
Abstract
Pulmonary fibrosis (PF) is a progressive and fatal interstitial lung disease characterized by excessive extracellular matrix deposition and fibroblast activation. Current antifibrotic therapies, such as nintedanib and pirfenidone, slow disease progression but fail to halt fibrosis or significantly improve survival. Macrolides, a class of antibiotics with immunomodulatory and anti-inflammatory properties, have emerged as potential adjunctive therapies for PF. Preclinical studies demonstrate that macrolides attenuate fibrogenesis through multifaceted mechanisms: suppression of TGF-β/Smad and JNK/c-Jun signaling, inhibition of pro-fibrotic cytokine release, modulation of macrophage polarization toward antifibrotic M2 phenotypes, and induction of apoptosis in senescent cells. Clinically, macrolides have shown promise in reducing acute exacerbations in idiopathic pulmonary fibrosis (IPF), mitigating radiation pneumonitis, and attenuating post-infectious fibrotic changes. However, conflicting results from clinical trials and the absence of large-scale randomized studies highlight the need for further validation. This review evaluates the antifibrotic mechanisms and therapeutic potential of macrolides in PF, integrating preclinical and clinical evidence. We aim to inform future research directions by elucidating their role in modulating key pathways and addressing unresolved efficacy questions.
Introduction
Pulmonary fibrosis (PF) represents the advanced stage of several diffuse parenchymal lung diseases, 1 particularly interstitial lung disease (ILD), characterized by declining lung function, worsening quality of life, and shortened life expectancy.2,3 Idiopathic pulmonary fibrosis (IPF) is the most prevalent and characteristic form,4,5 with a median life expectancy of only 3–5 years without treatment.6,7 Thirteen to forty percent of patients with non-IPF ILDs also present a progressive fibrosing phenotype. 8 Though current antifibrotic agents such as nintedanib and pirfenidone have shown efficacy in slowing disease progression, they do not cure PF and have only minimally improved mortality rates. Furthermore, immunosuppression has been proven to provide no benefit and could potentially be harmful, particularly in patients with a usual interstitial pneumonia pattern. 9 Overall, the management of PF remains challenging, necessitating ongoing research into effective therapies and strategies to improve patient outcomes.
Though triggers, susceptibility factors, and initial inflammatory responses can differ among fibrosing ILDs,6,8,10 common mechanisms become prominent in the later phases. 11 Persistent micro-injuries to alveolar epithelial cells activate developmental signaling pathways, notably transforming growth factor (TGF)-β. This leads to cellular dysfunction, disrupted equilibrium in the alveolar epithelial-mesenchymal unit, progressive deposition of extracellular matrix (ECM) proteins, epithelial-to-mesenchymal transition (EMT), and subsequent distortion of lung structures 12 (Figure 1.). Recent studies have shown that lung dysbiosis, characterized by increased bacterial load and reduced microbial diversity, has been observed in IPF patients and is associated with disease progression and immune response, 13 potentially contributing to acute exacerbations, hospitalizations, and decreased survival. 14

Regulatory mechanisms and functional characteristics of macrolides in pulmonary fibrosis. Macrolides inhibit EMT, fibroblast proliferation, and apoptosis resistance in both AECs and fibroblasts, ultimately suppressing the deposition of ECM proteins and preventing the formation of scar tissue and distortion of lung homeostasis. Moreover, macrolides promote the transition of activated macrophages from the pro-inflammatory M1 phenotype to the anti-inflammatory M2 phenotype and mobilize other immune cells, including neutrophils and lymphocytes, to participate in the anti-fibrosis process.
