
Abstract
Background:
Asthma is a leading cause of emergency hospital visits and a significant factor in lost productive hours. The lack of a synthesized body of knowledge on bronchial asthma has notable public health implications.
Objective:
This systematic review and meta-analysis aim to investigate the prevalence of asthma and its predictors among patients presenting in Ethiopian public hospitals.
Design:
Duplicate studies were removed using EndNote version X9. The Newcastle–Ottawa Scale guided the quality assessment, and data extraction followed the Joanna Briggs Institute format.
Data source and methods:
The authors used advanced search methods, including databases such as PubMed, Scopus, Embase, Africa Index Medicus, Science Direct, HINARI, Google Scholar, and manual searches. Data presentation adhered to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) checklist. Publication bias was assessed using Egger’s regression test and a funnel plot. Sensitivity analysis was also conducted.
Results:
The search yielded 352 original articles, with 22 meeting the criteria for inclusion. Using the random-effects DerSimonian-Laird model, the prevalence of bronchial asthma was found to be 9.02% (95% CI: 7.50, 10.53). Several factors were associated with the prevalence of bronchial asthma, including the spring season (AOR 3.7; 95% CI: 2.11, 6.49), childhood age (AOR 4.2; 95% CI: 1.84, 9.55), and urban residence (AOR 1.7; 95% CI: 1.29, 2.31). Other significant factors include family history of asthma (AOR 2.89; 95% CI: 2.22, 3.75), insecticide exposure (AOR 3.3; 95% CI: 2.23, 4.91), and the presence of household insects like cockroaches (AOR 3.33; 95% CI: 2.15, 5.15). Smoking (AOR 3.64; 95% CI: 2.66, 4.98), obstructive sleep apnea (AOR 4.29; 95% CI: 2.37, 7.76), and recurrent upper respiratory tract infections (AOR 4.31; 95% CI: 2.24, 8.32) were also significant.
Conclusion:
The pooled prevalence of bronchial asthma is notably high in Ethiopia. Key predictors include childhood age, spring season, urban living, family history of asthma, exposure to insecticides, presence of cockroaches, smoking, obstructive sleep apnea, and recurrent upper respiratory infections. Targeted interventions are crucial and should focus on lifestyle improvements, allergen identification, cockroach control, smoking cessation, reducing insecticide exposure, and promoting a safe environment.
Trial registration:
This review’s protocol was pre-registered with the International Prospective Register of Systematic Reviews (PROSPERO registration number CRD42023491222).
Introduction
Bronchial asthma involves reversible constriction of the airways due to bronchial spasms, thick mucus production, and significant inflammation of the bronchial smooth muscles. It typically presents with symptoms like coughing, dyspnea, and wheezing. Chest X-rays may also show hyperinflation of the alveoli. 1 According to 2020–2023 World Health Organization (WHO) estimates, nearly 262 million people worldwide suffered from bronchial asthma, resulting in 455,000 deaths.1,2 Additionally, a study conducted in Pakistan showed that 29.1% of cases experienced an acute asthma attack annually during the winter season. 3
Between 1990 and 2019, the incidence of bronchial asthma decreased from 601.20 to 477.92 per 100,000 people, and asthma mortality rates also declined from 8.60 to 5.96 per 100,000. However, it is widely recognized that in 2021 and 2022, asthma prevalence increased in some global regions, marking a shift from the earlier downward trend.1,2 Asthma is the leading cause of emergency hospital visits and significantly contributes to the loss of productive hours. For example, a study in Saudi Arabia revealed that asthma affects over 2 million people. A majority of these individuals experience uncontrolled asthma, which adversely affects their quality of life. The pooled prevalence was reported at 14.3%, showing no significant difference between urban and rural areas. 4 Furthermore, approximately 10% of the population in highly developed European countries grapples with bronchial asthma. Interestingly, the prevalence of asthma showed no discernible difference between the pre- and post-COVID-19 eras.5,6
A systematic review and meta-analysis conducted in 2021 reported a 14.5% prevalence of asthma in Egypt. 7 Similarly, a study in India found an annual pooled prevalence of 3.6%. 8
