
Abstract
Background:
Lymphangioleiomyomatosis (LAM) is a rare multisystemic disorder characterized by the proliferation of abnormal smooth muscle-like cells. Although serum vascular endothelial growth factor-D (VEGF-D) is currently used as a diagnostic biomarker for LAM, its diagnostic value in Korean patients is unclear.
Objectives:
To evaluate the diagnostic value of serum VEGF-D for LAM in Korean patients.
Design:
A multicenter prospective cohort study
Methods:
Serum samples were prospectively collected from five medical institutions, from patients with LAM (n = 40) and controls (n = 24; healthy participants = 3, other cystic lung diseases = 13, idiopathic pulmonary fibrosis = 4, idiopathic nonspecific interstitial pneumonia = 4). Serum VEGF-D levels were measured using the enzyme-linked immunosorbent assay, and the diagnostic value was evaluated using receiver operating characteristic (ROC) curve analysis.
Results:
The mean age of patients with LAM was 44.5 years, and all were female (controls: 47.8 years; female: 70.8%, p < 0.001). The serum VEGF-D levels were significantly higher in patients with LAM than those in the control group (median: 708.9 pg/mL vs 325.3 pg/mL, p < 0.001). In the ROC curve analysis, serum VEGF-D levels showed good predicting performance for LAM diagnosis (area under the curve = 0.918) with an optimal cut-off value of 432.7 pg/mL (sensitivity = 85.0%, specificity = 87.5%). When 800 pg/mL was used as the cut-off value, the specificity of serum VEGF-D for LAM diagnosis increased to 100.0%.
Conclusion:
Our results suggest that serum VEGF-D may be a useful biomarker for diagnosing LAM in Korean patients, similar to previous reports.
Plain Language Summary
In this study, we discuss a blood test to diagnose a rare lung disease, called lymphangioleiomyomatosis (LAM). LAM primarily affects women, especially during their childbearing years, and can cause serious lung problems such as damage and cyst (air-filled sac) formation. The blood test looks for a special protein in the blood, called vascular endothelial growth factor-D (VEGF-D). If someone has a lot of this protein, it usually means that they have LAM. We have found that when VEGF-D levels are high, the test can effectively separate LAM from other lung diseases. We also found that raising this threshold to higher levels made it much more likely to correctly distinguish a group of people who do not have the disease from patients with LAM. Our study is important because it’s the first to show the usefulness of blood VEGF-D testing in Korean LAM patients, and because it suggests an easier and less inconvenient way for physicians to diagnose LAM in Koreans. Our findings are an important step in improving the management of Korean patients with LAM.
Keywords
Introduction
Lymphangioleiomyomatosis (LAM) is a multisystemic disease caused by the abnormal proliferation of smooth muscle-like cells in the lung vasculature and lymphatic system. 1 LAM occurs exclusively in women, particularly those of childbearing age between 30 and 50 years,2,3 and can occasionally accompany tuberous sclerosis complex (TSC).4,5 Mutations in the TSC genes, particularly in TSC2, can lead to uncontrolled proliferation of atypical smooth muscle-like cells known as “LAM cells”; germline TSC mutations cause tuberous sclerosis complex and somatic mutations have been identified in sporadic LAM.6,7 These cells cause the narrowing of the airways, resulting in airflow limitation and destruction of the lung parenchyma, leading to the formation of thin-walled cysts.1,8 LAM is commonly associated with extra-pulmonary manifestations such as angiomyolipoma (AML) or lymphangioleiomyoma.1,8
The vascular endothelial growth factor (VEGF) family, consisting of VEGF-A, -B, -C, and -D and placental growth factor, is responsible for regulating the development and growth of vascular endothelial cells and thus plays a crucial role in angiogenesis. 9 Among the VEGF family members, VEGF-D is recognized for its potent lymphangiogenic and angiogenic abilities. 10 In the past, diagnosing LAM required a lung biopsy in cases where extra-pulmonary manifestations were absent. However, in a study conducted by Seyama et al. in 2006, it was demonstrated that blood VEGF-D levels in patients with LAM were significantly higher than those in healthy controls, suggesting that measuring serum VEGF-D levels could serve as a non-invasive diagnostic method for LAM. 11 Following these initial findings, several studies have further supported the utility of VEGF-D as a diagnostic biomarker for LAM.12–15 Based on this, the American Thoracic Society (ATS)/Japanese Respiratory Society (JRS) guideline established a definite diagnosis of LAM as a case with a clinical history and typical LAM findings on high-resolution computed tomography scan, along with a characteristic feature such as the presence of AML, TSC, or an elevated serum VEGF-D level equal to or greater than 800 pg/mL. 16 However, the diagnostic value of serum VEGF-D levels for LAM in Asian patients, including Koreans, has not well been established. Therefore, we aimed to determine the diagnostic value of serum VEGF-D in Korean patients with LAM. We also investigated the correlation between serum VEGF-D levels and disease severity, including lung function and exercise capacity, in patients with LAM.
