
Abstract
Background:
People with cystic fibrosis (pwCF) are increasingly considering their reproductive options. Currently, there are many genetic testing options available for pwCF and their reproductive partners. Healthcare providers, including genetic counselors, can educate pwCF about these options and support them through the decision-making process.
Objective:
This study explored the role of genetics in the reproductive decisions of pwCF and their perspectives and experiences surrounding prenatal and preconception genetic counseling and testing.
Design:
We conducted a qualitative study of a national US sample of pwCF age ⩾18 years recruited from the CF Foundation Community Voice platform.
Methods:
We conducted and recorded semi-structured telephone interviews with participants. We utilized Dedoose software and applied inductive thematic analysis to code the interview transcripts and elicit themes.
Results:
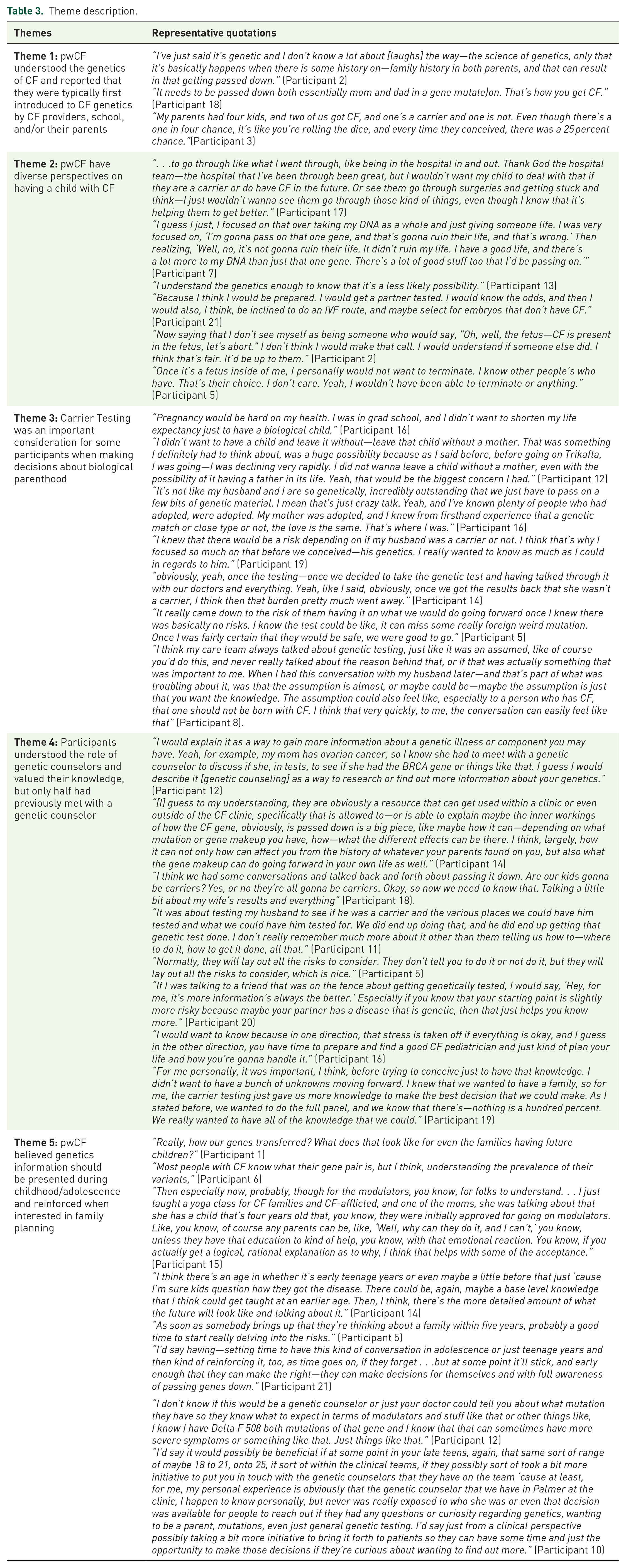
We interviewed 21 participants (76.2% women, 95.2% White, 4.8% Hispanic, 57.1% parents, 23.8% considering parenthood). Key themes included: (1) pwCF appeared to understand the genetics of CF and were typically first introduced to CF genetics by CF providers, school, or their parents; (2) pwCF had diverse perspectives on having a child with CF; (3) carrier testing was an important consideration for some participants when making decisions about biological parenthood; (4) participants understood the role of genetic counselors and valued their knowledge, but only half previously met with a genetic counselor; (5) pwCF believed genetics information should be presented during childhood/adolescence and reinforced when interested in family planning.