Various factors are associated with the prevalence and severity of bronchial asthma. For example, a study in India showed that having pets like cats or dogs, household insects such as cockroaches, exposure to fresh fruit smells, and perfumes, and occupations like agricultural work increased asthma prevalence and severity. 8 Likewise, two systematic reviews and meta-analyses in China revealed that comorbidities, smoking, obstructive sleep apnea, cold weather, family history, recurrent upper respiratory tract infections, the spring season, and a history of allergies can predict asthma prevalence.9,10 Despite multiple individual studies on bronchial asthma in Ethiopia, there is a significant lack of consolidated data. This shortfall hinders a comprehensive national understanding of asthma’s prevalence and determinants. The fragmented data creates substantial barriers to understanding the true impact of asthma. It also limits the ability of health policymakers and practitioners to develop targeted, evidence-based strategies to combat the disease effectively. Previous research efforts, often localized or limited in scope, may lead to skewed perceptions of asthma prevalence due to regional differences in healthcare access, environmental factors, and genetic predispositions.5,6,11
The absence of a synthesized body of knowledge is particularly problematic given the public health implications of bronchial asthma. This condition affects significant portions of populations worldwide and is linked to lifestyle, environmental, and genetic factors. In Ethiopia, where healthcare resources are often strained, the lack of detailed, actionable data impedes the effective allocation of resources and implementation of interventions that could yield significant public health benefits.
The importance of conducting this systematic review and meta-analysis is therefore critical. This study aims to fill the gap by aggregating existing research, providing a more robust, accurate, and regionally representative estimate of asthma’s prevalence across different demographics and geographical areas within Ethiopia. It will also help identify key determinants and trends that may influence asthma prevalence, such as urban versus rural discrepancies, socioeconomic status, and exposure to pollutants. This consolidated view will enable a more nuanced understanding of how asthma interacts with other health issues and social determinants in Ethiopia. This is crucial for developing multifaceted intervention strategies that address not only the medical but also the socioeconomic dimensions of managing asthma. The insights gained from this research will be instrumental in guiding healthcare policy, enhancing asthma management programs, and ultimately improving health outcomes by ensuring that interventions are well-targeted and appropriately resourced.
By addressing these research deficiencies, the study will significantly contribute to the body of global asthma research and to the optimization of health interventions in Ethiopia. This approach will not only advance academic understanding but also provide practical benefits in terms of public health strategy and patient care. This underscores the value of this research endeavor.
Research questions
What is the combined prevalence rate of bronchial asthma among individuals seeking medical care in Ethiopia?
What are the collective factors influencing the prevalence of bronchial asthma in Ethiopia?
Methods
Protocol and registration
The results presented in this review adhere to the principles outlined in the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) checklist 12 (Figure 1). The plan for conducting this review was pre-registered with the International Prospective Register of Systematic Reviews (PROSPERO), identifiable by the registration number CRD42023491222.

A flowchart showing the sequence of study selection using PRISMA.
Inclusion and exclusion criteria
All published studies reporting on the prevalence of bronchial asthma in Ethiopia were incorporated into the analysis. The study did not impose any limitations on the period of study; therefore, studies that met the other criteria and were published in any year were included. Citations lacking abstracts or full texts, as well as anonymous reports, editorials, and qualitative studies, were excluded from the analysis.
Search strategy and selection criteria
The authors employed a systematic search strategy across multiple databases from December 12th to 30th, including PubMed, Scopus, HINARI, Science Direct, Africa Index Medicus, Embase, Google Scholar, and manual searches. Our inclusion criteria did not specify publication years, allowing for studies from any time period. However, we excluded studies published in languages other than English. Furthermore, the authors accessed the online library repositories of Addis Ababa University and Bahir Dar University. Additionally, they examined references within each article of the reviewed studies that were relevant to the objectives of this review and meta-analysis. The primary search terms used in PubMed included a combination of MeSH terms: “Asthma,” “Bronchial Spasm,” “Bronchial Hyperactivity,” “Wheeze,” “Predictors,” “Associated Factors,” and “Ethiopia.”
