
Abstract
Background:
During the COVID-19 pandemic, telemedicine became crucial for monitoring chronic conditions, including respiratory diseases.
Objectives:
This study, part of a larger cohort of COVID-positive patients, focuses on individuals with chronic obstructive pulmonary disease (COPD) monitored through an active home surveillance system (COD19).
Design:
Longitudinal telematic active surveillance study.
Methods:
The study included COVID-19-positive patients in home isolation, quarantined workers, and those discharged from ASST hospitals or emergency departments. At discharge, patients received a letter with isolation guidelines, a COD19 kit (oxygen meter, thermometer, protective devices), and instructions for monitoring clinical parameters. Regular phone check-ins by physicians were conducted, starting within 12 h of activation. A secure platform COD19 enabled data collection and communication between patients, healthcare providers, and regional authorities.
Results:
The study involved 1288 patients, including 226 (17.5%) with COPD, who were older (p < 0.001), had a higher BMI (p = 0.006), and were more frequently admitted from home isolation (p < 0.001). COPD patients also had higher mean body temperature (p = 0.011) and respiratory rate (p = 0.035), with a non-significant trend toward lower SpO2 values. Monitoring outcomes indicated that COPD patients were more likely to require higher levels of care (p < 0.001), and the only two deceased patients were from this group. The remote monitoring service received positive feedback, with a median answering ratio of 92%, reflecting strong patient participation and manageable monitoring processes.
Conclusion:
The findings underscore telemedicine’s effectiveness in COPD management, ensuring continuity of care and smooth home-to-hospital transitions. The system enhanced accessibility, enabling consistent monitoring and timely interventions. As healthcare evolves, telemedicine remains a key tool in improving patient care and accessibility.
Keywords
Introduction
Chronic obstructive pulmonary disease (COPD) is a leading global health concern, contributing significantly to morbidity, mortality, and healthcare utilization.1 –4 It is characterized by persistent and only partially reversible airway obstruction, diagnosed through spirometry.5,6 COPD encompasses both chronic bronchitis, primarily affecting larger airways, and emphysema, characterized by destruction of lung parenchyma, leading to air trapping and exertional breathlessness. While cigarette smoking remains the primary risk factor, exposure to indoor air pollutants—especially in developing regions—can also play a role in its onset and progression.5 –8
COPD patients exhibit increased vulnerability to respiratory viral infections and virus-induced exacerbations triggered by influenza, rhinoviruses, and seasonal coronaviruses.9,11 Studies indicate that respiratory viruses are responsible for approximately 50% of COPD exacerbations,9,10 raising the possibility that SARS-CoV-2 could also contribute to exacerbations in these patients. 10 The objectives in managing COPD include slowing disease progression and alleviating its symptoms.6,7 Monitoring patients’ physical and mental well-being is essential for optimal management, as regular follow-ups provide valuable information that supports the attainment of these treatment objectives. 8
During the COVID-19 pandemic, telemedicine gained significant importance, particularly for evaluating and monitoring patients with chronic conditions, including respiratory disease, thereby reducing the need for in-person visits to healthcare facilities.12 –18
Telemedicine refers to the use of electronic information and communication technologies by healthcare professionals to deliver and support medical care for patients at a distance.13 –15 It includes various tools such as videoconferencing, wearable devices, internet platforms, mobile applications, store-and-forward systems, streaming media, and both terrestrial and wireless communication. Consistent with guidance during the pandemic, telemedicine approaches, including virtual appointments, were often employed to substitute or delay in-person consultations for patients with COPD.15,16 Telemonitoring, through telemedicine programs, allows the delivery of quality healthcare to patients who have limited access to health services.12 –18 Additionally, telehealth facilitates self-management by providing patients with access to relevant information while enabling the transfer of monitored health data.