Conclusion:
pwCF have discrepant views on passing on CF to future offspring, and although there is recognition of the role of genetic counseling and a desire for knowledge from genetic testing, genetic considerations are but one factor involved in parenthood decisions. Future work should develop patient-, provider-, or system-based interventions to best integrate high-quality genetics and genetic counseling care into the CF team for those with CF considering parenthood.
Plain language summary
More people with Cystic Fibrosis (pwCF) are thinking about becoming parents. Since, Cystic Fibrosis (CF) is a genetic condition, we wanted to understand if genetics plays a role in making decisions about whether to become parents or not. We also wanted to understand pwCF’s thoughts about prenatal genetic counseling and testing. We interviewed 21 pwCF and analyzed their interview transcripts and developed 5 themes. 1) pwCF understand CF genetics, 2) pwCF have different views on having their own child with CF, 3) carrier testing is important for making parenthood decisions, 4) pwCF understand the role of genetic counselors but many have never met with one, 5) genetics information should be discussed when pwCF are younger. Future studies should try to implement interventions to introduce more genetic counseling and testing services into the CF care team.
Keywords
Introduction
Available therapies for people with cystic fibrosis (pwCF), including CF transmembrane conductance regulator (CFTR) modulators, have led to many pwCF living longer and considering their reproductive options. Previous work has shown that 84% of males and 78% of females with CF wish to have children.1,2 In addition, a doubling of pregnancies among pwCF has been documented in the United States with the widespread use of CFTR modulators. 3
Many pwCF have concerns about genetic inheritance when they are considering parenthood. One survey found that 72% of females with CF were worried that their future children would have CF, and 79% said that they would want their partners to undergo CF genetic testing for future children. 2 Attitudes toward and acceptance of prenatal screening are also influenced by the timing of what is offered. One Australian survey found that while 93% of pwCF agreed that preconception CF carrier screening should be offered to the general prenatal population, there was a marked decrease in support for carrier screening among pwCF once a couple is pregnant. 4 Views on the purpose of CF carrier screening also vary among pwCF; in another study, nearly all pwCF agreed that the goal of preconception CF carrier screening was to educate couples about the chance of their children inheriting a genetic disease; approximately half felt that the goal of CF carrier screening was to “avoid births of all children with CF.” 5
In addition to CF carrier screening, there are other pre-conception, prenatal, and postnatal genetic testing options available for pwCF to learn more about their chances of having a child with CF (Table 1). Assisted reproductive technologies (ART) such as in vitro fertilization (IVF), which is commonly utilized by males with CF who have primary infertility due to congenital bilateral absence of the vas deferens, incorporates genetic testing to screen embryos for chromosomal aneuploidy and known variants for genetic conditions before embryo selection. When CFTR pathogenic variants have been identified in the reproductive partner of a pwCF, IVF with preimplantation genetic testing for monogenic disorders (PGT-M) can be utilized to screen for embryos with CF. 6 During a pregnancy, prenatal diagnostic testing can be done by obtaining a sample of fetal cells through chorionic villus sampling (CVS) or amniocentesis. However, both CVS and amniocentesis carry a risk of miscarriage or pre-term labor, which may deter some pregnant individuals from pursuing these options. 7 Analysis of cell-free fetal DNA from maternal blood is a non-invasive prenatal screening method available for CF on a limited basis. A finding of an echogenic bowel on a 20-week anatomy ultrasound increases the risk for CF, among other conditions, and would prompt a discussion of carrier and prenatal diagnostic options to inform pregnancy management decisions, including birth planning with a multidisciplinary team. 8 Infants with CF can be identified after birth through newborn screening (NBS), which incorporates analysis of a panel of CFTR variants in all US states. Of note, NBS does not detect all infants with CF; some may be diagnosed later in life based on the presentation of symptoms and diagnostic testing. For pwCF taking CFTR modulators during pregnancy, there is a risk of a false negative NBS result due to lowered immunoreactive trypsinogen evaluation in the infant 9 ; diagnostic evaluation via sweat chloride testing and genetic analysis is recommended.
Genetic testing options available for pwCF to learn more about their chances to have a child with CF.