Quality assessment
All studies identified from the database were imported into the citation manager, EndNote version X9, to remove duplicates and facilitate further processing. Five authors (OA, AG, SM, ST, and AE) independently examined and evaluated the titles and abstracts of the identified studies. Any disagreements that arose were resolved through discussion with the fifth author (AE), based on pre-established criteria for article selection. The Newcastle–Ottawa Scale, adapted for the systematic review, was employed by the authors to assess the quality of each study. 13 The assessment considered three key aspects: (1) Selection (with a maximum of four stars), (2) Comparability (with a maximum of three stars), and (3) Outcome (with a maximum of two stars). Each original article underwent individual appraisal by each author. In instances of discrepancies among the authors, consensus was reached by averaging the scores provided by all five authors. The score for each study was calculated on a scale from 0 to 10 for cross-sectional studies and from 0 to 9 for cohort and case-control studies. 14 A score exceeding 6 was deemed “good” and deemed eligible for inclusion in the study. 13 Additionally, publication bias was evaluated using Egger’s regression test, funnel plots, and sensitivity analysis. Noteworthy is the fact that the reliability of these methods across the diverse range of studies under consideration demonstrated commendable consistency, as reflected by Cronbach’s alpha scores ranging from 0.75 to 0.89. Moreover, the thorough validation process conducted by the three experts involved a comprehensive evaluation of each study included in the review.
Outcome measurement
Additionally, publication bias was evaluated using Egger’s regression test, funnel plots, and sensitivity analysis. Noteworthy is the fact that the reliability of these methods across the diverse range of studies under consideration demonstrated commendable consistency, as reflected by Cronbach’s alpha scores ranging from 0.75 to 0.89. Moreover, the thorough validation process conducted by the three experts involved a comprehensive evaluation of each study included in the review.
Data extraction and analysis
The data were acquired using the standardized format from the Joanna Briggs Institute (JBI) data extraction format 2023. 15 Each of the five authors independently gathered relevant information using this format. In cases where discrepancies arose during the data extraction process, the authors resolved them through discussion and consensus. The data extraction format included details such as the primary author’s name, publication year, study setting, design, sample size, sampling technique, prevalence of bronchial asthma with a 95% confidence interval (CI), logarithm of proportion, and associated factors of bronchial asthma prevalence with a 95% CI. Meta-analysis was conducted using the statistical software STATA version 17, utilizing the random-effects DerSimonian-Laird model 16 for pooled analysis. The degree of heterogeneity among studies was gauged using the I-squared statistic, and trim-and-fill analyses were performed to assess publication bias and heterogeneity. Additionally, a sensitivity analysis was performed. Data presentation adhered to the PRISMA checklist 12 (Figure 1).
Results
Search results and characteristics of the reviewed studies
The researchers identified 352 original articles by conducting searches on platforms such as PubMed, Scopus, Embase, Africa Index Medicus, Science Direct, HINARI, and other search engines, including Google Scholar, in addition to manual searches. After removing 244 duplicates, 108 articles remained. Screening of titles and abstracts led to the exclusion of 77 studies due to their irrelevance to the study’s objectives. The remaining 31 studies were assessed for retrieval, but 5 articles could not be retrieved, leaving 26 studies that met the inclusion criteria. Four articles were excluded; two lacked information on study design17,18 and two had outcomes unrelated to this meta-analysis.19,20 In conclusion, this systematic review and meta-analysis included 22 studies21–42 (Figure 1).
Risk bias assessment
According to the Newcastle–Ottawa Scale quality appraisal criteria, the studies included in this systematic review and meta-analysis did not show a risk of bias. As a result, all studies were included for analysis in this review.
The meta-analysis included 22 pertinent studies spanning the years 1977–2022. Within this set, the majority comprising 14 study22,24–27,29-31,33,37,38,39,40,41 employed a cross-sectional design, while six studies employed a case-control design,21,32,34–36,38 and the smallest number (two studies)23,28 utilized a cohort design. The individual sample sizes for each study varied, ranging from 108 to 8,900. This comprehensive review considered a cumulative sample size of 55,807 patients.