During the pandemic, our group developed a telemedicine service 19 to manage home-care patients (virtual hospital) and provide real-time analysis to help predict healthcare system strain and optimize resource allocation using predictive and prescriptive models. An active Home Surveillance System (Operations Center for Discharged Patients; COD19) and the Home Hospital Care System (COD20) were established on a computer platform specifically designed for the pandemic. This initiative was made possible through a collaboration between the University of Milan, the Health Protection Agency (Agenzia per la Tutela della Salute—ATS) of the Metropolitan City of Milan, the Local Health and Welfare Agency (Azienda Socio-Sanitaria Territoriale-ASST) Fatebenefratelli-Sacco hospitals, and industrial research partners.
This study builds on a larger cohort investigation of COVID-positive patients, which includes a subgroup of individuals with COPD, who have been monitored using the COD19 telemedicine platform. The aim of this report is to share our experiences and emphasize the effectiveness and potential benefits of telemedicine platforms in managing COPD during epidemic situations and other circumstances that necessitate isolation.
Materials and methods
Study design and patient selection
The Operations Center for Discharged Patients (COD19) was an active surveillance service for home-care patients that involved: (1) monitoring critical clinical conditions; (2) recognizing social and health issues; and (3) providing necessary clinical services in the form of a telemedicine service. COD19 was based on a call center that was active 16 h a day, 7 days a week.19,20
Inclusion criteria were: subjects aged > 18 years, both male and female; COVID-19-positive patients during their home isolation reported by the municipality health department, healthcare; COVID-19-positive workers or suspected positive ordered to home quarantine by the Occupational Medicine specialist; COVID-19-positive patients discharged from the Emergency Departments of the ASST hospitals or discharged from the inpatient hospital wards of the ASST hospitals.
Exclusion criteria were: patients under 18 years of age; patients unable to provide informed consent; patients without access to a telephone or digital device necessary for remote monitoring.
At discharge, each patient was given a letter recommending home isolation, instructions for fiduciary home isolation, a COD19 kit containing an oxygen saturation meter, a thermometer, and individual protection devices, a letter communicating the start of the COD19 service, and instructions for taking the clinical parameters.
Surveillance involved phone calls from resident physicians to monitor various clinical parameters related to COVID-19 infection throughout the quarantine period. The initial contact with the patient occurred within 12 h of the request for home surveillance activation. This active home surveillance utilized a secure platform for data collection, processing, and communication with patients, healthcare providers, the ATS, and the region.
For statistical purposes, the patients were divided according to the presence of a previously documented diagnosis of COPD into patients with or without COPD.
The study was conducted in accordance with the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines for observational studies (Supplemental File 1). 21
Data collection
For each patient using the service, the following clinical data were collected: body temperature; percent oxygen saturation at rest; percent oxygen saturation after a 6-minute walk test; and number of breaths per minute. Patients were equipped with pulse oximeters and thermometers and provided with written instructions for their use. Patients discharged from hospital settings often received brief verbal reinforcement on device usage. During the regular monitoring calls, operators could address patient queries and potentially identify grossly inconsistent readings. Nevertheless, ensuring data accuracy in unsupervised remote monitoring presents inherent challenges, including potential variability due to factors like peripheral perfusion affecting pulse oximetry.
The parameters collected were analyzed using an algorithm. If any parameters were abnormal, the operator reached out to the designated infectious disease specialist for further instructions on monitoring or contacted the patient directly. During the call, the operator also gathered clinical information regarding the patient’s COVID-19 history and any underlying comorbidities. The patient’s general practitioner was informed via email within 12 h that the patient was being monitored by the Active Home Surveillance Service.
Clinical decision-making within the COD19 system was primarily guided by pre-defined alert thresholds prompting operator action or specialist consultation. These thresholds included: body temperature ⩾37.5°C, respiratory rate >22 breaths per minute, oxygen saturation (SpO2) < 95%, or a reduction in SpO2 of more than five points following the walk test. For the 6-minute walk test, patients received written instructions guiding them to walk continuously for 6 min within their home, typically in the longest available clear path, at a self-selected pace suitable for their condition and environment. They were instructed to record SpO2 immediately before starting and immediately after completing the walk.