With the abundance of genetic information and genetic testing options available for pwCF pursuing parenthood, speaking to a genetic professional, like a genetic counselor, may help pwCF navigate these choices. Genetic counselors can educate pwCF and families about genetic inheritance, review the benefits and limitations of available genetic testing, and discuss family-building modalities including ART, donor sperm, and adoption. Studies that have investigated genetics knowledge and exposure to genetic counseling among pwCF are limited in number but have demonstrated gaps in knowledge.10,11 A recent genetic counseling intervention among pwCF considering parenthood found that, following implementation, genetics knowledge improved. 12
The views and experiences about preconception and prenatal genetic counseling among pwCF have not been explored in the era of widespread CFTR modulator use. In addition, the impact of genetic information on how pwCF perceive their reproductive futures has not been previously assessed. Therefore, we aimed to explore the role of genetics in the reproductive decisions of pwCF and their perspectives and experiences regarding preconception and prenatal genetic counseling and testing.
Methods
The reporting of this study follows the consolidated criteria for reporting qualitative research (COREQ) statement. 13 This checklist is included in Supplemental Figure 1.
Recruitment
We recruited participants who had a diagnosis of CF, were 18 years of age or older, and spoke English. Between October and November 2023, we advertised the study via CF Foundation Community Voice (a platform for pwCF and family members of pwCF to learn more and elect to participate in CF research studies 14 ). Community Voice members received emails containing study details and a linked interest survey (Supplemental Figure 2). We sent a subsequent email to survey respondents with a request to schedule an interview via the principal investigator’s Calendly page.
Interview design
We developed a study interview guide (Supplemental Figure 3) with input from our multidisciplinary research team, which includes clinicians and researchers with experience working with the CF population and a faculty member with experience in health communication. We confirmed the face validity of our interview guide using the clinical expertise of our research team. We did not formally pilot test our interview guide before we began data collection. GR, a female graduate student in genetic counseling, conducted all interviews. Prior to the interviews, we assured that all participants were made aware through email communication about the aims of the study, what results would be utilized for, and GR’s status as a genetic counseling graduate student. The only communication with GR prior to interviews was for scheduling purposes. We obtained verbal consent and confirmed that participants met the inclusion criteria as above before beginning each interview. We conducted interviews between November 2023 and January 2024 and compensated all participants with an electronic gift card.
GR asked participants about their understanding of CF inheritance, their discussions with healthcare providers about genetics and genetic testing, experiences with genetic counselors, views on genetic testing, and the impacts of genetics on family planning. GR conducted these interviews over the phone in a private room to ensure confidentiality for participants. No one was present during these calls except for the interviewer and the participant. We interviewed each participant only once, and interviews typically lasted between 30 and 40 min. No field notes were made during or after the interviews.
Data analysis
All interviews were audio-recorded, with participant consent, and transcribed verbatim by a third party. We did not return transcripts to participants for correction or comments. GR and AP, a bachelor-level research coordinator, analyzed interview transcripts using inductive thematic analysis. We each read 20% of the transcripts and then discussed our identified codes. Following this discussion, we read an additional 20% of transcripts. We discussed any disagreements thoroughly before coming to a consensus. We then coded all transcripts using the final codebook with Dedoose software, 15 and identified no new codes, therefore achieving data saturation. We consolidated the codes into significant themes and identified representative quotations. Study participants did not provide feedback on the identified themes.
Results
Thirty individuals filled out the interest survey, and 21 subsequently scheduled an interview. We interviewed all 21 pwCF (age range 18–74 years; 16 women). Twenty self-identified as White, and one identified as Hispanic. Participant demographics are listed in Table 2.
Patient demographics.

The majority (n = 12) were already parents, and one-third (n = 7) were considering parenthood. Two participants had decided against pursuing parenthood. Of the parent participants, nine had biological children, two had pursued adoption, and one had pursued ART using a sperm donor. Of those considering parenthood, six were considering biological parenthood, and one was adoption. Eleven participants or their reproductive partners had met with a genetic counselor, out of which 10 participants were already parents.
Identified themes
Key themes and representative quotations are shown in Table 3 and discussed in detail below.
Theme description.
Theme 1. pwCF understood the genetics of CF and reported that they were typically first introduced to CF genetics by CF providers, school, and/or their parents
Most participants could describe recessive inheritance and demonstrated an understanding of CF genetics. One participant succinctly shared, “It is . . . homozygous recessive. You have to have two recessive copies to create [a person with] CF” (Participant 5). When asked about CF inheritance, some participants also discussed the risks associated with two carriers having a child with CF. One participant commented, “If both parents have a copy of the gene, there’s a one in four chance that the child will have CF” (Participant 8). While participants understood concepts surrounding CF genetics and recessive inheritance, many used different phrasing to describe CF-causing mutations or pathogenic variants. Some used the term “mutated” or “mutation” or “defect.” Other participants referred to CFTR mutations instead as a “CF gene,” “recessive gene,” or “pathogenic variant.”