Meta-analysis results
The pooled prevalence of bronchial asthma in Ethiopia
In this reviewed study, the prevalence of bronchial asthma, using the random-effects DerSimonian-Laird model, was found to be 9.02% (95% CI: 7.50, 10.53; Figure 2).

A forest plot for the pooled prevalence of bronchial asthma in Ethiopia using the random-effects DerSimonian-Laird model, 2023 (n = 22).
Heterogeneity results
The studies included in this meta-analysis exhibited substantial heterogeneity (I2 = 98.25%, τ 2 = 11.37%) as depicted in Figure 2, and this heterogeneity was statistically significant (p < 0.001) with a 95% CI. The reason behind the high I2 remains unknown. However, it is important to note that an expected increase in heterogeneity is inherent in meta-analyses that examine prevalence across diverse regions and study designs. Therefore, the findings should be interpreted with caution. Furthermore, the study considered a broad prediction interval, a straightforward and easily comprehensible indicator, which highlights significant heterogeneity compared to the confidence interval and implies a high level of variability.
Publication bias and sensitivity test results
Publication bias was evaluated using Begg’s test, which indicated no significant publication bias with a p-value of 0.06. However, Egger’s regression test revealed notable publication bias with a p-value of less than 0.001. The funnel plot (Figure 3) exhibited asymmetry, further supporting the presence of publication bias. To address both publication bias and heterogeneity, trim-and-fill analyses were conducted in the study.

Funnel plot showing the asymmetric distribution of 22 articles on the prevalence of bronchial asthma in Ethiopia, 2024.