Macrolides, a group of antibiotics structured with the macrocyclic lactone ring structure, exert antimicrobial effects by binding to the 50S ribosomal subunit of the
We conducted a comprehensive literature search in PubMed to identify relevant studies on macrolides in PF, including all available records through November 2024, while limiting the search to English-language publications. No lower date restriction was applied to ensure the inclusion of all historical evidence. To ensure comprehensive coverage, we supplemented the electronic search by manually screening reference lists from selected original research articles and review papers. The search strategy incorporated the following key terms: “macrolide” and its main members (“clarithromycin,” “erythromycin,” “roxithromycin,” and “azithromycin”), combined with disease-related terms including “pulmonary fibrosis,” “lung fibrosis,” “idiopathic pulmonary fibrosis,” “IPF,” “interstitial lung disease,” and “ILD.” To capture mechanistic and clinical aspects, we also included terms like “cytokine,” “neutrophil,” “pneumonia,” “pulmonary infection,” “acute lung injury,” “acute respiratory distress syndrome,” and “ARDS.” The screening process followed a three-stage approach: (1) initial review of titles and abstracts for relevance; (2) full-text evaluation when abstracts provided insufficient information; and (3) exclusion of clearly irrelevant studies. Finally, all included studies were systematically categorized into preclinical studies (in vitro/animal models) and clinical studies (human trials).
Macrolides and the non-antimicrobial effects
Macrolides, such as azithromycin (AZM), erythromycin (EM), roxithromycin (RXM), and clarithromycin (CAM), exhibit multifaceted immunomodulatory and anti-inflammatory properties that extend beyond their conventional antibacterial roles. 23 These pleiotropic effects are mediated through diverse molecular mechanisms, including: (1) Suppression of inflammatory signaling pathways,24,25 leading to downregulation of pro-inflammatory cytokines and chemokines while enhancing anti-inflammatory mediators like IL-10; (2) Modulation of innate and adaptive immunity via macrophage polarization,20,26,27 inhibition of neutrophil extracellular trap formation, and regulation of T-cell differentiation; (3) Mucoregulatory actions, including suppression of mucus hypersecretion by blocking EGFR/MAPK-dependent MUC5AC expression and reducing goblet cell hyperplasia28,29; (4) Biofilm disruption30 –32 through interference with bacterial quorum sensing and ECM components, enhancing antibiotic penetration; (5) Antiviral and epithelial repair-promoting effects, potentially via inhibition of viral replication and augmentation of autophagy-mediated epithelial barrier restoration.33 –35
Clinically, these properties have positioned macrolides as disease-modifying agents in chronic respiratory disorders.36,37 Low-dose, long-term macrolide therapy is now a cornerstone in diffuse panbronchiolitis and a guideline-recommended option for frequent exacerbators with COPD or non-cystic fibrosis bronchiectasis,38,39 demonstrating significant reductions in exacerbation frequency and sputum volume. Emerging evidence supports their utility in severe asthma, 40 particularly with neutrophilic phenotypes, post-viral airway hyperreactivity, 41 and cystic fibrosis. 42
Emerging evidence highlights macrolides’ potential to attenuate PF through mechanisms partially overlapping with chronic airway diseases, including TGF-β/Smad signaling suppression, inhibition of pro-fibrotic cytokines, and macrophage M2 polarization. However, it remains unclear whether their efficacy arises from broad immunomodulation or PF-specific pathways—and whether clinical evidence supports their therapeutic use.