Participants described several ways in which they first learned about CF genetics. Some described first learning about CF genetics in a school setting: “Years ago, just eighth-grade biology. You learn about genetics” (Participant 5). Others reported that they learned about CF genetics from a healthcare provider: “I don’t have a distinct memory, but I think it was that I—at one of my routine visits, I think a doctor explained it to me that way when I was probably around 10 or so, probably, I wanna say” (Participant 2). Some initially heard about CF genetics from their parents or from a combination of their CF provider and their parents and a few reported learning about CF genetics through independent research.
Theme 2. pwCF have diverse perspectives on having a child with CF
Participants had differing levels of concern about passing CF on to biological children. Their perspectives had a myriad of influences: personal experiences with CF and CF modulators, understanding of genetics and risks, and views related to the termination of pregnancies with a CF diagnosis. One participant shared:
“I think it would’ve been incredibly selfish. It’s hard. It’s just so hard having CF. . . . It’s an early death, and I just would have not been able to look my child in the face if they were going in the hospital, getting IV treatments, and having to think that I knew this was a possibility, because I have CF and I put them through that. That would’ve broken me” (Participant 3).
Another participant said: “Well, because I didn’t wanna watch them suffer and knowing I had given that to them because growing up, my mom used to sit there and cry and say, ‘I’m so sorry I gave this to you, if we had only known.’ That really made an impression on me” (Participant 16).
Other participants expressed less concern about passing CF to their biological children. One participant shared: “I don’t know if I was just sort of naïve at the time when I was thinking about having biological children or not thinking it through, really [laughter], but I don’t know. It just wasn’t a huge fear of mine. I guess it just goes back to feeling like that wouldn’t be the worst thing” (Participant 11). Others noted that quality of life with CF has improved, making life less difficult: “I don’t feel like it would be the same feeling now because of the medications and things that are out there. I think that—I mean, the fact that they can start Trikafta [CFTR modulator] with babies very young, those babies would live a very different life” (Participant 9).
Because modulator eligibility is typically based on the specific CFTR mutations a pwCF has, we asked participants about their concerns about having a child with CF who was ineligible for CFTR modulators. One participant shared: “That would definitely come up, for sure. Just seeing the patients who have not been able to at least try the modulators and be eligible for that. I would definitely be concerned about that now, for sure, having one rare mutation” (Participant 19). Others were less concerned and expressed faith in the development of new treatments: “I only know two people that are not eligible for the modulators. I honestly just have full faith that things—and maybe it’s a horrible way to look at it—but I have full faith that with CFF [Cystic Fibrosis Foundation], as wonderful as the foundation there, that they’ll find something else that works for those who can’t take Trikafta [CFTR modulator]” (Participant 1).
Some participants reported that they were less concerned because they would consider pursuing genetic testing and/or IVF to avoid having a child with CF:
“Not really, mainly because I feel like there’s a lot of steps you can take . . . There’s been embryo testing. There’s IVF. There’s all these paths you can take to avoid having a child with CF. I’m not so much worried about that. Although I appreciate that there’s still always going to be a non-zero probability that a child with CF could be born to us as a result of some previously unknown mutation” (Participant 6).
Perspectives surrounding the termination of pregnancies with a CF diagnosis influenced participants’ views on having a child with CF as well. One participant revealed that they did not support termination of pregnancies with a CF diagnosis: “I’m not really comfortable with the idea of selective abortion for CF either. It’s a little bit too close to home [as a person with CF]” (Participant 16). Some participants thought that genetic testing for CF during pregnancy and decisions regarding the future of the pregnancy should be an individual decision: “That’s an impossible situation. It was a very, very hard question and one that nobody could tell somebody else what to do. I think that ultimately has to be the choice of the two parents, and I would really hope that whatever choice they made was just not shamed by others because nobody can understand what somebody’s individual situation is” (Participant 19).
Participants had different views regarding the utility of genetic testing during pregnancy. For example, one participant revealed that they were not sure if they would decide to terminate the fetus with a CF diagnosis, but they would want the information to make a well-informed decision: “I don’t know, it might inform my decision to do something. I can’t say that I would necessarily terminate a fetus. I can’t put myself in the future knowing how I would feel in that situation, but I would certainly want the information so that I can make that decision” (Participant 6).
