
Abstract
Background:
Cardiovascular disease (CVD) risks are increasing in people with cystic fibrosis (pwCF). While cholesterol levels were historically low in pwCF, higher levels after initiating highly effective modulator therapy (HEMT) have been reported. Mechanisms are unclear and there is little guidance on screening.
Objectives:
To evaluate serum lipid changes at multiple timepoints after ivacaftor initiation, and to assess current screening practices for CVD risk factors among CF providers.
Design:
This was a post-hoc correlative analysis of prospectively collected clinical data and serum samples from the GOAL cohort study. Cross-sectional survey methodology was also employed.
Methods:
We evaluated serum lipids (total cholesterol (TC), low-density lipoprotein (LDL), and high-density lipoprotein (HDL)) at baseline, 3- and 18 months after ivacaftor initiation using samples from the GOAL study biorepository. We also surveyed CF providers across the United States on their CVD risk screening practices.
Results:
Fifty GOAL participants’ samples were analyzed. Using the repeated measures model, TC significantly varied by visit (p = 0.004), driven by a significant increase from baseline at 3 months (mean difference 9.4 mg/dL). This difference diminished by 18 months. BMI was a significant covariate for TC. No significant differences by visit were detected in LDL or HDL. Seventy-five respondents participated in the survey (response rate 5.6%; 41 adult providers, 18 pediatric providers, and 10 providers caring for both) with 67% reporting no lipid screening policy existed in their center. In the past year, 29% of adult providers prescribed lipid-lowering therapy, 54% started anti-hypertensive medications, and 48% initiated ischemic cardiac evaluations for pwCF.
Conclusion:
TC significantly increased within 3 months of initiating ivacaftor, but subsequently diminished toward baseline by 18 months. Lipid screening practices among CF providers were variable and providers are increasingly being confronted with managing CVD risk factors. Partnering with primary care providers is likely to become increasingly important in CF care models.
Plain language summary
- Modulators are medicines that improve the function of the affected protein in cystic fibrosis (CF).
- Cholesterol levels used to be very low in CF, but increasing cholesterol levels in patients on modulators have been reported.
- Other risk factors for heart disease may be changing in CF as patients are living longer.
- We were interested in measuring cholesterol levels over time in people with CF started on ivacaftor, the first modulator therapy.
- We were also interested in how CF providers are monitoring cholesterol levels and risk factors for heart disease.
- We measured blood total cholesterol and other lipid levels at baseline, after being on ivacaftor for 3 months, and at 18 months. We used blood samples from 50 patients that had been collected as part of an earlier clinical trial evaluating ivacaftor.
- We sent out a survey by email through the Cystic Fibrosis Foundation (CFF) to doctors and advanced practice providers (APPs) asking about their screening practices.
- Total cholesterol increased at 3 months on ivacaftor, but then returned towards baseline by 18 months.
- Body mass index (BMI) increased at each visit.
- Low-density lipoprotein (LDL, associated with higher risk of heart disease) did not change.
- CF providers had different screening practices. Only a third of providers had a cholesterol screening policy at their CF centers.
- Several providers had started medicines to treat heart disease risk factors, such as blood pressure and cholesterol-lowering medications, even though most of these providers were lung doctors.
- More studies are needed to understand how cholesterol changes on modulators occur, and to clarify if those changes are short-term or if they are sustained over time.
- It will be important for CF providers to work closely with primary care providers and other specialists going forward.