Methods
Study design
This multicenter prospective study was conducted from April 2018 to September 2021 at five medical institutions in South Korea. The study was reported according to the Standards for Reporting of Diagnostic Accuracy Studies (STARD) statement. 17
Study population
This study included 40 patients with LAM diagnosed between July 1994 and January 2021 from five medical institutions in South Korea. Inclusion criteria were as follows: patients confirmed to have definite LAM according to the diagnostic criteria of the ATS/JRS clinical practice guideline 16 and who consented to blood sampling for VEGF-D measurement. Exclusion criteria included patients in whom clinical information could not be obtained at the time of sampling or in whom the sample volume was insufficient for measurement. The control group (n = 24) consisted of healthy participants (n = 3) and patients with other lung diseases (n = 21), including cystic lung disease (n = 13; emphysema or cyst = 9, Birt–Hogg–Dubé syndrome = 3, Sjogren’s syndrome = 1), idiopathic pulmonary fibrosis (n = 4), and idiopathic nonspecific interstitial pneumonia (n = 4). All methods were carried out in accordance with relevant guidelines and regulations.
Clinical data
Clinical parameters and survival data were collected from the electronic medical records of patients with LAM, and the control group. All clinical parameters were obtained at the time of blood sampling. Spirometry, diffusing capacity for carbon monoxide (DLCO), and total lung capacity (TLC) measured by plethysmography were conducted following the ATS/European Respiratory Society recommendation.18–20 The 6-minute walk test (6MWT) was performed according to the ATS guidelines. 21 Data on the presence of TSC and LAM complications, such as pneumothorax, lymphangioleiomyoma, and AML, were also collected at the time of blood sampling. Medical therapy for LAM included the administration of sirolimus and the use of inhaled bronchodilators.
Measurement of VEGF-D
Serum samples were collected prospectively from April 2018 to September 2021 at each medical institute and stored at −80°C until measurement (April 2022). Serum VEGF-D levels were quantified using an ELISA kit (R&D Systems Inc., Minneapolis, MN, USA) following the manufacturer’s instructions. All samples were tested in duplicate, and the average values were used for the subsequent analyses. The inter-assay coefficient of variation (standard deviation/mean × 100) for duplicate samples was determined to be 7.3%.
Statistical analysis
All variables are represented as mean ± standard deviation, median (interquartile range [IQR]), or number (%). Continuous variables were compared between groups using the Mann–Whitney U test, and categorical variables were compared using Fisher’s exact test. Receiver operating characteristic (ROC) curve analysis was conducted to evaluate the diagnostic performance of serum VEGF-D levels, with the area under the curve (AUC) being reported. The optimal cut-off value was determined as the value corresponding to the highest Youden’s index. 22 Additional parameters, including sensitivity, specificity, positive predictive value (PPV), negative predictive value (NPV), and accuracy, were determined through ROC curve analysis. The diagnostic performance of serum VEGF-D for LAM was also evaluated using the cut-off value of 800 pg/mL, as recommended in the ATS/JRS guideline. 16 The correlation between serum VEGF-D levels and clinical parameters was evaluated using the Spearman rank-order correlation coefficient. All statistical analysis was performed using SPSS 24.0 (IBM Corp., Armonk, NY, USA). Statistical significance was set at p < 0.05 (two-tailed).