However, other participants revealed that they would not consider terminating a fetus with a CF diagnosis, so they would not pursue genetic testing during pregnancy, as shown in the following example:
“I think that that’s something that I would understand why someone would potentially do. I don’t know if that’s something that I would pursue or not myself, given that I know what CF is, I know what goes into having CF, and I know it wouldn’t make a decision for me in terms of if I am already pregnant, what I want to do—if I want to continue with that pregnancy” (Participant 13).
Theme 3. Carrier testing was an important consideration for some participants when making decisions about biological parenthood
One important genetic consideration for many participants was their reproductive partner’s CF carrier status. Some participants revealed that when their partner’s carrier status came back negative, they felt more comfortable pursuing biological parenthood, as seen in the following example: “Once we found out that my husband wasn’t a carrier, then I really didn’t have a problem with it [pursuing biological parenthood]” (Participant 7). Another shared: “It influenced me in the sense that with the carrier testing, I felt much more at ease that the chances of bringing somebody into the world with CF were so low. I think it put me at ease. . .” (Participant 3).
Although many participants found carrier testing results helpful in making their parenthood decisions, some felt pressure from their healthcare team. For example, one participant who described negative reactions from her healthcare team:
“My husband and I had actually started trying already when it [carrier testing] was brought up at my CF clinic. I had some pretty negative reactions from a few of my people on the CF team, like really, really awful, telling me like, ‘How could I do this? How could I do this to a baby? . . . which is hard to hear that somebody thinks having a person be born with CF is the worst thing that could happen to a person . . .” (Participant 11).
This participant and her partner underwent CF carrier testing, reporting:
“I kinda went into it reluctantly . . . I know it is the right thing to do, to do genetic testing to avoid having a child with CF, but it’s hard, too, to be like, ‘Oh, nobody would want a baby with CF.’ I am a person living with CF and—I don’t know. It was just a really difficult time to sort of get to a place where I was like, ‘Okay, yeah, let’s do this testing,’ mostly because everybody wanted us to do it” (Participant 11).
Many participants reported that rather than pursuing unassisted conception, they instead considered other options for becoming a parent to limit the likelihood their child would have CF, like adoption or ART. For example, one male participant who pursued parenthood via ART using a sperm donor reported:
“I don’t have an ego about that enough where—I’ve known friends who either were adopted or who adopted kids, and I know that—I’m very logical believer that your family is not limited to just who you’re biologically related to, and so I always just felt like, well, there’s a lot of options out there other than having biological children and I would be totally comfortable with both. Sure enough, my daughter is—she’s my world. She’s amazing and I just love her so much and I don’t feel like my feelings for her would be any different if I were—if she actually shared my DNA or not” (Participant 2).
Theme 4. Participants understood the role of genetic counselors and valued their knowledge, but only half had previously met with a genetic counselor
Most participants understood the role of a genetic counselor. Participants valued gaining knowledge about CF genetics and preparing for potential children with CF. However, only around half of our participants or their partner had ever experienced preconception or prenatal genetic counseling themselves. Participants also revealed challenges with accessing and receiving genetic counseling services.
Some participants described genetic counselors as individuals that could help one learn more about their own genetic information and genetic risks: “I would say that they could be a great person to try and find out more about your genetics on the regard of if you happen to have any mutations yourself” (Participant 10). Participants also described genetic counselors as a resource to ask questions: “Educate someone on their condition, their genetic modification and just be a resource to questions about it. I feel like for us, it was more of an opportunity to understand how it happened, like how this could happen, and also for us, it was also like what next” (Participant 18).
Participants also believed that genetic counselors could provide more nuanced information about genetic risks. For example, one participant described: “I think—when we talked about CF—she mentioned the carrier rates for my ethnic background and the carrier rates from my husband’s ethnic background, things like that, so that people would understand, basically, how the odds work for each of these diseases that they could potentially pass on to a child” (Participant 6).
Another component of a genetic counselor’s role that participants highlighted was the discussion of genetic testing, including the types of genetic testing and knowledge that would be obtained following testing. For example, one participant described: “[Genetic counselors] Really have that conversation with them to make sure people are well informed about the types of testing that’s out there to help them make the best decision for themselves whether to move forward with genetic testing or not” (Participant 1). Another participant described how genetic counselors can review the results of the testing with their patients: “Then to kind of recommend and prescribe the testing that goes forward with it, and then analyzing and reviewing the results of the testing, and what risks or complications the couple might encounter if they do reproduce” (Participant 15).