Introduction
While cardiovascular disease (CVD) has historically been of little concern in people with cystic fibrosis (pwCF), recent reports of ischemic cardiac disease1,2 highlight the need to re-evaluate the risk for CVD in pwCF. Highly effective modulator therapy (HEMT) may increase rates of obesity and hypertension3,4 and longer lifespans may lead to an increased prevalence of CF-related diabetes (CFRD). In addition to these important CVD risk factors, hyperlipidemia is a key CVD predictor in the general population. PwCF have historically been reported to have low total cholesterol (TC), high-density lipoprotein (HDL), and low-density lipoprotein (LDL) levels when compared with age and sex-matched healthy controls.5–8 Elevated blood lipid profiles in pwCF using HEMT have been reported, however, with some noting increases in TC and LDL (with discrepant changes in HDL).9 –13 These reports have largely been retrospective, focused on elexacaftor/tezacaftor/ivacaftor (ETI), and have not evaluated short-term versus longer-term effects. Guidelines have recommended annual lipid screening in patients with CFRD possessing additional CVD risk factors. 14 The adherence rate to this recommendation is unknown, as are lipid screening patterns in the larger group of HEMT-treated pwCF.
We sought to understand providers’ current screening practices for CVD risk factors and to evaluate specific changes in lipid profiles with HEMT. We used stored serum samples from the GOAL Study (“G551D Observational Study”) to evaluate serum lipid concentrations at multiple standardized intervals after starting ivacaftor, including both an early (3 month) and delayed (18 month) time point. GOAL samples were selected as samples from the PROMISE Study (evaluating ETI) were not yet available through the Cystic Fibrosis Foundation (CFF) biorepository. We hypothesized that initiation of ivacaftor, the first HEMT, would significantly increase TC and other lipid values. We also distributed a national survey to assess how CF providers currently screen for dyslipidemia and other CVD risk factors, considering the evolving perceptions of CVD risk in pwCF. We hypothesized that providers would have varying practice patterns regarding lipid screening, given limited guidance and the historically low burden of CVD in CF.
Materials and methods
GOAL lipid analysis
We performed a post-hoc correlative analysis of prospectively collected clinical data and serum samples from the GOAL study (NCT01521338; with cohort 1 enrollment beginning in 2012) 15 and followed the STROBE guideline for cohort studies. 16 Stored serum samples (frozen at −80°C) from the GOAL study were used to evaluate lipid profiles at baseline pre-ivacaftor, and at 3 and 18 months after treatment initiation. 15 Eligibility criteria included those of the GOAL trial (https://clinicaltrials.gov/study/NCT01521338#participation-criteria) with participants who had serum samples available at all three timepoints. We excluded patients with the R117H mutation or other residual function mutations to minimize confounding from milder mutations. Samples from the GOAL study were not routinely collected in the fasting state. Primary endpoints were the changes in TC, HDL, TC/HDL ratio, and directly measured LDL. Lipid testing was performed with the Atellica CH Cholesterol_2 (Chol_2) and CH LDL Cholesterol Direct (DLDL) assays via enzymatic testing with the Atellica CH Analyzer (Siemens). This study was approved by the UNC Institutional Review Board (IRB).
CVD screening survey in CF providers
A survey was designed using Qualtrics© software (The survey for this work was generated using Qualtrics software, Version 12.2022-3.2023 of Qualtrics. Copyright© 2024 Qualtrics. Qualtrics and all other Qualtrics product or service names are registered trademarks or trademarks of Qualtrics, Provo, UT, USA) 17 and piloted by 4 pediatric and adult CF providers at the University of North Carolina at Chapel Hill (UNC) and yielded 65 completed responses. The Checklist for Reporting of Survey Studies (CROSS guideline) was followed when applicable. 18 The cross-sectional survey was distributed by the CFF via email to United States (US) physicians and advanced practice providers (APPs) working in CF care between December 16, 2022 and March 1, 2023 (see Supplement Material). One additional email reminder to complete the survey was sent. Respondents were allowed to leave questions blank. Multiple submissions were not permitted. De-identified survey responses were analyzed in aggregate. This study was approved by the UNC Institutional Review Board (IRB).