Antifibrotic mechanisms of macrolides
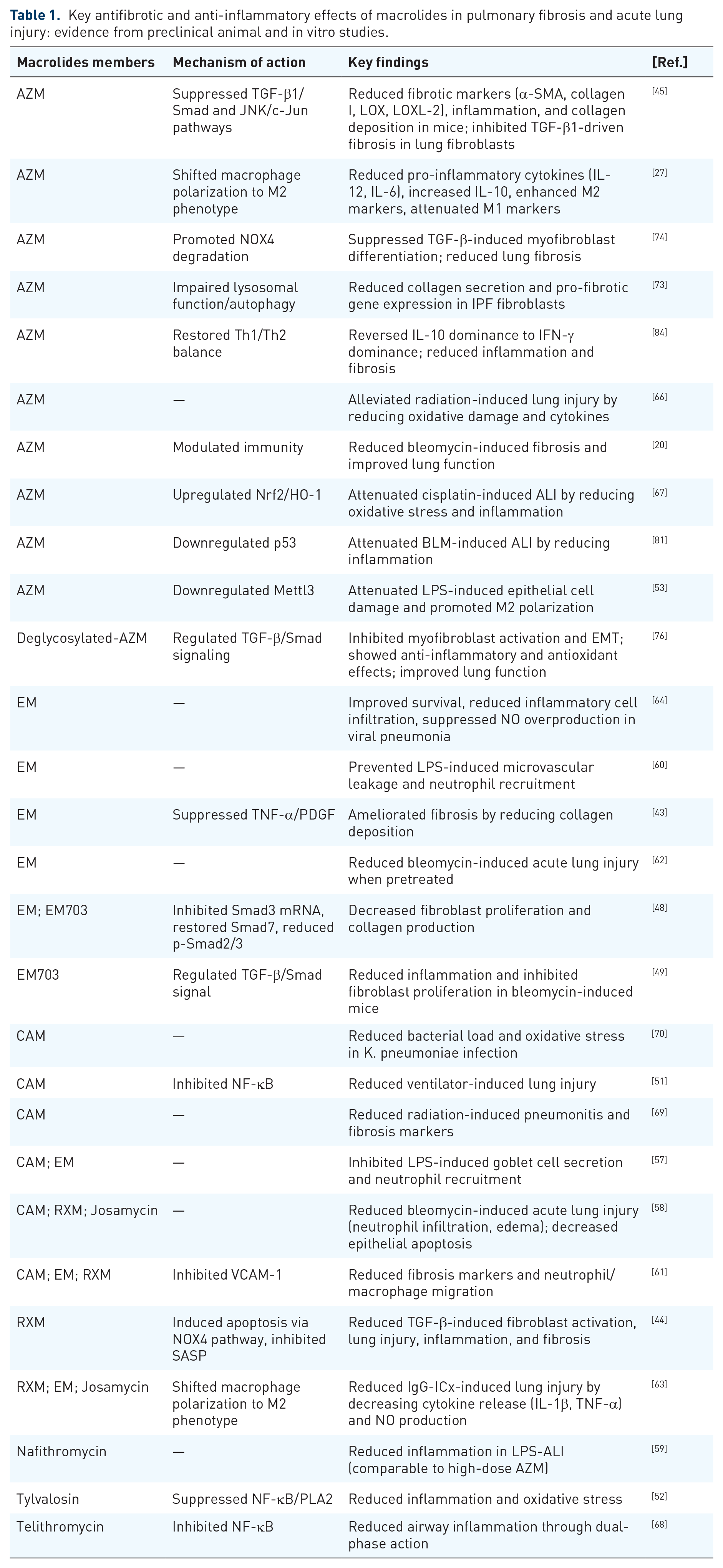
Macrolides have emerged as potential therapeutic agents for PF due to their multifaceted mechanisms of action. Both animal models and in vitro studies suggest a therapeutic role for macrolides in attenuating fibrotic processes.20,43 –45 Below, we categorize their effects based on distinct molecular and cellular pathways (Table 1).
Key antifibrotic and anti-inflammatory effects of macrolides in pulmonary fibrosis and acute lung injury: evidence from preclinical animal and in vitro studies.