If a patient’s clinical parameters remain negative for 4 consecutive days, active home surveillance is reduced to one phone call per day. The resolution of symptoms does not equate to microbiological clearance, and the patient may still be contagious. Therefore, they must observe a period of self-quarantine at home, remaining isolated and avoiding contact with others for at least 14 days after symptoms have resolved. During home surveillance, if body temperature is recorded at 37.5°C or higher, respiratory rate exceeds 22 breaths per minute, oxygen saturation (SpO2) falls below 95%, or there is a reduction in oxygen saturation of more than five points during a walk test, the counting of days for clinical recovery is reset, starting from the first day when all parameters are negative. After the 14-day isolation period, the patient must undergo two follow-up swab tests, spaced 48 h apart. If both tests are negative, it indicates complete resolution of the infection, the virus is no longer present, and the quarantine can be concluded. If either or both tests are positive, they must be repeated after 1 week, and home isolation will continue.
Statistical analysis
Continuous variables were reported as median and interquartile range (IQR; 25th, 75th percentile), whereas categorical variables were reported as count (fraction). For unadjusted comparison between groups, we used the Wilcoxon rank sum test and the Pearson’s Chi-squared test where appropriate.
Patients were categorized into two groups:
Patients with COPD (COPD)
Patients without COPD (No-COPD)
Analysis of covariance (ANCOVA) was used to compare parameters during monitoring between the two groups, adjusting for age, sex, body mass index (BMI, calculated as weight divided by height squared), and smoking habits. The parameters compared included:
Body temperature (°C)
Percent oxygen saturation at rest (%)
Percent oxygen saturation after a 6-minute walk test (%)
Number of breaths per minute
For the longitudinal analyses comparing mean physiological parameters over the monitoring period (presented in Table 2 and Figure 1), each patient’s average value for body temperature, SpO2 at rest, SpO2 post-walk, and respiratory rate was calculated. To ensure a minimum level of data density for these mean calculations, patients who had, on average, <1 recorded measurement per week for these parameters during their time in the COD19 service were excluded from these specific analyses.