Statistical analysis
Based on preliminary data from lipid changes observed at our center, 10 we estimated a sample size of 50 patients would provide > 90% power to detect significant differences in TC and LDL (G*Power 3.1). 19 Unadjusted mean changes in lipid values between visits were calculated and absolute values were analyzed over visits with a repeated measures model. Post-hoc comparisons were corrected by the Tukey method to reduce the risk of false discovery. The significance of prespecified covariates, including body mass index (BMI), age, sex, and CFRD was assessed. Statistical analysis was performed in SAS 9.4 (Cary, NC, USA).
Although a formal power calculation was not performed for the survey study, a total of 65 respondents was our target response goal to have representation from approximately one-half of the ~130 US CFF centers (though multiple respondents from the same CF center could respond). Survey results were tabulated and presented as frequencies and percentages.
Results
GOAL lipid analyses
Serum samples and clinical data from 50 GOAL study participants were analyzed. Baseline demographics are provided in Table 1.
Patient demographics.

Baseline demographics of GOAL participants that provided serum samples (n = 50). CFRD status was determined by diagnosis listed in the US CF Patient Registry during the year of baseline visit; CFTR genotype group was assigned by referencing genotype to CFTR2.org. 20
Categories are not further defined <5% and <8% to protect potentially identifiable individuals.
BMI, body mass index; CFRD, cystic fibrosis-related diabetes; CFTR, cystic fibrosis transmembrane conductance regulator; FEV1pp, forced expiratory volume in 1 second, percent predicted.
Mean lipid values and BMI by visit are shown in Table 2. In a repeated measures model, TC significantly changed across visits (p = 0.004). When evaluating changes between individual visits using the Tukey method to correct for multiple comparisons, a significant increase in TC from baseline to 3 months on ivacaftor was observed (mean difference 9.4 mg/dL, p = 0.003). TC then regressed back toward baseline by 18 months (mean difference between 3 months and 18 months: −5.92 mg/dL, p = 0.087, mean difference between baseline and 18 months: 3.5 mg/dL, p = 0.407). Changes in LDL by visit approached statistical significance, with a similar increase from baseline at 3 months (mean difference 5.2 mg/dL, p = 0.06). No significant changes in HDL or TC/HDL ratio across visits were detected. When age, sex, CFRD, and BMI were simultaneously added to the model as covariates, the significant difference in TC between baseline and 3 months on ivacaftor persisted (mean difference 7.1 mg/dL, p = 0.013). Notably, BMI (analyzed at each visit as a time-varying covariate) was a significant covariate in the model (higher BMI was associated with higher TC levels; p = 0.002), whereas increasing age approached significance (p = 0.052). CFRD was not a significant covariate. BMI significantly increased at each subsequent visit from baseline (p < 0.001).
Mean lipid parameters and BMI in patients with CF at baseline, and at 3 and 18 months on ivacaftor.

Mean lipid parameters and BMI in pwCF at baseline pre-ivacaftor, and at 3 and 18 months on ivacaftor (unadjusted for covariates), n = 50. p Values for the effect of visit in a repeated measures model are shown.
BMI, body mass index; CI, confidence interval; HDL, high-density lipoprotein; LDL, low-density lipoprotein; TC, total cholesterol.
CVD screening survey results
Demographics
Surveys were sent to 1345 email addresses registered on one or more CFF listservs (program directors, physicians, nurse practitioners, and physician assistants). Response rate was 5.6%; 65 completed the entire survey and 10 additional surveys were partially completed. Respondents were from 30 different states, with varying years of experience caring for pwCF (Table 3).
CVD screening by CF providers survey respondent demographics.

CVD screening in CF provider survey respondent demographics.
Write-in responses for other subspecialties included: critical care, hematology, infectious disease, internal medicine primary care, and pediatrics.
APPs, advanced practice providers; CF, cystic fibrosis; CVD, cardiovascular disease; NPs, nurse practitioners; Pas, physician assistants; pwCF, patients with cystic fibrosis.