Although most participants understood and valued the role of genetic counselors, only half of participants or their reproductive partner met with a genetic counselor. Some participants revealed concerns surrounding access to genetic counselors and current information genetic counselors know about CF. For example, one participant discussed how pwCF may not be aware about genetic counseling: “. . .Some people don’t even know genetic counselors exist. . .” (Participant 5). Another participant said they were unsure how to make a genetic counseling appointment or where to access that information: “Would they ask their doctor to get that genetic counseling appointment? How do they go about doing that?” (Participant 12).
Another concern expressed was whether or not genetic counselors had up-to-date information about CF prognosis. One participant shared:
“It’s like what kind of information are people getting about actual life with CF? I talked to one family one time, in my role at work, where they found out that they’re 20—she was like 20 weeks along when they found out that she had CF. They were calling because they were thinking about terminating the pregnancy. They wanted to talk to a parent, ‘cause they didn’t think they could do it. . . They reported to me that their genetic counselor gave them a lot of scary information . . . CF has changed so fast. Do [genetic counselors] have the knowledge of current treatments to help people make that decision?” (Participant 8).
Theme 5. pwCF believe genetics information should be presented during childhood/adolescence and reinforced when interested in family planning
Most participants believe genetic information such as recessive inheritance, personal mutations, and CFTR modulator eligibility, should be presented during childhood/adolescence and reinforced when interested in family planning. One participant shared: “I think a basic understanding of how genetics works in terms of reproductive health and children feels important, recessive genes versus dominant genes and some level of understanding on that, feels like a base level of knowledge that potentially everyone should be aware of” (Participant 13).
Another participant commented: “I think people with CF should know what mutations they have. I was told that when I was young. I’ve always known. I think it’s important because a lot of times especially for the age I was born, that paper copy is gone. If I didn’t know, I’d have to get retested ‘cause it’s not in my paper records. I have no idea where that paper is” (Participant 7).
Many participants believed that genetic information should be first introduced to pwCF during childhood/adolescence:
“It’s probably something that the conversation needs to start happening in pediatrics. I know it was something I was thinking about before I even had my first boyfriend in years and years before I was sexually active or even thinking about—like realistically thinking about having children, but it was still playing into my decision or long-term decision making” (Participant 13).
In addition, some participants thought CF genetics information should also be communicated when a pwCF is at an age to consider family planning: “[I] would also assume that most people when they’re still at pediatric clinic are not at a stage of their life where they’re considering having children, so it’s probably more impactful to do it in an adult clinic format, where somebody might be approaching an age where they’re considering having children” (Participant 6).
Discussion
pwCF have an understanding of CF genetics and displayed a wide range of views on the role of genetics in their reproductive decisions. These views were influenced by participants’ personal experiences with CF and CFTR modulators, their understanding of genetics and risks, and their views about pregnancy termination due to a prenatal CF diagnosis. Many participants commented on the importance of knowing their partner’s CF carrier status before making a parenthood decision. Participants were knowledgeable about the role and value of genetic counselors; however, only half of our participants had met with a genetic counselor, meaning such services seem underutilized.
Our results align with prior studies exploring genetics knowledge among pwCF. Conway et al found that >80% of surveyed pwCF understood that both parents of a pwCF were carriers and would have a 25% chance of having another child with CF for each pregnancy. However, only half understood that a pwCF would pass on a CF-causing variant to their children, making each one at least a carrier. 11 Another study found that, while 70% of pwCF understood the chances of two carriers having a child with CF, only one-third knew the risks of a pwCF and a CF carrier having a child with CF. 16
Participants reported learning about CF genetics from conversations with CF providers or their parents, information taught at school, or independent research. If pwCF are learning about CF genetics from their parents, parents must understand it. Boyer et al assessed parents of pwCF’s understanding of CF and their discussion of CF with their unaffected children and found that 71% of parents had discussed CF genetics with their unaffected children. 17 While most of our participants were well-informed about CF genetics, based on the misconceptions reported in previous studies,11,16 it is essential for pwCF to be informed specifically about their own risks of having a child with CF or a carrier. Genetic concepts should be reinforced by trusted healthcare providers, including genetic counselors and the CF team.
