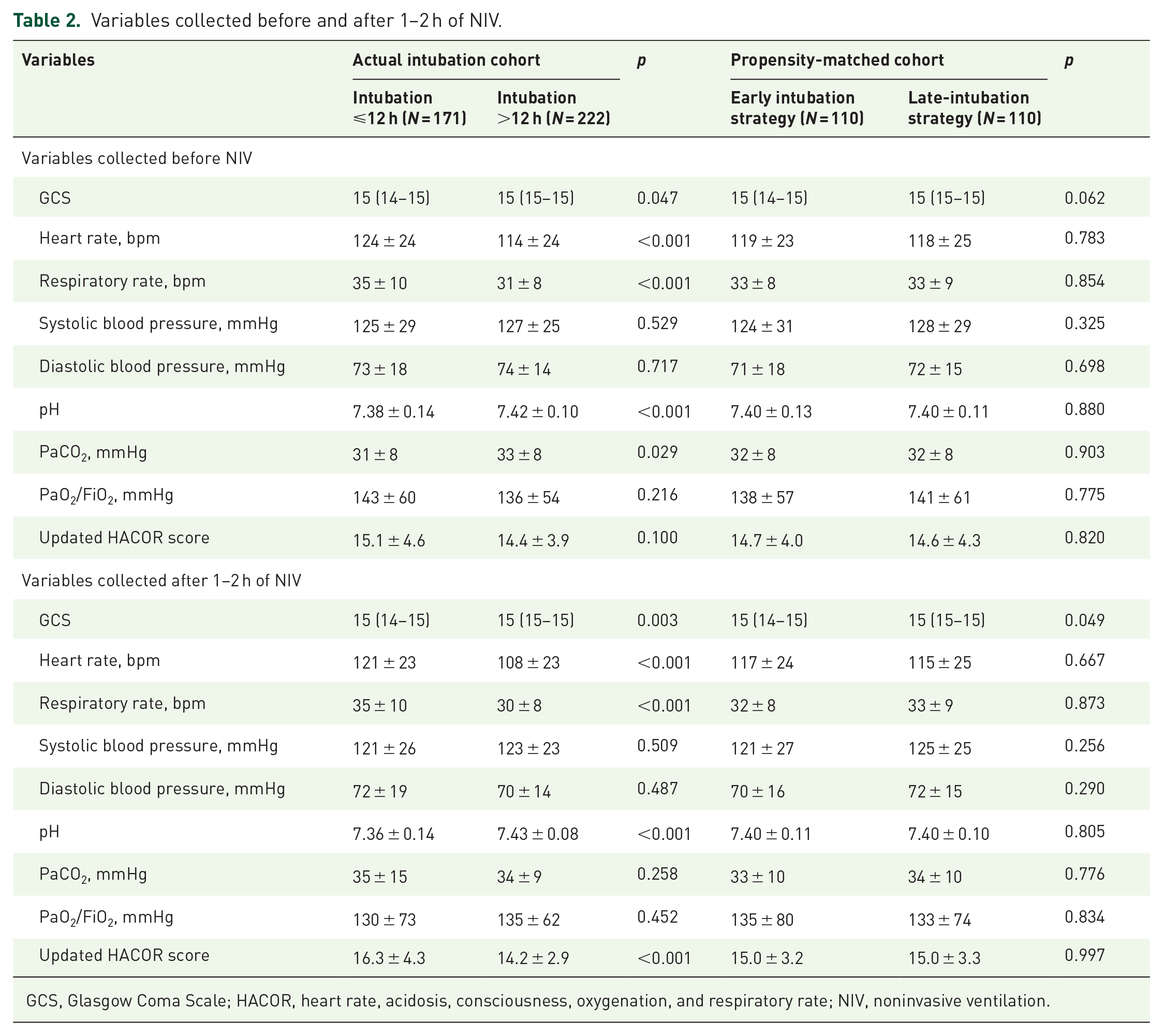
GCS, Glasgow Coma Scale; HACOR, heart rate, acidosis, consciousness, oxygenation, and respiratory rate; NIV, noninvasive ventilation.
Outcomes.

ICU, intensive care unit; NIV, noninvasive ventilation.
Crude and adjusted OR of death in ICU or hospital for early intubation strategy.

It was adjusted by age, sex, SOFA score, presence of septic shock, presence of ARDS, ICU types, diagnosis, underlying disease, vital signs, arterial blood gas tests, and updated HACOR score.
ARDS, acute respiratory distress syndrome; CI, confidence interval; HACOR, heart rate, acidosis, consciousness, oxygenation, and respiratory rate; ICU, intensive care unit; OR, odds ratio; SOFA, sequential organ failure assessment.
Among the patients who were actually intubated, 171 patients underwent intubation within 12 h of NIV initiation, 118 patients between 12 and 48 h, and 104 patients beyond 48 h (Figure 2). The corresponding ICU mortality rates were 36%, 53%, and 63%, respectively. A similar tendency was observed for hospital mortality.