Inhibition of TGF-β1/Smad signaling pathway
Macrolides, including AZM, EM, and its derivative EM703, have demonstrated significant potential in inhibiting the TGF-β/Smad signaling pathway, a central driver of fibrosis.46,47 Our team has clarified AZM attenuated bleomycin-induced PF in mice by suppressing TGF-β1/Smad signaling, leading to reduced expression of fibrotic markers such as α-smooth muscle actin (α-SMA), type I collagen, LOX, and LOXL-2, as well as decreased collagen deposition. 45 We also found that AZM inhibited TGF-β1-induced fibrotic responses in primary lung fibroblasts, further supporting its role in blocking TGF-β1-mediated fibrosis. 45 Similarly, EM and EM703 inhibited TGF-β-induced Smad3 mRNA expression, restored Smad7 levels, and reduced p-Smad2/3 protein activation, thereby suppressing fibroblast proliferation and collagen production in human lung fibroblasts, 48 while EM703 also attenuated inflammation and regulated TGF-β/Smad signaling in bleomycin-induced lung fibrosis in mice. 49
Inhibition of NF-κB signaling pathway
The NF-κB signaling pathway plays a vital role in regulating inflammation, immune responses, and fibrosis. 50 Macrolides have been shown to exert antifibrotic effects by modulating NF-κB activation and downstream inflammatory responses. The inhibition of NF-κB signaling by macrolides exerts multifaceted antifibrotic effects by suppressing the expression of pro-inflammatory cytokines 51 (e.g., IL-1β, TNF-α, IL-6, and IL-8), which are key drivers of inflammation and fibrosis, while also attenuating neutrophil recruitment through the downregulation of adhesion molecules 51 (e.g., E-selectin) and chemokines, thereby reducing tissue damage. In addition, NF-κB inhibition downregulates pro-fibrotic mediators such as TGF-β, which are central to fibroblast activation and ECM deposition, and promotes inflammation resolution by enhancing inflammatory cell apoptosis and reducing oxidative stress. 52 Furthermore, macrolides protect epithelial cells from apoptosis and ferroptosis, 53 preserving lung tissue integrity and function, collectively contributing to their therapeutic potential in PF.
Suppression of JNK/c-Jun signaling pathway
JNK1 promotes collagen deposition and pulmonary fibrosis by enhancing TGF-β1 signaling and pro-fibrotic gene expression in response to cellular stress and environmental insults.54,55 AZM has demonstrated inhibitory effects on this pathway. In the same study by our research team, 45 AZM attenuated bleomycin-induced PF in mice by inhibiting the JNK/c-Jun signaling pathway, leading to reduced inflammation and fibrosis.
Anti-inflammatory and antioxidant effects
The severity of acute lung injury (ALI) directly correlates with the extent of subsequent chronic inflammation and fibrosis, 56 suggesting that early intervention using the anti-inflammatory properties of macrolides may be valuable in modulating fibrotic mechanisms. Pretreatment with macrolides significantly decreased neutrophil infiltration,57 –60 inflammatory cell migration, 61 and lung edema 62 in ALI mice models. Macrolides, including EM, RXM, and josamycin, reduced inflammation by decreasing cytokines (IL-1β and TNF-α), iNOS expression, and NO production, as shown in influenza-virus-induced pneumonia and IgG immune complex-induced lung injury models.63,64 Similarly, radiation-induced lung injury (RILI) is a significant complication of thoracic radiotherapy, caused by the direct toxic effects of radiation on lung tissue, followed by an inflammatory cell infiltration that leads to interstitial pneumonia and fibrotic repair processes. 65 AZM attenuated the irradiation-induced increases in the mRNA expression of fibrotic markers in RILI mice by reducing inflammatory cytokine expression (IL-1β, IL-6, TNF-α, TGF-β1) and oxidative damage. 66 AZM attenuated cisplatin-induced ALI in rats by reducing inflammation via upregulation of Nrf2/HO-1 signaling and PPARγ, and also inhibiting necroptosis by enhancing cytoglobin and SIRT1-mediated oxidative stress responses. 67 Deglycosylated azithromycin (Deg-AZM) and telithromycin both exhibited anti-inflammatory by suppressing NF-κB activation, phospholipase A2 activity, decreasing inflammatory mediators, and enhancing inflammatory cell apoptosis. 68 These findings collectively highlight the shared anti-inflammatory mechanisms of macrolides across different models of lung injury.69,70
Modulation of autophagy and lysosomal function
Autophagy dysregulation is implicated in fibrosis.71,72 AZM has been shown to impair lysosomal function and autophagy in IPF fibroblasts, which not only reduces collagen secretion and pro-fibrotic gene expression 73 but also promotes NOX4 degradation through enhanced proteasome activity and autophagy inhibition, ultimately suppressing myofibroblast differentiation. 74
Inhibition of myofibroblast activation and EMT
EMT, a process where alveolar epithelial cells lose epithelial traits and acquire mesenchymal properties, 75 significantly contributes to fibrosis by expanding the myofibroblast pool. AZM has been shown to inhibit EMT and myofibroblast activation, key drivers of fibrosis. Specifically, AZM promotes NOX4 degradation, 74 suppressing TGF-β-induced myofibroblast differentiation and reducing lung fibrosis. In addition, Deg-AZM attenuates bleomycin-induced PF by further inhibiting EMT and myofibroblast activation. 76 These findings highlight AZM’s dual role in targeting both NOX4/TGF-β signaling and EMT, offering a multifaceted approach to mitigating fibrosis.