Screening practices
One-third (22/67) of providers reported having a lipid screening policy at their CF center (16/41 adult providers, 4/18 pediatric providers, and 2/10 providers caring for both). Of those with a policy, seventeen reported a policy of annual lipid screening, one reported screening every other year, two screened during early puberty and near the time of transition to adult care, and two respondents did not report the frequency of screening.
Two-thirds (45/67) reported that their CF center does not have a lipid screening policy. Of these providers, 69% (31/45) screen some pwCF based on certain clinical characteristics, while 22% (10/45) do not check lipids in any pwCF. Reasons for not routinely checking lipids included lack of evidence (29%), competing clinical concerns (37%), and viewing lipid screening as outside the scope of CF providers (29%). Clinical characteristics that most often prompted lipid measurement in pwCF included high BMI (32/65, 49%), family history (30/65, 46%), age (24/65, 37%), CFRD (24/65, 37%), and hypertension (23/65, 35%).
Most respondents routinely ask their patients about exercise habits (62/65, 95%), dietary habits (61/65, 94%), and tobacco use history (56/65, 86%). Assessment of family history of heart disease, hyperlipidemia, hypertension, and stroke was routinely assessed by less than half of CF providers (43%, 37%, 36%, and 29%, respectively).
Management
In the past year, 29% of respondents caring for adults (n = 48) started lipid-lowering therapy in at least one pwCF, 54% prescribed antihypertensive medication, and 48% initiated ischemic cardiac evaluations (Figure 1). Among all respondents, the majority (94%) referred pwCF to a dietician for being overweight/obese, while 34% referred pwCF to a weight loss clinic, and 6% prescribed weight loss medications to pwCF.
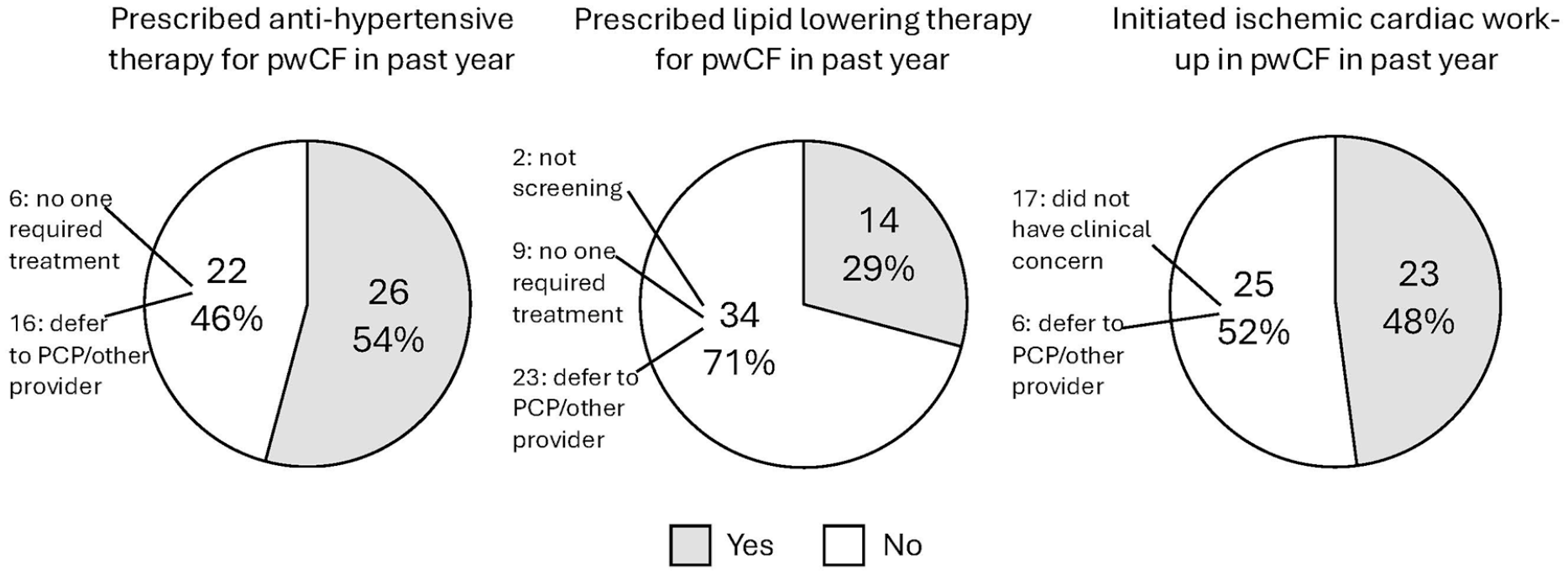
Management of CVD risk factors in patients with CF.