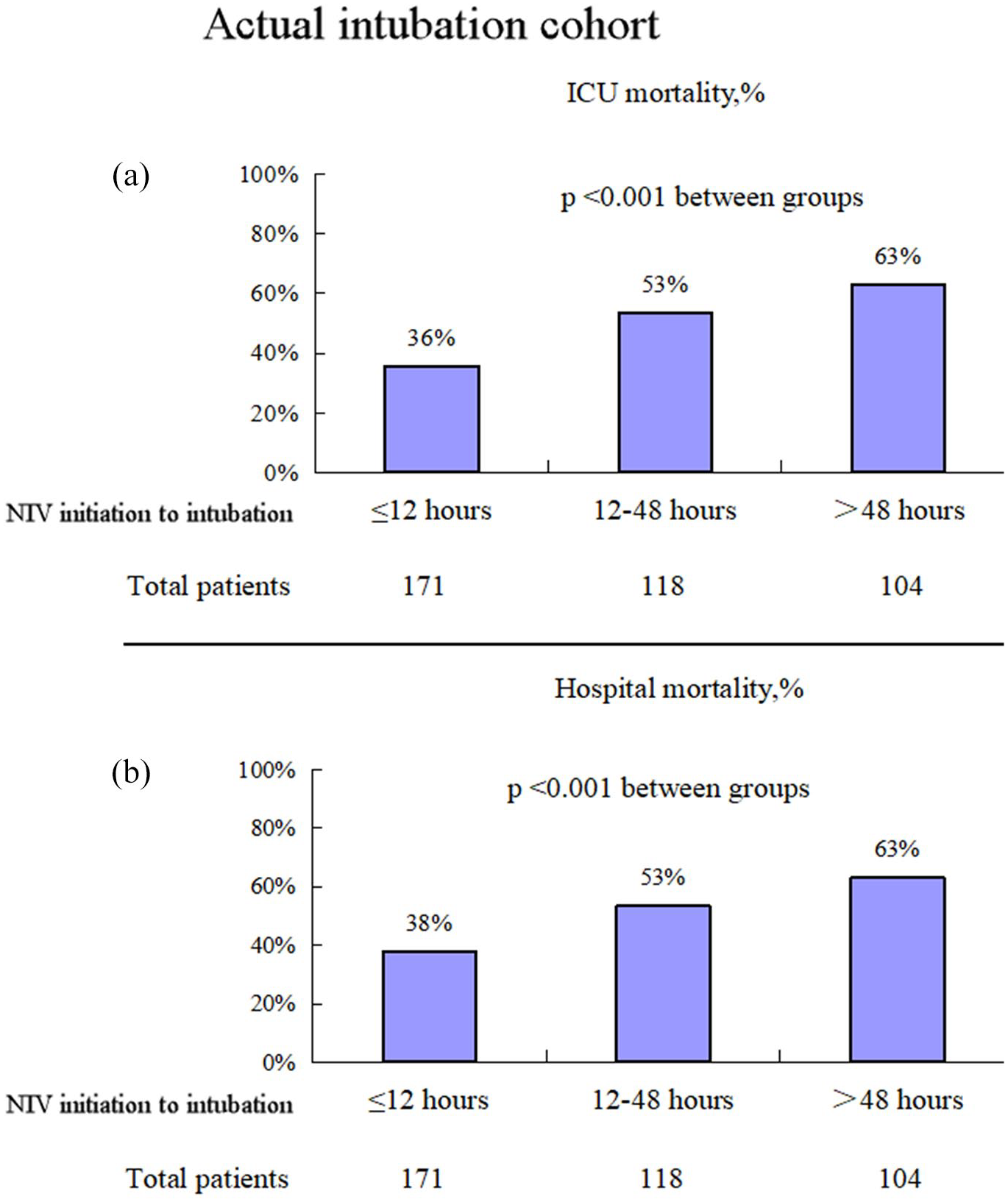
Association between timing of intubation from NIV initiation and mortality.
In sensitivity analyses, 190 patients in whom NIV was successful were categorized into the late-intubation group. Compared to the late-intubation group, early intubated patients exhibited significantly higher SOFA scores, greater prevalence of septic shock, elevated heart rates, increased respiratory rates, and higher updated HACOR scores (Supplemental Table 2). Nevertheless, the ICU and hospital mortality rates did not show significant differences between the groups (36% vs 32%, p = 0.384 and 38% vs 35%, p = 0.447, respectively, Supplemental Table 3). After propensity matching, 110 patients were included in each group. The baseline data were comparable between the groups for most conditions (Supplemental Tables 4 and 5). In the early intubation group, all patients received intubation. In the late-intubation group, however, 78 patients (71%) received intubation. After propensity matching, the early intubation group had lower ICU and hospital mortality rates than the late-intubation group (32% vs 46%, p = 0.052 and 34% vs 50%, p = 0.020, respectively).
Discussion
The current study reveals that mortality increases with an increase in the time intervals from the initiation of NIV to intubation. In patients assigned to the late-intubation strategy, some cases managed to avoid intubation. Nevertheless, the late-intubation strategy may have a higher mortality rate compared to the early intubation strategy.