Induction of apoptosis in senescent cells
Cellular senescence, particularly in fibroblasts and epithelial cells, contributes to chronic inflammation and fibrosis.77,78 Senescent cells accumulate in fibrotic tissues and release pro-inflammatory cytokines, growth factors, and ECM components, collectively known as the senescence-associated secretory phenotype (SASP). 79 AZM and RXM were identified as novel senolytic drugs that preferentially target senescent human fibroblasts, inducing autophagy and metabolic changes, 80 EM did not demonstrate comparable senolytic effects. In addition, RXM targeted senescent cells by inducing apoptosis and inhibiting SASP factors through the NOX4 pathway, which reduced TGF-β-induced fibroblast activation, and diminished lung injury, inflammation, and fibrosis in bleomycin-induced mice. 44 AZM nanostructured lipid carrier (AZ-NLC) was shown to enhance senescent cell clearance in bleomycin-induced lung injury models through p53 downregulation and Bcl-2 expression modulation, further supporting the senotherapeutic potential of macrolides in PF. 81
Restoration of immune cell balance
Macrolides play a crucial role in regulating immune cell balance by targeting multiple immune cells.70,82,83 AZM promotes macrophage polarization toward the anti-inflammatory M2 phenotype by downregulating Mettl3 and inactivating the NF-κB pathway, leading to reduced pro-inflammatory cytokines (IL-12, IL-6) and increased anti-inflammatory IL-10, enhanced M2 markers (mannose receptor, CD23, arginase activity). 27 This polarization supports the tissue repair process and may help prevent pathological fibrosis. AZM can also reverse the Th2-like response (IL-10 dominance) to a Th1-like response (IFN-γ dominance) in bleomycin-induced PF in rats, 84 reducing inflammatory cell infiltration and fibrosis at the early stage of fibrosing alveolitis.
Inhibition of mucus production
Macrolides have been shown to exert beneficial effects in chronic airway diseases through their ability to reduce mucus viscosity and enhance mucociliary clearance,85,86 contributing to improved pulmonary function and decreased infection risk in affected patients. Experimental studies using guinea pig tracheal models have demonstrated that CAM and EM can effectively suppress LPS-induced goblet cell secretion and attenuate neutrophil recruitment, 57 suggesting the potential anti-inflammatory effect. While these findings are promising, further targeted trials are needed to assess their additional effects in patients with PF. In recent years, rapid advancements have been made in developing drug delivery systems for PF. 87 For instance, inhalable nanoparticles loaded with antifibrotic drugs enable rapid and site-specific delivery to the pulmonary airways, offering potential early relief for patients. 88 However, the airway mucus layer poses a natural barrier to inhaled drug delivery. In this context, macrolides may play an adjunctive role in antifibrotic therapy by indirectly suppressing mucus production.
Modulation of lung microbiota
In chronic pulmonary diseases such as PF, reduced microbial diversity and increased bacterial load are closely linked to disrupted pulmonary homeostasis, which is associated with poor clinical outcomes and disease progression.13,89,90 Biofilms, structured bacterial clusters encased in a self-produced matrix 91 , can persist in the lungs, promote chronic inflammation, and complicate infections, thereby contributing to disease progression. 92 Notably, chronic airway inflammation in PF patients is often accompanied by increased harboring of potentially pathogenic pathogens, such as Haemophilus, Neisseria, and Streptococcus species than healthy controls. 93 Patients with AE-IPF showed significant respiratory microbiome alterations as well, including increased Campylobacter and Stenotrophomonas species compared to stable controls. 94 This dysbiosis may further contribute to airway damage and fibrosis progression through biofilm-mediated persistent stimulation.93,95,96 Macrolides exert multifaceted effects on bacterial biofilms by disrupting quorum sensing,32,97 suppressing virulence factors,98,99 and degrading established biofilm matrices. 31 They simultaneously inhibit bacterial-epithelial adhesion 30 while enhancing mucosal clearance and epithelial repair. These combined mechanisms ameliorate biofilm-mediated inflammation and bacterial persistence, potentially mitigating disease progression in chronic respiratory conditions. Based on current evidence, macrolides may represent a potential adjunctive therapy combined with antifibrotic medications to provide new therapeutic possibilities. However, this hypothesis requires further validation through additional preclinical studies.