Prior studies report that pwCF are concerned about their children also having CF.2,18 However, our participants reported a range of views on whether having a biological child with CF was a concern or not. These views were influenced by multiple factors, including personal experiences with CF, the availability and effectiveness of CFTR modulators, and expressed faith in the development of future treatments for those who are currently ineligible. Our results highlight that it is important for healthcare providers of pwCF, including genetic counselors, to recognize that having a child with CF is not a concern for all pwCF and assess their patient’s goals and priorities in a client-centered manner.
Participants also had mixed opinions about whether they would pursue prenatal genetic testing for a fetus during pregnancy to determine a CF diagnosis as well as whether or not to terminate a pregnancy based on CF diagnosis. These findings align with the work of Conway et al, which found that the majority of pwCF would pursue prenatal genetic diagnosis if they knew their partner was a CF carrier. 19 The authors also found that 68% shared that abortion can be considered if a fetus has CF, but only 23% would choose to terminate a pregnancy of a fetus with CF. 19
Similar to prior studies, many of our study participants’ decisions surrounding biological parenthood were strongly influenced by their reproductive partner’s CF carrier testing result. 20 The information gained from testing could help with considerations surrounding birth planning, monitoring for echogenic bowel, preparing for a baby and parent with CF, prenatal exposures to CFTR modulator therapy, planning for a sweat test, termination of pregnancy, or deciding against biological parenthood. However, this desire to pursue genetic testing was not universal. Several participants shared that they felt pressure from their healthcare providers for their partners to pursue carrier testing before making reproductive decisions. These results underscore that genetic testing should be a personal decision. PwCF should be educated about carrier testing and supported through an informed decision-making process, but not coerced into making such decisions. 21 Genetic counselors are trained specifically to provide education about genetic testing, in a nondirective fashion, and therefore, would be a qualified healthcare provider for pwCF with whom to discuss carrier testing.
Only half of our participants or their reproductive partners had ever met with a genetic counselor. This is comparable to a 2019 study that found that 57% of pwCF interviewed had previously met with a genetic counselor 22 and increased from an earlier study where only 27% of pwCF surveyed reported that they were referred for genetic counseling. 23 Considering previous studies have reported that around 80% of pwCF wish to have children, genetic counseling is being underutilized in this population.1,2
Potential reasons for the underutilization of genetic counseling services include significant access barriers. For example, currently, Medicare does not recognize genetic counselors as healthcare providers, which presents financial and insurance barriers. 24 U.S. federal legislation recognizing the healthcare role of genetic counselors may improve access and use of these services. Individuals living in rural areas may face geographic barriers to access genetic counseling services, given the scarcity of providers. Telemedicine and/or satellite clinics are potential ways to overcome this barrier. 25 Additionally, some U.S. states do not have genetic counseling licensure in place. This can lead to genetics services being provided by inadequately trained professionals. 26
Most of our participants correctly identified the core features of a genetic counselor’s role. In contrast, Wilson et al found a lack of knowledge among pwCF regarding genetic counseling and what was discussed during such an appointment. 22 Similarly, a 2023 study found that genetic counseling and planning, including partner carrier screening, were important in helping pwCF make decisions regarding parenthood. 27
Several of our participants raised concerns about genetic counseling, such as awareness and access to these services as well as whether genetic counselors had up-to-date information about CF prognosis and treatments. Level of association between genetic counselors and CF care centers has been shown to influence CF clinician’s views of genetic counselors’ expertise, value, and accessibility in the setting of CF NBS. 28 Elsas et al surveyed prenatal genetic counselors in 2013 about their knowledge of ivacaftor, the first approved CFTR modulator. They found that 80% were unfamiliar with this drug and would not feel comfortable discussing it with patients, but would refer to a CF specialist. 29 Unpublished data from a 2020 survey of prenatal genetic counselors conducted following the 2019 approval of elexacaftor–tezacaftor–ivacaftor found that nearly all respondents had heard of CFTR modulators and most would refer individuals with a prenatal diagnosis of CF to a specialist to discuss elexacaftor–tezacaftor–ivacaftor. 30
pwCF value education about CF genetics starting in childhood/adolescence and re-addressed when they are more interested in family planning. Currently, there are tools being developed to provide pwCF making reproductive health decisions with appropriate information, including information about genetics and heritability of CF.31,32 Future development and effectiveness and implementation testing of such patient-facing interventions are needed. Specifically, clinical interventions for adolescents with CF are needed. Additionally, development is warranted for provider-facing trainings related to reproductive health communication with pwCF and systems-based interventions to ensure universal education and care provision for all reproductive-age pwCF. The values-based, client-centered tenets of genetic counseling33,34 emphasize non-directiveness in the reproductive setting, such that providers discussing reproductive genetic testing should provide education about a range of options, and support client’s informed decisions. As our interviews show, prenatal or preconception genetic testing is not desired by all pwCF and their reproductive partners, and their goals for seeking testing may be to prepare for having a baby with CF rather than prevention.