Results
Baseline characteristics
Among all patients with LAM, the mean age was 44.2 ± 9.6 years, all were female, and 8.1% were ever-smokers (Table 1). The LAM group had a significantly higher proportion of females than the control group (100.0% vs 70.8%, p = 0.001) (Supplemental Table S1). The median follow-up period from LAM diagnosis to the sampling date was 0.7 years (IQR: 0.1–8.8 years). In sirolimus-treated patients, median interval between sirolimus treatment and blood sampling was 3.2 years (IQR: 1.3–6.4 years)). Of the 40 patients, 22 (55.0%) were diagnosed by biopsy (lung = 20, lymph node = 2), while the remaining 18 were diagnosed based on typical chest CT findings with complications, including 11 (27.5%) with lymphangioleiomyoma, 9 (22.5%) with TSC, and 8 (20.0%) with AML. The most common accompanying complication was lymphangioleiomyoma (60%), followed by pneumothorax (15%), and AML (5.0%; Table 1). TSC was present in 25.0% of patients.
Baseline characteristics of patients with LAM.

Data are represented as the mean ± standard deviation, or number (%).
Median levels of serum VEGF-D were significantly higher in the LAM group (708.9 (IQR: 503.7–1453.1) pg/mL vs 325.3 (287.7–384.9) pg/mL, p < 0.001) than those observed in the control group (Figure 1(a) and Supplemental Table S1).
DLCO, diffusing capacity for carbon monoxide; FEV1, forced expiratory volume per 1 second; FVC, forced vital capacity; LAM, lymphangioleiomyomatosis; 6MWT, 6-minute walk test; RV, residual volume; SpO2, saturation of oxygen; TSC, tuberous sclerosis complex; TLC, total lung capacity.

Comparison of serum VEGF-D levels between patients with LAM and controls. (a) Comparisons of serum VEGF-D levels between the LAM and control groups. The box and whisker plot shows all points in the data distribution. (b) Receiver operator characteristic curve for VEGF-D in diagnosing LAM. The dashed line is the reference.
Sirolimus and inhaled bronchodilators were used in 57.5% and 37.5% of all patients, respectively. Progesterone was used in 15.0% of patients, but none received a gonadotropin-releasing hormone agonist or underwent oophorectomy. In addition, none of the patients received home oxygen therapy. Patients receiving sirolimus had lower lung function (DLCO, forced expiratory volume per 1 second) than those not receiving sirolimus (Supplemental Table S2).
Diagnostic performance for LAM
In the ROC curve analysis, serum VEGF-D showed high diagnostic performance for LAM, with an AUC value of 0.918 (95% confidence interval (CI): 0.848–0.988, p < 0.001; Figure 1(b)). The optimal cut-off value for serum VEGF-D was determined to be 432.7 pg/mL. The sensitivity and specificity for LAM diagnosis were 85.0% and 87.5%, respectively, resulting in a PPV of 91.9%, an NPV of 77.8%, and an overall accuracy of 86.0% (Table 2). In addition, using a cut-off value of 800 pg/mL for LAM diagnosis increased the specificity of serum VEGF-D to 100%; however, this was at the cost of reduced sensitivity (42.5%) and accuracy (64.1%).
Comparison of diagnostic performance of VEGF-D according to cut-off values in patients with LAM.

Optimal cut-off value estimated by ROC curve analysis.
LAM, lymphangioleiomyomatosis; NPV, negative predictive value; PPV, positive predictive value; VEGF, vascular endothelial growth factor.
VEGF-D levels according to complications
No significant differences were observed in serum VEGF-D levels with respect to the presence of complications at the sampling time (Figure 2); however, patients with AML (n = 2) showed numerically lower median VEGF-D levels (436.2 (IQR: 371.6–500.8) pg/mL vs 738.4 (518.5–1502.0) pg/mL, p = 0.092) than those without (n = 38; Figure 2(c)). In addition, no differences in median VEGF-D levels were observed between patients receiving sirolimus and those not receiving sirolimus (698.7 (IQR: 554.8–1341.4) pg/mL vs 719.0 (IQR: 499.9–1408.26) pg/mL, p = 0.705).