Trends in body temperature, SpO2, SpO2 after a 6-minute walk test, and respiratory rate over the first 21 monitoring days (median monitoring duration) for patients with and without COPD.
Statistical analyses were performed in R 4.0.4. 22
Results
A total of 1288 patients were included in the study, of whom 226 (17.5%) had COPD. Patient characteristics are shown in Table 1. The median age of the patients was 52 years (IQR 38, 64), and 695 (55%) were female. The median BMI was 24.7 kg/m2 (IQR 22.0, 27.7). The majority of patients were never smokers (67%), and 34% were admitted from home isolation.
Characteristics of patients with (COPD) and without COPD (No-COPD).
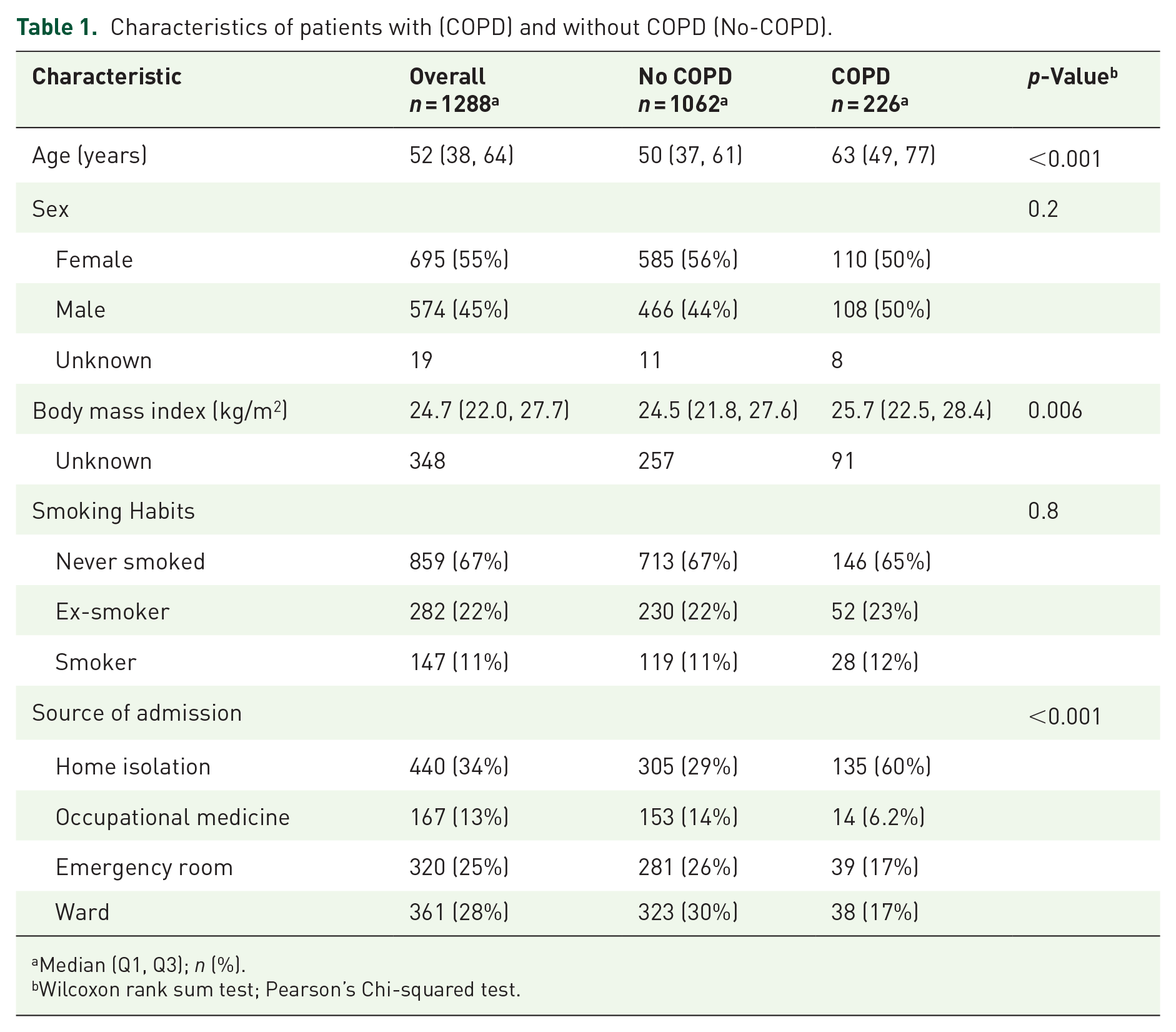
Median (Q1, Q3); n (%).
Wilcoxon rank sum test; Pearson’s Chi-squared test.
COPD patients were older (median age 63 vs 50 years, p < 0.001), had a higher BMI (median 25.7 vs 24.5 kg/m2, p = 0.006), and were more likely to be admitted from home isolation (60% vs 29%, p < 0.001) than No-COPD patients. There were no significant differences between the two groups in terms of sex or smoking habits.
The median monitoring duration was 2.93 weeks (IQR 2.14, 4.29) for No-COPD and 2.71 weeks (IQR 2.00, 3.86) for COPD patients. There was no significant difference in monitoring duration between the two groups (adjusted difference −0.02 weeks, 95% CI −0.73 to 0.69, p > 0.9).
Table 2 shows the comparison of monitoring duration and physiological parameters between COPD and No-COPD patients, adjusted for age, sex, and BMI. Patients with COPD had significantly higher mean body temperature (36.12°C vs 36.07°C, p = 0.011) and respiratory rate (18.4 vs 17.8 breaths per minute, p = 0.035) during monitoring, compared to those without COPD. While there were no statistically significant differences between the groups in terms of mean SpO2, both at rest and after the 6-minute walk test, a trend toward lower SpO2 values in COPD patients is apparent in Figure 1. Analysis was performed on the subgroup of patients requiring supplemental oxygen therapy during the monitoring period (N = 15 with COPD, N = 94 without COPD). No statistically significant difference in mean SpO2 was observed between the COPD and No-COPD patients receiving oxygen (Median [IQR]: 96% [95, 97] vs 97% [95, 98]; adjusted difference 5.8, 95% CI −23 to 34, p = 0.7). Moreover, within both the COPD and No-COPD groups, recorded SpO2 values did not significantly differ between measurements taken with versus without supplemental oxygen (p = 0.4 for COPD, p = 0.9 for No-COPD).