We also assessed providers’ comfort levels in diagnosing and treating CVD risk factors on a 5-point Likert scale, with responses subsequently converted to uncomfortable, neutral, or comfortable (Figure 2). Most adult providers were comfortable diagnosing hypertension and hyperlipidemia but only about one-half were comfortable treating these disorders. In contrast, only a minority of pediatric providers were comfortable diagnosing or treating hyperlipidemia and hypertension. Most providers caring for adult pwCF (94% of adult providers and providers who see both) estimated that ⩽60% of their pwCF see their primary care provider (PCP) annually. Conversely, 71% of pediatric providers estimated that >60% of their pwCF saw their PCP annually.

CF provider comfort level with screening and management of selected CVD risk factors. Provider comfort level with screening and management of selected CVD risk factors. (a) Level of pediatric provider comfort (n = 18, missing data from 1). (b) Level of adult provider comfort (n = 41, missing data from 1).
Free responses. Twenty respondents provided free text responses regarding CF providers’ roles in screening and managing CVD risk factors. Seven respondents noted that because of rising rates of obesity, increasing longevity, and concerns about metabolic complications, screening for CVD risk factors was important when it previously had not been a concern. Increased CFF guidance on lipids and other CVD screening was desired, as well as data on CVD incidence and outcomes on HEMT. Four respondents planned to implement lipid or CVD risk screening in their centers, such as lipid testing with annual labs, or following current American Academy of Pediatrics (AAP) lipid screening recommendations in children. Two respondents felt that CF providers should perform lipid screening; however, more respondents (nine) felt that collaboration with PCPs would provide better care for pwCF, despite the recognition that many pwCF do not have a PCP. Reasons cited included CF providers’ lack of familiarity with updated screening and treatment guidelines and competing clinical demands. Providers also commented on misperceptions by pwCF about the role of the CF provider as their PCP.
Discussion
Interpretation
As reported in recent publications,9 –13 we observed a significant increase from baseline in TC at 3 months after starting HEMT with ivacaftor. By 18 months, however, lipid levels were no longer significantly elevated. We speculate that this could be due to dietary modifications made by patients in response to initial weight gain on ivacaftor, perhaps shifting from the legacy diet of high-fat, high-calorie intake. However, the average BMI in this cohort continued to increase from 3 months to 18 months. Reassuringly, a continued rise in lipids was not observed after the 3-month timepoint, in contrast to other studies of lipid levels in pwCF taking ETI. Because ivacaftor provides less robust restoration of CFTR activity than ETI,21–23 it may also have less effect on lipids (TC mean increases of 15–28 mg/dL reported on ETI),11,12 suggesting a direct relationship between the restoration of CFTR activity and lipid increases. Patients who are eligible for ivacaftor based on genotype may have had less lipid malabsorption compared with other pwCF; however, we think this is less likely as the majority of included pwCF had genotypes predicted to be severe.