A sensitivity analysis was carried out, and all estimates fell within the limits of the confidence intervals, as depicted in (Figure 4). This indicates that no individual study significantly contributed to publication bias. Consequently, none of the studies were excluded from the final meta-analysis.
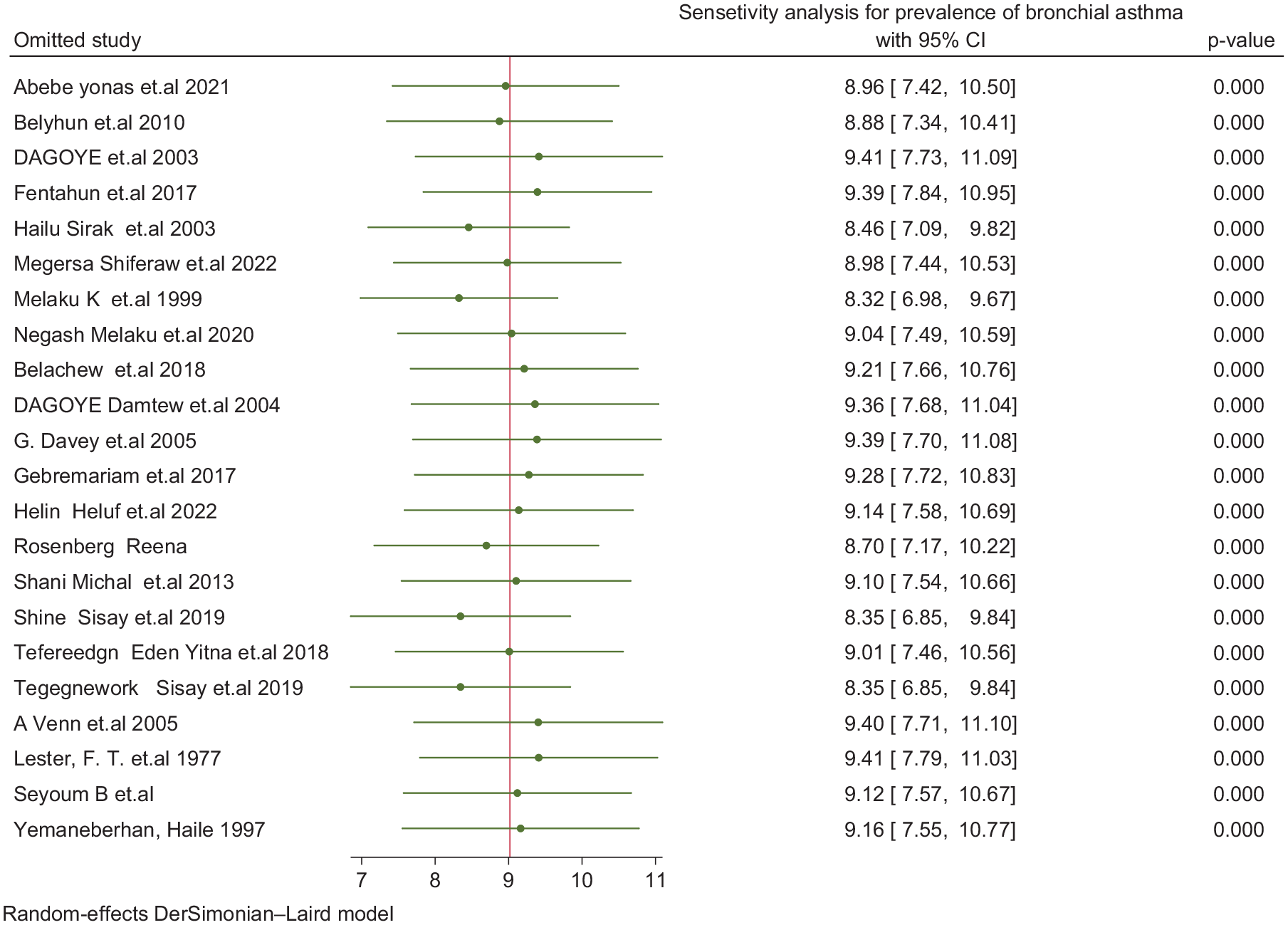
Sensitivity analysis for prevalence of bronchial asthma (n = 22).
Subgroup analysis for bronchial asthma in Ethiopia
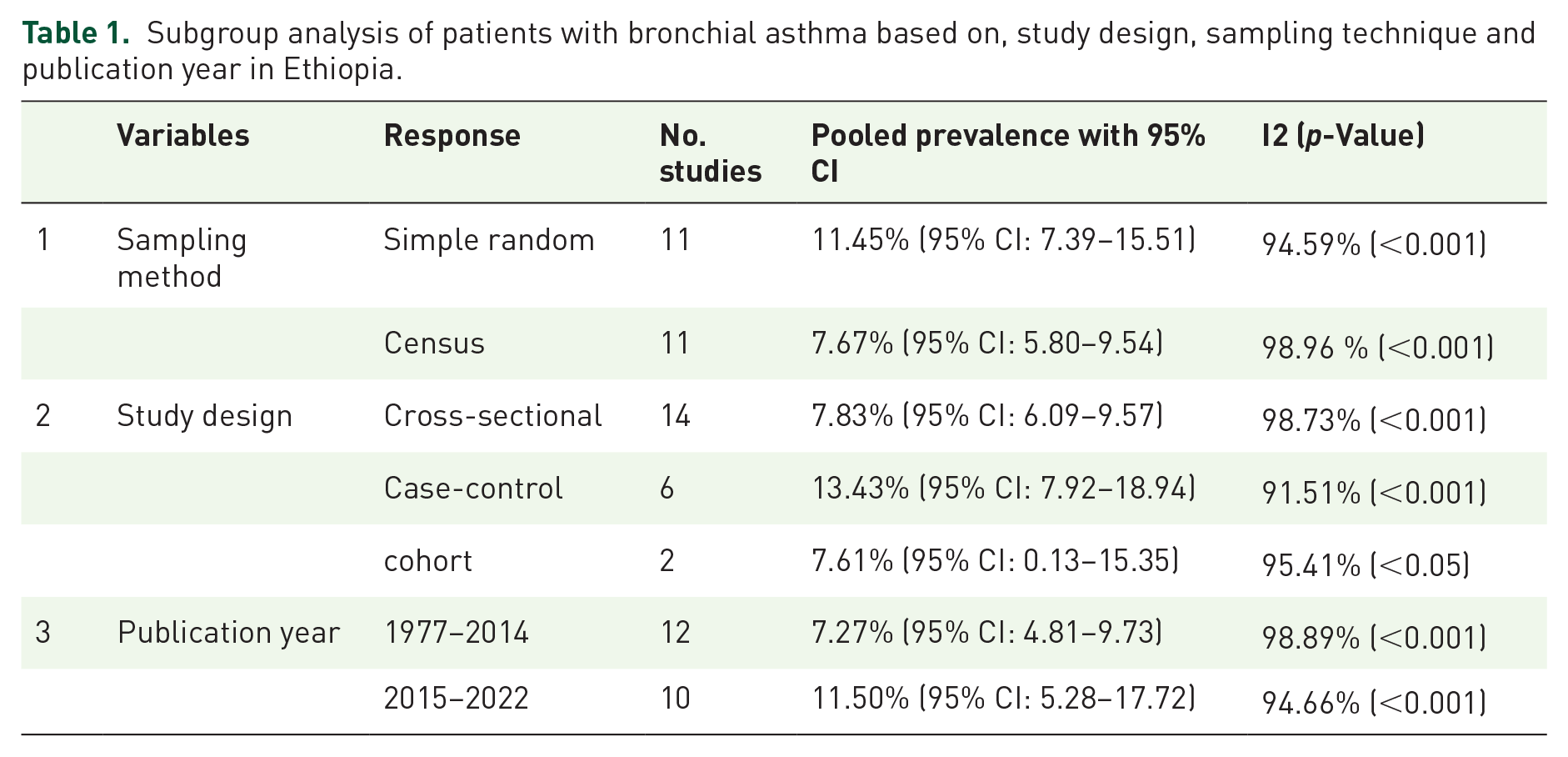
Subgroup analysis based on the sampling technique yielded the following percentages: 11.45% (95% CI: 7.39–15.51) for simple random sampling and 7.67% (95% CI: 5.80–9.54) for census. Regarding study design, cross-sectional studies showed a prevalence of 7.83% (95% CI: 6.09–9.57), case-control studies indicated a prevalence of 13.43% (95% CI: 7.92–18.94), and cohort studies exhibited a prevalence of 7.61% (95% CI: 0.13–15.35). Subgroup analysis by publication year revealed rates of 7.27% (95% CI: 4.81–9.73) for the period 1977–2014 and 11.50% (95% CI: 5.28–17.72) for the years 2015–2022 (Table 1).
Subgroup analysis of patients with bronchial asthma based on, study design, sampling technique and publication year in Ethiopia.
Factors associated with the prevalence of bronchial asthma in Ethiopia
In this comprehensive meta-analysis, nine factors were identified as having a positive impact on the prevalence of bronchial asthma. The combined effect of five studies21,23,29,32,34 revealed that the spring season was associated with 3.7 times higher odds of prevalence (AOR 3.7; 95% CI: 2.11–6.49) compared to the summer season. Similarly, the collective findings of four studies23,25,32,35 indicated that child age had approximately four times higher odds of prevalence (AOR 4.2; 95% CI: 1.84–9.55) than adults. Additionally, the amalgamated