Comparison of monitoring duration and physiological parameters between patients with and without COPD.

Adjusted for age, sex, and body mass index.
Median (Q1, Q3).
ANCOVA.
CI, confidence interval.
Figure 1 displays the trends in body temperature, SpO2 (at rest and after the 6-minute walk test), and respiratory rate over the monitoring days for COPD and No-COPD patients. Notably, while not statistically significant, No-COPD patients consistently exhibit higher SpO2 values throughout the monitoring period compared to those with COPD.
Table 3 presents the monitoring outcomes for COPD and No-COPD patients. It shows that patients with COPD were more likely to be transferred to higher levels of care (4.4% vs 1.2%, p < 0.001). The only two deceased patients were part of the COPD group.
Monitoring outcomes for patients with and without COPD.
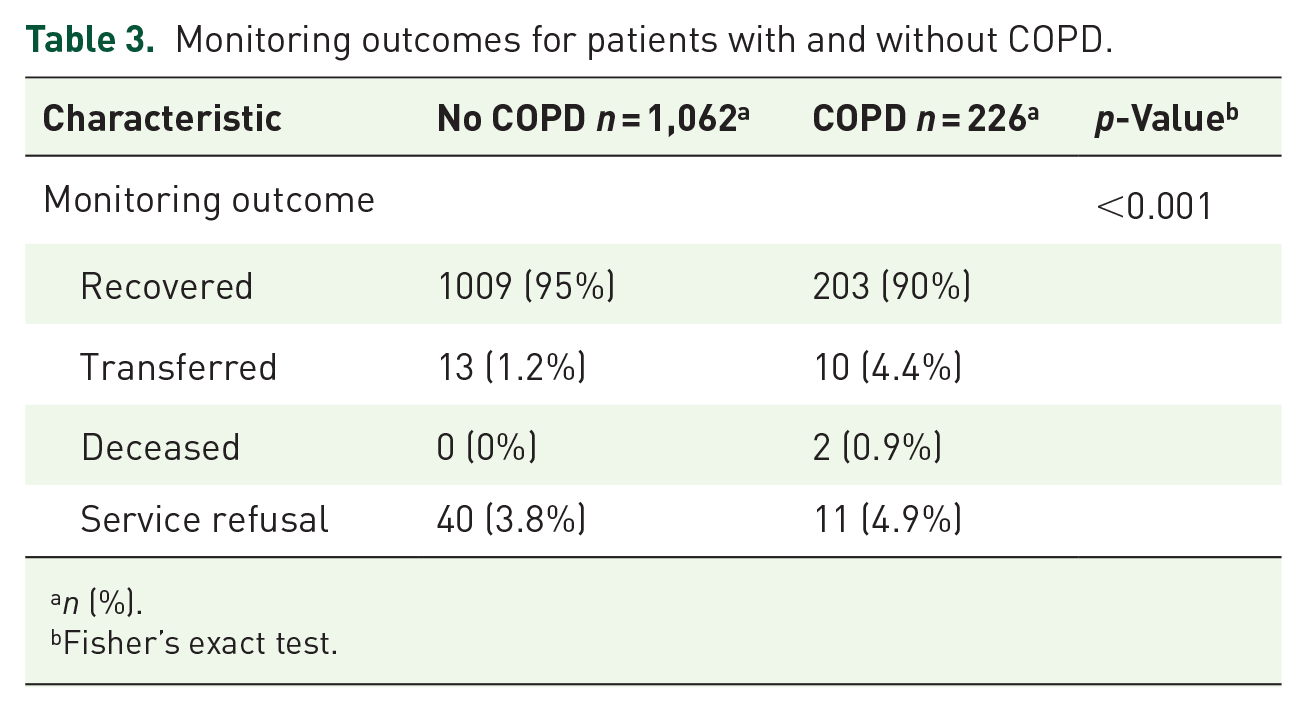
n (%).
Fisher’s exact test.