Based on our survey of CF providers in the United States, lipid screening practices were highly variable. As expected, most respondents did not have a lipid screening policy at their center. Stated indications for, and frequency of, lipid screening varied. Many CF providers are incorporating risk factors such as age, BMI, and family history into their screening decisions in the absence of center screening policies. In particular, family history may be an important risk factor to assess, as one study found the greater magnitude of TC and LDL increases occured in pwCF who had a family history of CVD or CVD risk factors. 10
In this sample of predominantly pulmonology-trained CF providers, screening for CVD risk factors that overlapped with typical aspects of CF care such as exercise, tobacco use, and dietary habits was high. Screening for a family history of CVD was lower. Respondents were more comfortable diagnosing these conditions, and less comfortable managing these conditions. Concerningly, adult providers estimated that a majority of their pwCF do not see a PCP regularly despite many deferring management of CVD risk factors to other providers. Therefore, CF providers are not uncommonly confronted with initiating therapy for hypertension, hyperlipidemia, and obesity despite a lack of comfort in doing so. This aligns with previous data from our CF Center where preventative screening practices typically performed by a PCP were not routinely completed by the CF care team, again highlighting the need for collaboration between specialists and PCPs. 24
Nearly half of adult provider respondents reported initiating ischemic cardiac evaluations for pwCF in the prior year. While we did not seek details or results of such a workup, it is important to note that several respondents were at least entertaining a diagnosis of coronary artery disease in pwCF despite the historical rarity of CVD in CF.
Limitations
Limitations of our analysis of serum lipids after beginning ivacaftor include the relatively sparse clinical details captured within the GOAL study. The GOAL study was not designed with CVD risk in mind, therefore detailed information about blood pressure, dietary intake, or medication use (either to manage CVD risk factors, or that could predispose to CVD risk factors, such as glucocorticoids or antipsychotic medications) was not available. Similarly, a family history of CVD may predict changes in lipids after HEMT initiation but was not captured. 10 Previously, we observed that the presence of CF liver disease was associated with a blunted change (less of an increase) in TC and LDL after beginning HEMT, and HEMT has been theorized to contribute to lipid changes by an increase in hepatic synthesis of lipoproteins.10,25 Few patients with CF liver disease were included in this sample; however, limiting our ability to assess the impact of this factor. Although blood samples in the GOAL study were not collected in a fasting state, preventing assessment of triglyceride levels, we specifically analyzed directly measured LDL to mitigate non-fasting state effects. There is increasing acceptance of using non-fasting lipid samples for dyslipidemia screening in clinical practice as patients spend more time in the post-prandial state than the fasting state.26,27 Non-fasting lipid values have been used to estimate CVD risk.28,29 Therefore, these non-fasting lipid sample measurements of convenience may still be reflective of real-world clinical data.
Limitations of our survey study include a low response rate (though similar to other CFF-distributed surveys) and the possibility that it may not be representative of wider CF provider practices. Responses may be biased, as CF providers who have encountered CVD risk factors in their patients may be more likely to complete the survey. This US survey may not be generalizable to other countries with different dietary habits or CVD risk profiles. Similarly, results may not be as relevant to providers practicing where HEMT is not available. This survey focused on screening for known CVD risk factors in the general population, but there may be other unassessed CF-specific risk factors such as chronic inflammation or certain infections that may be affecting individual provider screening practices.
Next steps
Understanding risk factors, magnitude, and progression of lipid changes over time with HEMT is important as lifespans of pwCF increase into the decades when CVD is more common and as other traditional CVD risk factors are on the rise. Further studies are required to understand the exact mechanism of changing lipid profiles initially seen with ivacaftor in this study, and over time with ETI in other studies. Two biologically plausible mechanisms include enhanced cholesterol absorption in the gut and changes in the hepatic synthesis of lipids. Longitudinal studies are required to further confirm that the pattern of lipid changes after HEMT is primarily an initial increase, rather than a progressive rise with years of modulator use.