This study had limitations. As with any qualitative study, our population may not be representative of pwCF as a whole. Our participants were all recruited via the CF Foundation Community Voice, an opt-in program, which implies that, at baseline, participants were highly motivated to participate in research studies and are potentially more knowledgeable about CF genetics. Another limitation is that we had a relatively homogenous population regarding race/ethnicity. As genetics services in general are underutilized in minority populations, 35 pwCF from minoritized racial and ethnic backgrounds may have different lived experiences regarding genetic counseling and testing from our participants, nearly all of whom were White. This limited diversity in our study population may limit generalizability. Therefore future studies should intentionally focus on and include pwCF from minority populations. Finally, as with all qualitative studies, the positionality of the interviewer and coders may shape the interview interactions with the study participants and interpretations of the data. In addition, we did not pilot our interview guide prior to conducting our interviews, which could limit how effective the questions were. To mitigate bias, we intentionally reviewed the interview guide, codebook, and analyses with the research team. However, future studies could incorporate external coding validation or participant feedback. Finally, as pwCF who were born around the introduction of CFTR modulators grow older and begin considering their reproductive futures, it will be important to explore their perspectives on having future children with CF and prenatal and pre-conception CF genetic testing.
Conclusion
Our findings highlight that pwCF value a personalized, client-centered approach to offering genetic testing and providing genetic counseling services as they consider parenthood. We believe that future work should develop patient-, provider-, and/or systems-based interventions to best integrate high-quality genetics and implement recent CF Foundation recommendations to include genetic counselors on CF care teams. 36 In addition, all health care providers discussing pregnancy and genetic testing should be trained in a nondirective approach to discussing reproductive genetic testing. This would allow for improved access to comprehensive reproductive healthcare for all pwCF, especially for those who are making decisions surrounding parenthood.
Supplemental Material
sj-docx-1-tar-10.1177_17534666251340334 – Supplemental material for Perspectives of people with cystic fibrosis considering parenthood surrounding preconception and prenatal genetic counseling and testing
Supplemental material, sj-docx-1-tar-10.1177_17534666251340334 for Perspectives of people with cystic fibrosis considering parenthood surrounding preconception and prenatal genetic counseling and testing by Gopika Rajanikanth, Asher Prangley, Olivia M. Stransky, Elinor Langfelder-Schwind, Jodie Vento, Elizabeth Felter and Traci M. Kazmerski in Therapeutic Advances in Respiratory Disease
Supplemental Material
sj-pdf-2-tar-10.1177_17534666251340334 – Supplemental material for Perspectives of people with cystic fibrosis considering parenthood surrounding preconception and prenatal genetic counseling and testing
Supplemental material, sj-pdf-2-tar-10.1177_17534666251340334 for Perspectives of people with cystic fibrosis considering parenthood surrounding preconception and prenatal genetic counseling and testing by Gopika Rajanikanth, Asher Prangley, Olivia M. Stransky, Elinor Langfelder-Schwind, Jodie Vento, Elizabeth Felter and Traci M. Kazmerski in Therapeutic Advances in Respiratory Disease
Supplemental Material
sj-pdf-3-tar-10.1177_17534666251340334 – Supplemental material for Perspectives of people with cystic fibrosis considering parenthood surrounding preconception and prenatal genetic counseling and testing
Supplemental material, sj-pdf-3-tar-10.1177_17534666251340334 for Perspectives of people with cystic fibrosis considering parenthood surrounding preconception and prenatal genetic counseling and testing by Gopika Rajanikanth, Asher Prangley, Olivia M. Stransky, Elinor Langfelder-Schwind, Jodie Vento, Elizabeth Felter and Traci M. Kazmerski in Therapeutic Advances in Respiratory Disease
Footnotes
Acknowledgements
We would like to thank the Cystic Fibrosis Foundation for funding this study. We would also like to thank the CFF Community Voice team for their assistance with recruitment for this study. Lastly, we would like to thank our study participants for their time and willingness to share their perspectives and experiences.
Declarations
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.