In a prior study on patients with de novo acute respiratory failure, the NIV failure rate was 46%. 18 Among patients with NIV failure in that particular study, the time from NIV initiation to intubation was 32 ± 24 h in survivors, while it was 78 ± 65 h in nonsurvivors. Other research has also demonstrated that delayed intubation is associated with an elevated mortality rate.19 –21 This suggests that the timing of intubation may be related to mortality in patients with NIV failure. In our study, a dose-response effect was observed. The longer the delay in intubation, the greater the probability of death (mortality rates of 36%, 53%, and 63% were observed among patients intubated within 12 h, between 12–48 h, and more than 48 h, respectively). These findings imply that the evaluation of the efficacy of NIV should potentially be carried out within 12 h of NIV. However, these results need to be validated in further studies before official recommendations can be formulated. Another point worthy of note is that the time elapsed between symptom onset and the initiation of NIV can significantly impact disease progression, as the early use of NIV in patients with mild acute respiratory failure can reduce the progression to a severe condition. 22
Not all cases of late intubation are associated with an increased mortality rate. A study reported that the mortality rate was significantly higher in patients receiving early versus non-early invasive mechanical ventilation. 23 The study included a general population, with an intubation rate of 100% in the early intervention group but only 35% in the non-early intervention group. There might have been a substantial number of patients in the early intervention group who did not need intubation. In our study, however, the intubation rate was 100% in the early intervention group and 71% in the late-intervention group, as we only recruited patients at high risk of NIV failure. Therefore, early intubation is somewhat reasonable in a high-risk patient population.
Spontaneous breathing preservation is essential for NIV. Compared with controlled ventilation, normal spontaneous breathing can enhance gas distribution in the dependent lung regions, improve cardiac function, and mitigate lung injury.24 –26 However, forceful spontaneous breathing can result in strong muscle contractions and large negative pleural pressure swings, which lead to lung injury,27 –29 also known as self-inflicted lung injury. 30 Prolonged exposure to forceful spontaneous breathing is associated with more severe lung injury. Moreover, the development of barotrauma (e.g., pneumomediastinum or pneumothorax) represents the most severe form of lung injury. This may potentially explain the association between delayed intubation and increased mortality in NIV patients. 31 Early detection of barotrauma is crucial for preventing its progression to a severe condition. The Macklin effect, visible on chest computed tomography scans, can be used as a tool to identify the risk of barotrauma at an early stage. 32
Another issue that should be noted is how to define delayed intubation. Merely considering the time from the initiation of NIV to intubation may not be adequate. Instead, the duration during which the patient experiences labored breathing, which could potentially lead to self-inflicted lung injury, might be a more rational criterion. In addition, the updated HACOR score should be regarded as just one of multiple measures for assessing the need for intubation. A reasonable strategy could be to combine this score with esophageal pressure, P0.1, and the tidal volume utilized in NIV.
This study had several limitations. First, as a secondary analysis, it only demonstrates an association between delayed intubation and increased mortality rather than establishing causality. The strength of evidence was limited, and a randomized controlled trial is needed to provide more robust conclusions. Second, the time window used to evaluate the efficacy of NIV was 12 h. Owing to the relatively small sample size, it was not feasible to further narrow this time window. Thus, the optimal time window requires further exploration. Third, we employed the propensity matching method to balance the baseline data between the early- and late-intubation groups. Since this was not a randomized controlled trial, residual confounding from unmeasured variables may persist, potentially influencing the results.
Conclusion
In patients who are at high risk of NIV failure, early intubation is associated with a reduction in mortality. Given that this is a secondary analysis, a randomized controlled trial is warranted to validate this finding.
Supplemental Material
sj-doc-2-tar-10.1177_17534666251347757 – Supplemental material for Association between early intubation and mortality in patients at high risk for noninvasive ventilation failure: a propensity-matched cohort study
Supplemental material, sj-doc-2-tar-10.1177_17534666251347757 for Association between early intubation and mortality in patients at high risk for noninvasive ventilation failure: a propensity-matched cohort study by Tao Huang, Lijuan Chen, Xiaoyi Liu, Ke Wang, Weiwei Shu, Lei Jiang, Linfu Bai, Wenhui Hu, Mengyi Ma and Jun Duan in Therapeutic Advances in Respiratory Disease
Supplemental Material
sj-docx-1-tar-10.1177_17534666251347757 – Supplemental material for Association between early intubation and mortality in patients at high risk for noninvasive ventilation failure: a propensity-matched cohort study
Supplemental material, sj-docx-1-tar-10.1177_17534666251347757 for Association between early intubation and mortality in patients at high risk for noninvasive ventilation failure: a propensity-matched cohort study by Tao Huang, Lijuan Chen, Xiaoyi Liu, Ke Wang, Weiwei Shu, Lei Jiang, Linfu Bai, Wenhui Hu, Mengyi Ma and Jun Duan in Therapeutic Advances in Respiratory Disease
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.