results of five studies23,24,27,38 demonstrated that urban residence was associated with 1.7 times higher odds of asthma prevalence (AOR 1.7; 95% CI: 1.29–2.31) compared to rural counterparts. Furthermore, the combined effect of nine studies22–24,27,31,32,38,39,40 showed that a family history of allergic asthma was linked to approximately three times higher odds of prevalence (AOR 2.89; 95% CI: 2.22–3.75) compared to its absence. The combined effect of five studies24,25,27,32,38 indicated that exposure to insecticides increased the odds of prevalence by 3.3 times (AOR 3.3; 95% CI: 2.23–4.91) compared to its absence. The combined effect of five studies24–27,34 also showed that the presence of household insects (cockroaches) was associated with 3.33 times higher odds of prevalence (AOR 3.33; 95% CI: 2.15–5.15) compared to households without cockroaches. The combined effect of six studies26,32–34,38,40 revealed that smoking was associated with 3.6 times higher odds (AOR 3.64; 95% CI: 2.66, 4.98) as predictors of high bronchial asthma prevalence compared to non-smokers. The collective results of four studies22,32–34 indicated that obstructive sleep apnea had four times higher odds (AOR 4.29; 95% CI 2.37, 7.76) as predictors of bronchial asthma compared to patients without obstructive sleep apnea. Furthermore, the combined effect of four studies29,32–34 demonstrated that recurrent upper respiratory tract infection (RURTI) was associated with 4.3 times higher odds (AOR 4.31; 95% CI: 2.24, 8.32) as predictors of bronchial asthma compared to those with no history of RURTI. The combined effect of five studies24–27,34 showed that the being females had 2.5 times higher odds of prevalence (AOR 2.5; 95% CI: 1.21, 4.32) compared to their counterparts (males) (Table 2).