Overall, the remote monitoring service was well-accepted by patients. The median answering ratio, which represents the percentage of calls answered by patients, was 92% (IQR 83%, 97%) overall, with no significant difference between COPD and No-COPD patients (90% vs 92%, p = 0.9). This high response rate suggests that patients were generally willing to participate in the program and found the monitoring process to be manageable.
Discussion
Our experience demonstrates that telemedicine services can provide valuable monitoring for COPD patients by recording all vital parameters and functional tests. We were able to track trends in body temperature, SpO2 levels, and respiratory rate over the monitoring period, including measurements taken after a 6-minute walk test; in cases of more critical conditions, the telemedicine platform enabled the rapid transfer of patients to the hospital. The telemedicine approach was well-received and easy to manage, providing a promising tool for COPD management, especially in situations requiring isolation.
The relatively high proportion of non-smokers within the documented COPD cohort might be partially explained by the referral mechanisms during the pandemic. Referrals from home isolation or stable patients discharged from hospitals to the COD19 service may have inadvertently selected for individuals with less severe baseline respiratory conditions, potentially including COPD less strongly associated with extensive smoking histories. It is also important to remember that while smoking is primary, other factors like environmental exposures contribute to COPD development.5 –8 While the analysis revealed statistically significant differences in mean body temperature and respiratory rate between the groups, the absolute differences were small. The practical clinical relevance within the COD19 service stemmed not from these minor average differences, but from the system’s response protocol triggered when individual patient readings exceeded the pre-defined alert thresholds, leading to further assessment or intervention.
Our findings are consistent with the broader literature on telemedicine for COPD, which has shown that telemedicine interventions are generally well-received by patients. The use of telemedicine and its efficacy in the management of COPD patients has been evaluated over the past decade (2013–2022) through the existing literature by Vila et al. 16 Different approaches are available: home telemonitoring, tele-education and self-management, telerehabilitation and mobile health (mHealth).17,18 The overall findings indicate positive effects in health status improvement, reduction in healthcare resource utilization, feasibility of implementation and patient satisfaction, while no safety issues were identified in the studies reviewed. The authors conclude that telemedicine is a promising complement to traditional healthcare methods in managing COPD, enhancing health outcomes, and optimizing resource use. 16
Madawala et al. 23 reviewed existing literature to understand how the COVID-19 pandemic affected healthcare experiences for adults with COPD, analyzing qualitative, quantitative, and mixed studies published between December 2019 and June 2022. Prior to COVID-19, studies of COPD patients highlighted the importance of the doctor-patient relationship for the quality of care, which may influence health outcomes. The study reveals that the pandemic disrupted healthcare access, leading to increased anxiety, isolation, and a fear of virus exposure among COPD patients. Innovations such as telemedicine and online rehabilitation programs were positively received, helping mitigate some challenges by maintaining patient care, physical activity, and social connection, such as exercise through Zoom classes. However, many COPD patients expressed concerns about being forgotten by healthcare providers during the pandemic. Overall, the review emphasizes the need for continued telehealth options and standardized protocols to support COPD patients effectively, highlighting the importance of addressing both the physical and emotional needs of this vulnerable group.23,24
Saheli et al. 25 highlighted the importance of remote monitoring of patients with COVID-19 to alleviate hospital capacity pressures, ensuring that resources were available for the most critically ill patients, such as COPD patients. As in our patients, the oxygen saturation by pulse oximeters and clinic home monitoring, permitted an early detection of any deterioration, facilitating timely interventions.
A systematic review 26 was conducted to evaluate the reliability, validity, and responsiveness of digital devices measuring SpO2 and respiratory rate in COPD patients in remote settings, assessing their reliability, convergent and concurrent validity, and predictive validity of SpO2 and respiratory rate devices, if compared to other monitoring methods.
A Japanese multicenter, 27 prospective study has investigated the feasibility and acceptability of telemedicine among COPD patients and physicians, specifically through a telemedicine app, which included daily symptom tracking and weekly questionnaire. Both the participants’ compliance, with completing the questions, and the app’s acceptability among participants and healthcare providers, assessed via questionnaires at the end of the study, appeared positive. The study also examined the impact of Japan’s COVID-19 state of emergency on the results, with no significative difference before and after the pandemic.