Importantly, there may be other factors specific to CF that influence CVD risk. A recent multinational retrospective cohort study utilizing CF registry and electronic health record databases compared the risk of major adverse cardiac events (MACE) in pwCF using propensity matching with the general population and other inflammatory conditions. While age, hypertension, and diabetes were associated with MACE (which included myocardial infarction, left-sided heart failure, and atrial fibrillation) in pwCF, other clinical factors including lung function and days of intravenous antibiotic use were also associated with a higher risk of MACE. This highlights the need to develop clinical studies evaluating CVD in pwCF rather than simply applying knowledge from the general population to this group of patients. Notably, pwCF had a higher risk of MACE than the general population and an equally high or higher risk of MACE compared with other inflammatory conditions following propensity score-matching. 30
The survey results highlight the need to develop updated recommendations in the areas of lipid and CVD screening in CF through additional data collection and study. The US CF Patient Registry is now capturing lipid results, and providers should continue to report their clinical observations. Clinical care guidelines for patients with CFRD have previously recommended annual lipid screening in those with CFRD who are pancreatic sufficient, or who have additional risk factors (obesity, family history, or immunosuppressive therapy following organ transplant). 31 The 2022 International Society for Pediatric and Adolescent Diabetes (ISPAD) guidelines recommended annual lipid screening in patients with CFRD who are pancreatic sufficient, and lipid screening every 5 years in PwCF with pancreatic insufficiency according to general population recommendations for low-risk individuals. 32 A recent position piece recommended that lipid screening in pwCF should at least occur as frequently as screening in the general population. 33
Even though pediatric pwCF see their PCP more regularly than adult pwCF, CF providers are already collecting annual bloodwork. Therefore, screening in the pediatric CF population according to the AAP and National Heart, Lung and Blood Institute (NHLBI) recommendations (at 9–11 and 17–21 years of age) may be an opportunity to streamline testing.34,35 It is unclear if children with CF should undergo more frequent lipid monitoring than the AAP/NHLBI recommendations, but as HEMT is now available to young infants and is a lifelong medication, lipids and other metabolic parameters may warrant closer monitoring.
The 2024 CFF care model position paper recommends lipid screening for pwCF as per the general population guidelines, 36 however adult lipid screening guidelines usually incorporate CVD risk factors with follow-up testing determined by lipid results and overall risk of CVD, and our understanding of the overall risk of CVD in CF is evolving. 30 While the appropriate screening frequency in adult pwCF is unknown, we recommend improving other CVD risk factor screening, such as assessing family history and blood pressure. Broader work in the healthcare system is needed to ensure adult pwCF have access to PCPs. Until that time, CVD screening burden will continue to fall on CF providers. While they are positioned to identify emerging changes in the CF population, they may not be best suited to manage complications in other organ systems. Partnering with other subspecialists such as endocrinologists, nephrologists, and cardiologists along with PCPs is likely to become increasingly important in CF care models.
Conclusion
Ivacaftor appears to have an early effect on increasing TC after initiation; however, sustained elevations in TC or other lipid parameters were not seen at 18 months. More research is needed to understand the emerging lipid changes described with HEMT, if lifestyle changes such as dietary modification influence these effects, and what the long-term clinical ramifications will be for pwCF. This is especially important to elucidate considering other changing CVD risk factors in the aging CF population. Although there is significant variability in lipid and other CVD screening practices among CF providers, more CF providers are finding themselves in the position of managing CVD risk factors.
Supplemental Material
sj-docx-1-tar-10.1177_17534666251317200 – Supplemental material for New era, new GOALs: cardiovascular screening and lipid management in cystic fibrosis
Supplemental material, sj-docx-1-tar-10.1177_17534666251317200 for New era, new GOALs: cardiovascular screening and lipid management in cystic fibrosis by Katherine A. Despotes, Agathe S. Ceppe, Jennifer L. Goralski and Scott H. Donaldson in Therapeutic Advances in Respiratory Disease
Footnotes
Appendix
Acknowledgements
We would like to acknowledge the Cystic Fibrosis Foundation Biorepository for the provision of samples, the Odum Institute at the University of North Carolina at Chapel Hill for survey revision, and Subhashini Sellers MD and Laura Beth Gifford PA for survey pilot testing and feedback.
Declarations
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.