Factors associated with the prevalence of bronchial asthma in Ethiopia, 2024.

AOR, adjusted odds ratio; CI, confident interval; URTI, upper respiratory tract infection.
Discussion
In this reviewed study, the prevalence of bronchial asthma, calculated using the random-effects DerSimonian-Laird model, was found to be 9.02% (95% CI: 7.50–10.53). This suggests that, on average, about nine individuals out of every 100 at the healthcare facility were diagnosed with bronchial asthma. This finding is particularly concerning as it highlights a prevalent cause of morbidity in Ethiopia. Notably, this prevalence rate is higher than the 6.7% reported in a 2020 study conducted in China during the COVID-19 era. 3 The observed difference in prevalence could be attributed to factors such as seasonal variation, lifestyle, weather conditions, and the overall level of socioeconomic development in affluent countries. It is worth mentioning that the prevalence found in this study is lower than the 14.3% reported by a 2018 study in Saudi Arabia, 4 and aligns closely with the 10% prevalence of bronchial asthma among hospitalized patients reported in a global study conducted in 2023. 2
The combined prevalence revealed in this study is notably higher than that reported in studies conducted in Pakistan and India in 2022, where the rates of bronchial asthma were 3.3% 3 and 3.6%, 8 respectively. This disparity may be attributed to several contextual factors. The observed higher prevalence in Ethiopia could be influenced by factors such as a less advanced lifestyle, lower socioeconomic conditions, the presence of household insects, and a higher incidence of recurrent respiratory tract infections. Collectively, these factors contribute to the elevated prevalence of bronchial asthma in the Ethiopian population, distinguishing it from the rates reported in Pakistan and India. 22
In this meta-analysis, factors influencing the prevalence of bronchial asthma in Ethiopia were identified. The spring season emerged as a significant predictor of asthma prevalence, possibly because cold weather mimics allergic reactions, inducing hyperactivity in bronchial smooth muscle and thereby increasing prevalence. This finding aligns with research conducted in Saudi Arabia. 4 Similarly, child age was associated with higher odds of bronchial asthma prevalence. Indeed, most allergic disorders appear during childhood, which are directly related to asthma. Additionally, residing in an urban area was a predictor of asthma prevalence, as most allergens are found in urban environments, which can predispose individuals to asthma. Furthermore, a family history of asthma was associated with higher odds of bronchial asthma prevalence. This finding is consistent with a study conducted in India. 8 This is directly connected to the genetic mutation passed down from the family to the child. 2 The presence of insecticide exposure was associated with higher odds of asthma prevalence. In reality, insecticides can generate free radicals, and these chemicals can predispose individuals to asthma. Similarly, the presence of household insects, such as cockroaches, was a predictor of asthma prevalence. Smoking was also associated with higher odds of bronchial asthma prevalence. In fact, the chemicals in cigarettes can compromise airway function, leading to bronchial spasms. This finding is consistent with global studies conducted in 2005 and 2020.2,42 Additionally, obstructive sleep apnea (OSA) was identified as a predictor of bronchial asthma. Individuals with OSA typically have anatomically narrow airways, leading to manifestations of asthma. Furthermore, RURTI was associated as a predictor of bronchial asthma.