Wu et al. 28 examined the patient and clinician perspectives on remote deliver of COPD care during COVID-19. Most clinicians felt capable of remotely assessing symptom severity (95%), reinforcing smoking cessation (84%), and directing patients to other healthcare resources (80%). Patients reported that remote care effectively addressed the assessment of COPD severity and the initiation of new medications. These findings highlight that while many aspects of COPD care can be effectively managed remotely, certain elements may still require in-person interactions. The study underscores the importance of understanding both clinician and patient perspectives to optimize remote care delivery for COPD patients.
According to the literature,29 –32 our system supports telemedicine as a valuable tool for monitoring and self-management of patients with COPD. Home monitoring is one of the methods of using telemedical technologies aimed to provide care at home and maintain a connection between patients and healthcare providers. COPD is a significant global health issue, with substantial economic and social challenges. Telemedicine could potentially improve care for patients with limited healthcare access and enhance self-management. 33 It may favor continuity of care during the transition from hospital to home and vice versa, offering greater accessibility and potentially reducing the average cost per patient. Overall, telemedicine programs, such as tele-rehabilitation, health education, self-management, early COPD exacerbation detection, psychosocial support, and smoking cessation demonstrated a trend of non-inferiority compared to traditional COPD management, offering a promising solution for delivering quality healthcare while ensuring patient safety, especially during the pandemic. 33
The ability to monitor patients through thorough assessments, including peripheral SpO2 and HR at rest and during exertion, also provides the opportunity to track various parameters during daily activities, which is particularly useful in rehabilitation. 32
The high acceptance rate of the remote monitoring service is a notable finding of this study. The median answering ratio, a measure of patient participation, was 92% overall, with no significant difference between patients with and without COPD. This suggests that the service was well-received and considered manageable by most patients, regardless of their respiratory health status. Several factors likely contributed to this high acceptance rate. Firstly, the efforts made to bridge the digital divide by employing a variety of remote communication techniques, ranging from basic phone calls to tele-visits and tele-consultations with specialists, ensured accessibility for patients with varying levels of technological comfort and access. Secondly, the involvement of cultural mediators helped to overcome potential language and cultural barriers, making the service more inclusive and user-friendly. Finally, the active participation of patients’ general practitioners ensured continuity of care and facilitated communication between patients and the healthcare system. These strategies likely fostered a sense of trust and comfort among patients, encouraging their active participation in the program. The positive response to the service underscores the potential of remote monitoring to effectively engage and support patients during a pandemic, especially when tailored to address individual needs and circumstances.
As reported in the literature,34 –37 home monitoring for COPD patients can enhance medical care and disease management, despite some challenges and barriers to widespread adoption. Engaging end-users in the assessment and co-design of new telemonitoring solutions could significantly refine the effectiveness of remote monitoring for COPD in the near future.
Finally, beyond its value during the COVID-19 pandemic, this study highlights the potential of telemedicine to provide real-time information on patients’ conditions in their natural, free-living environments.38 –42 This capability offers a significant clinical opportunity to monitor patients’ health status continuously, detect subtle changes or early signs of deterioration, and intervene promptly to prevent adverse events. Telephone consultation by healthcare professionals to patients with COPD during the SARS-CoV-2 pandemic offers an example of the importance of adapting clinical approaches to maintain patient care as well as minimizing the risk of virus transmission, in addition to being a fast, easy, economical, and accessible modality. 42
This finding could inform the use of telemedicine for other chronic respiratory diseases, such as asthma, as well as for other chronic conditions that require regular monitoring and management.