Potential prokinetic effects of macrolides
Evidence suggests that gastroesophageal reflux disease (GERD) and esophageal dysmotility may contribute to the development and progression of PF.100,101 As potent motilin receptor agonists, macrolides enhance gastrointestinal motility, accelerate gastric emptying, and reduce GERD frequency. 102 This prokinetic effect may synergize with their direct anti-inflammatory properties, potentially alleviating reflux-mediated lung injury and improving PF-related symptoms such as chronic cough. 103 However, the clinical efficacy of targeting GERD in PF remains contentious. A pooled analysis of randomized controlled trials demonstrated that proton pump inhibitors slowed forced vital capacity decline in IPF patients, although they failed to improve survival or reduce hospitalization rates 104 and may even increase the risk of severe respiratory infections in advanced IPF. 105 Further prospective studies are warranted to delineate the relative contributions of macrolides’ dual mechanisms—prokinetic effects and direct antifibrotic actions—in modulating PF progression.
Clinical evidence on macrolides in PF
Macrolides exert antifibrotic effects through multiple mechanisms, including inhibition of TGF-β1/Smad and JNK/c-Jun signaling, anti-inflammatory and antioxidant effects, modulation of autophagy and lysosomal function, induction of apoptosis in senescent cells, and restoration of immune balance, making macrolides a potential candidate for the adjuvant treatment of PF. However, further clinical studies are needed to validate these findings and translate them into therapeutic applications. This section summarizes key clinical studies, highlighting their findings and implications for PF management (Table 2).
Macrolides in pulmonary fibrosis: Clinical evidence summary.

RP, radiation pneumonitis.
Effects on acute exacerbations in PF
Long-term macrolide therapy has been associated with a reduction in acute exacerbations (AEs) in PF. A retrospective cohort study found that patients receiving EM or CAM experienced significantly fewer AEs and improved 36-month survival rates. 106 These benefits are likely attributed to the anti-inflammatory properties of macrolides in long-term use, which may suppress the inflammatory cascade driving disease progression.
Two studies investigated the short-term use of AZM during acute exacerbations of IPF and chronic fibrosing interstitial pneumonia (AE-CFIP).107,108 In IPF patients, short-term AZM combined with corticosteroids significantly reduced 60-day mortality. 108 Similarly, in AE-CFIP patients, AZM reduced 60-day mortality and improved median survival time. 107 A retrospective study of IPF patients with rapidly progressing respiratory failure found that macrolide use was associated with improved survival, 109 suggesting a potential benefit in AEs when combined with high-dose corticosteroids. However, current guidelines emphasize that corticosteroids lack definitive benefit in IPF exacerbations and may even contribute to adverse outcomes. 110 Notably, while macrolides possess immunomodulatory effects, their acute therapeutic effects in these studies are likely mediated primarily through antibacterial or antiviral activity against pathogens, rather than immune modulation.35,111 The potential role of immunomodulation in AEs remains unverified and requires further high-quality evidence. 112
Potential improvement in prognosis and symptoms in PF
In addition to reducing AEs, long-term prophylactic macrolide therapy has been associated with improved survival in IPF patients. 106 Another retrospective observational study demonstrated that prophylactic AZM significantly reduced all-cause non-elective hospitalizations in IPF patients and decreased rescue antibiotic use. 22 These benefits were achieved without impacting the rate of decline in lung function, suggesting that macrolides may exert their effects through mechanisms beyond direct antifibrotic activity, such as reducing infection-related complications that contribute to disease progression. However, a randomized controlled trial 113 found that low-dose AZM did not improve cough-related quality of life, cough severity, or objective cough frequency in IPF patients, with more frequent gastrointestinal side effects, suggesting that efficacy may vary depending on dosing regimens and patient populations.