In this study, it was found that females are more susceptible to asthma attacks than males, likely due to the role of estrogen. Estrogen enhances the humoral immune response, increasing IgE production—an antibody integral to allergic reactions and asthma. Elevated IgE levels can lead to inflammation and airway constriction, common in asthma. On the other hand, males have a lower incidence of asthma, possibly due to the anti-inflammatory effects of testosterone. This hormone can dampen immune responses, reducing inflammation and lessening the severity and likelihood of asthma. These hormonal differences may explain the observed gender disparities in asthma prevalence and severity and highlight the importance of considering these factors in asthma treatment strategies. 43 However, before puberty, asthma is more common in males than in females; after puberty, the reverse is true. 11
Implication of the study
This meta-analysis indicates a heightened incidence of bronchial asthma in Ethiopia. Given the identified risk factors, it is imperative that relevant authorities implement preventive actions to reduce both the prevalence and the severe consequences of asthma. Asthma not only disrupts everyday life but can also be life-threatening. Therefore, targeted interventions are essential, such as promoting healthier lifestyles, identifying specific allergens, managing pest infestations (including cockroaches), encouraging smoking cessation, reducing exposure to insecticidal chemicals, and ensuring safer environments.
In summary, this review of bronchial asthma integrates new insights that are critical in enhancing healthcare quality for both managing and preventing asthma. Furthermore, stakeholders, including the Ministry of Health, WHO, and various governmental and non-governmental organizations, are positioned to significantly alleviate the asthma burden through informed management strategies in the broader context of national health.
Limitations of the study
The study did not include non-English research or studies available only in hardcopy due to accessibility issues. It also faces common meta-analysis limitations such as publication bias, which may skew results, and heterogeneity, as variations in study parameters can hinder conclusive results. Moreover, the reliability of the meta-analysis is contingent on the quality of the included studies. Nevertheless, the authors have tried to mitigate these issues by carefully designing the inclusion criteria and performing subgroup analyses.
Conclusion
The combined prevalence of bronchial asthma in Ethiopia is significantly higher compared to high-income nations such as China. Factors such as childhood age, urban living, the spring season, family history of asthma, exposure to insecticides, the presence of household cockroaches, smoking, OSA, and RURTIs are all positively associated with asthma prevalence. The studies included in this review encompass diverse asthma phenotypes, including allergic, mixed, non-allergic, and exercise-induced asthma, with a family history of allergic asthma showing a notable correlation with its prevalence.
Supplemental Material
sj-docx-1-tar-10.1177_17534666241275336 – Supplemental material for The prevalence of asthma and its predictor among patients presetting in Ethiopian public hospitals: systematic review and meta-analysis, 2024
Supplemental material, sj-docx-1-tar-10.1177_17534666241275336 for The prevalence of asthma and its predictor among patients presetting in Ethiopian public hospitals: systematic review and meta-analysis, 2024 by Ousman Adal, Sosina Tamire Mamo, Alamirew Eneyew Belay, Yeshimebet Tamir Tsehay, Henok Biresaw Netsere, Sileshi Mulatu, Gebrehiwot Berie Mekonnen, Mengistu Abebe Messelu, Gebremeskel Kibret Abebe, Wubet Tazeb Wondie, Chernet Tafere and Asnake Gashaw Belayneh in Therapeutic Advances in Respiratory Disease
Supplemental Material
sj-docx-2-tar-10.1177_17534666241275336 – Supplemental material for The prevalence of asthma and its predictor among patients presetting in Ethiopian public hospitals: systematic review and meta-analysis, 2024
Supplemental material, sj-docx-2-tar-10.1177_17534666241275336 for The prevalence of asthma and its predictor among patients presetting in Ethiopian public hospitals: systematic review and meta-analysis, 2024 by Ousman Adal, Sosina Tamire Mamo, Alamirew Eneyew Belay, Yeshimebet Tamir Tsehay, Henok Biresaw Netsere, Sileshi Mulatu, Gebrehiwot Berie Mekonnen, Mengistu Abebe Messelu, Gebremeskel Kibret Abebe, Wubet Tazeb Wondie, Chernet Tafere and Asnake Gashaw Belayneh in Therapeutic Advances in Respiratory Disease
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.