Telephone assistance permits the assessment of needs in patients with chronic respiratory diseases, which can range from follow-up of clinical conditions to arranging an in-person visit or urgent care. A phone call is a valuable resource when the health issue is well-identified and only follow-up and treatment adjustments are needed. With a telephone consultation, we can avoid the need for the patient and professional to travel, manage situations of fear or uncertainty, save time for both the patient and the professional. Telephone consultations may become a common practice in patient care, necessitating the development of new models to follow. 41
Moreover, this continuous stream of real-time data opens up new avenues for research, enabling studies that were previously limited by the constraints of traditional hospital-based settings or episodic observations during acute events or exacerbations. Telemedicine, therefore, has the potential to not only transform clinical practice but also reshape the landscape of COPD research, leading to a deeper understanding of the disease and the development of more effective interventions. 37
This study acknowledges several limitations. Firstly, the sample size of COPD patients was relatively small, which may limit the generalizability of the findings to the broader COPD population. Secondly, the study was conducted during the COVID-19 pandemic, and the inclusion criteria specifically targeted COVID-19-positive patients. This may affect the applicability of the results to COPD patients in non-pandemic situations or those who are not infected with COVID-19. Furthermore, this study relied on previously documented diagnoses of COPD, and the specific methods used for these prior diagnoses (e.g., spirometry confirmation vs clinical assessment) were not collected as part of the COD19 service protocol, which may influence the characterization of the COPD cohort. While smoking status (categorized as never, ex-, or current smoker) was adjusted for, more granular data such as pack-year history or objective measures of COPD severity (e.g., GOLD stage, baseline spirometry) were not systematically available within the COD19 platform dataset. Additionally, the monitoring duration was relatively short, which may not capture long-term trends and outcomes in COPD patients. The comparative analyses adjusted for age, sex, BMI, and smoking habits; however, data regarding other specific comorbidities (beyond the presence/absence of COPD) or indicators of baseline COVID-19 severity were not uniformly collected as part of the COD19 service protocol and thus could not be included in the adjustment models. The potential for residual confounding due to these unmeasured factors represents a limitation. Finally, the study primarily focused on physiological parameters and did not assess clinical outcomes related to COPD, such as exacerbations, hospitalizations, or quality of life. Future studies with larger sample sizes, longer monitoring durations, and inclusion of clinical outcomes could provide a more comprehensive understanding of the effectiveness of telemedicine in managing COPD.
Conclusion
By utilizing the COD19 platform, we monitored COPD patients throughout the pandemic, ensuring continuity of care and seamless transitions between home and hospital. The system provided excellent accessibility, facilitating consistent monitoring and timely interventions. The significance of telemedicine platforms is evident not only during pandemics but also in situations requiring patient isolation. These technologies have proven highly effective in managing chronic conditions, enabling early detection of complications, and improving long-term patient outcomes. Adapting the COD19 active surveillance model for routine detection of COPD exacerbations outside of pandemic or isolation contexts would likely necessitate modifications. Alert thresholds might need recalibration to focus more specifically on established indicators of exacerbation, such as significant increases in dyspnea or changes in sputum characteristics, perhaps combined with SpO2 trend analysis, rather than the acute infection parameters prioritized here. Furthermore, integrating validated patient-reported outcome tools or electronic symptom diaries could significantly enhance the system’s sensitivity and utility for early exacerbation detection in standard care pathways. Future research should aim to compare the effectiveness, applicability, and cost-effectiveness of different telemedicine modalities (e.g., active surveillance like COD19, tele-rehabilitation, symptom-tracking mobile applications) across diverse COPD patient populations and healthcare settings to better tailor remote management strategies. As healthcare continues to evolve, telemedicine stands as a crucial frontier, shaping the future of patient care and accessibility.
Supplemental Material
sj-pdf-1-tar-10.1177_17534666251346097 – Supplemental material for Active home surveillance system (COD19) in managing chronic obstructive pulmonary disease: lessons and future perspectives from the COVID-19 pandemic experience
Supplemental material, sj-pdf-1-tar-10.1177_17534666251346097 for Active home surveillance system (COD19) in managing chronic obstructive pulmonary disease: lessons and future perspectives from the COVID-19 pandemic experience by Andrea Foppiani, Valeria Calcaterra, Chiara Montanari, Simona Bertoli, Alberto Battezzati and Gianvincenzo Zuccotti in Therapeutic Advances in Respiratory Disease
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.