Long-term macrolide therapy has shown benefits in chronic pulmonary diseases beyond IPF. A non-controlled open-label trial found that long-term AZM therapy significantly reduced cough frequency by about 49.6% and improved quality of life in pulmonary sarcoidosis patients. 103 However, the noncontrolled design and small sample size limit causal inference, highlighting the need for robust trials to confirm the findings.
Several case reports114 –116 described improvements in symptoms and radiological findings in patients with specific subtypes of interstitial pneumonia, such as airway-centered interstitial fibrosis 116 and desquamative interstitial pneumonia. 114 These cases suggest that macrolides may slow disease progression in certain PF subtypes, such as ILD patients with human leukocyte antigen (HLA)-B54 positivity. 115
Prophylactic use in RP
Macrolides have been explored for their prophylactic role in reducing radiation pneumonitis (RP), a common complication of thoracic radiotherapy. 65 Two retrospective cohort studies reported that prophylactic administration of CAM significantly reduced the incidence of Grade ⩾2 RP and Grade ⩾3 RP.117,118 These effects are likely mediated by the suppression of radiation-induced inflammation, highlighting the potential of macrolides in mitigating treatment-related complications. However, the optimal CAM regimen of dose/duration and protective durability against RP remains unclear.
Role in post-infectious PF
Macrolides have also been investigated for their potential role in mitigating fibrotic changes following severe respiratory infections. A case series reported that AZM combined with pirfenidone and prednisolone improved symptoms, effort tolerance, and radiological findings in three patients with PF following H1N1 ARDS, 119 suggesting its adjunctive value to antifibrotic therapy potentially through the anti-inflammatory and immunomodulatory effects.
Prospects of macrolides in PF treatment
While preclinical and early clinical studies highlight the promising therapeutic potential of macrolides in PF, further research is essential to establish them as a standard treatment option. Key areas for future investigation include large-scale randomized controlled trials, optimization of dosing and duration, timing of administration, and deeper mechanistic insights into their antifibrotic and anti-inflammatory effects. In addition, long-term safety and efficacy evaluations, as well as real-world studies, are crucial to confirm their clinical benefits and pave the way for personalized and effective treatment strategies in PF.
Protective effects on alveolar epithelial cells during early injury: Understanding whether macrolides can prevent excessive damage to AECs early in the injury process could offer a preventive strategy for PF progression.
Fibroblast, endothelial cell, and EMT mechanisms: Further research into how macrolides affect these key cells and processes will deepen our understanding of their antifibrotic potential.
Combination therapies: Exploring combinations of macrolides with other antifibrotic agents, as well as the molecular mechanisms behind their synergy, could lead to more effective treatment protocols, while also fully considering potential adverse effects and drug-drug interactions to ensure safety and efficacy in individualized treatment plans.
Macrolide modifications: Engineering macrolides to enhance their antifibrotic effects, such as increasing their anti-inflammatory or immunosuppressive properties, is a potential direction for future research.
Personalized Medicine: Identifying which patients with PF are most likely to benefit from macrolide therapy based on their EMT profiles and TGF-β activity could optimize treatment strategies. Personalized medicine approaches may include genetic testing or biomarkers to predict responses to macrolides.
Rigorous clinical trials: Randomized controlled trials and real-world studies will be necessary to determine the long-term benefits of macrolides in PF and solidify their place in clinical practice.
Conclusion
Macrolides show considerable potential in treating PF, owing to their anti-inflammatory and antimicrobial properties, as well as the ability to modulate key cellular processes such as fibroblast activation, EMT, and cellular senescence. Their combination with other antifibrotic therapies may offer a multifaceted approach to treating this complex and progressive disease. Ongoing research is needed to confirm their efficacy in clinical settings and to explore potential improvements through combination therapies and drug modifications.