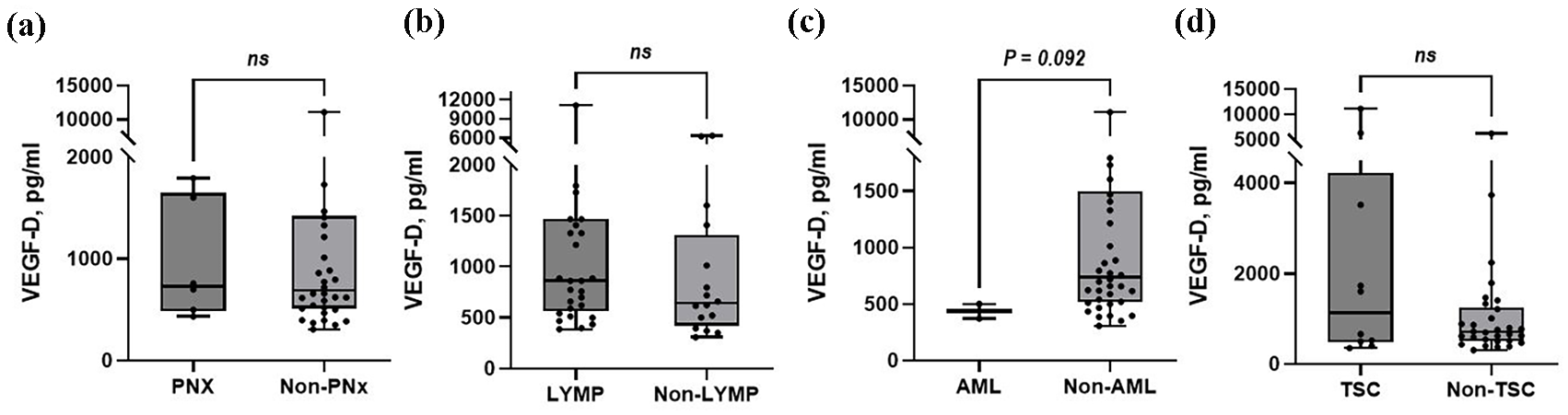
Comparison of serum VEGF-D levels in relation to complications in patients with LAM. (a) Pneumothorax, (b) Lymphangioleiomyoma, (c) Angiomyolipoma, (d) Tuberous sclerosis. The box and whisker plot shows the full range of the data distribution. We assessed the presence of complications at the sampling time.
Correlation with clinical parameters
No significant associations were observed between serum VEGF-D levels and clinical parameters; however, serum VEGF-D showed a trend toward a weak correlation with DLCO (r = −0.292, p = 0.072), and resting (r = −0.397, p = 0.083) and lowest SpO2 during the 6MWT (r = −0.394, p = 0.086; Figure 3 and Supplemental Table S3).

Correlation between serum VEGF-D levels and clinical parameters. (a) DLCO (b) Resting SpO2 during the 6MWT (c) Lowest SpO2 during the 6MWT. The plot displays slopes (lines) obtained through simple linear regression, along with their 95% confidence intervals (dash lines), using all data points.
Discussion
Herein, we evaluated the diagnostic value of serum VEGF-D levels for LAM in Korean patients for the first time. Our results suggest that serum VEGF-D can be a valuable diagnostic biomarker for LAM. Our findings also suggest that the internationally suggested cut-off value of 800 pg/mL is appropriate to optimize the specificity of LAM diagnosis in the Korean population.
Our study findings are consistent with previous research, supporting the diagnostic efficacy of VEGF-D for LAM in the Korean population (Table 3).12–15,23–25 In a US study by Young et al., serum VEGF-D levels were significantly higher in patients with LAM (n = 56) than in healthy controls (n = 40) (median: 1175 pg/mL vs 309 pg/mL, p < 0.001). Using a cut-off value of 600 pg/mL, the AUC of VEGF-D was 0.961, with a sensitivity of 74% and a specificity of 98%. 12 Further increasing the cut-off value to 800 pg/mL improved the specificity to 100%. 12 Similarly, a UK study showed that serum VEGF-D levels were higher in patients with LAM (n = 58) than in healthy female controls (n = 32) (median: 1174 pg/mL vs 332 pg/mL, p < 0.001). The AUC was 0.967, and the optimal cut-off value was 440 pg/mL (sensitivity: 93%, specificity: 97%). 23 In a recent meta-analysis including 10 studies, the overall AUC of VEGF-D for diagnosing LAM was 0.980, with a sensitivity of 82% and a specificity of 98%. 26 Our study yielded comparable results to previous studies with a ROC curve analysis estimating an optimal cut-off of 432.7 pg/mL, a sensitivity of 85.0%, and a specificity of 87.5% (Table 3). Further, applying a cut-off of 800 pg/mL resulted in no controls being misclassified as having LAM, suggesting that this cut-off value may be suitable in Korean patients. These consistent findings across different studies highlight the robustness of serum VEGF-D as a diagnostic biomarker for LAM and its potential clinical utility in different populations, including Korean patients.
Comparison of the diagnostic performance of serum VEGF-D levels in patients with LAM.
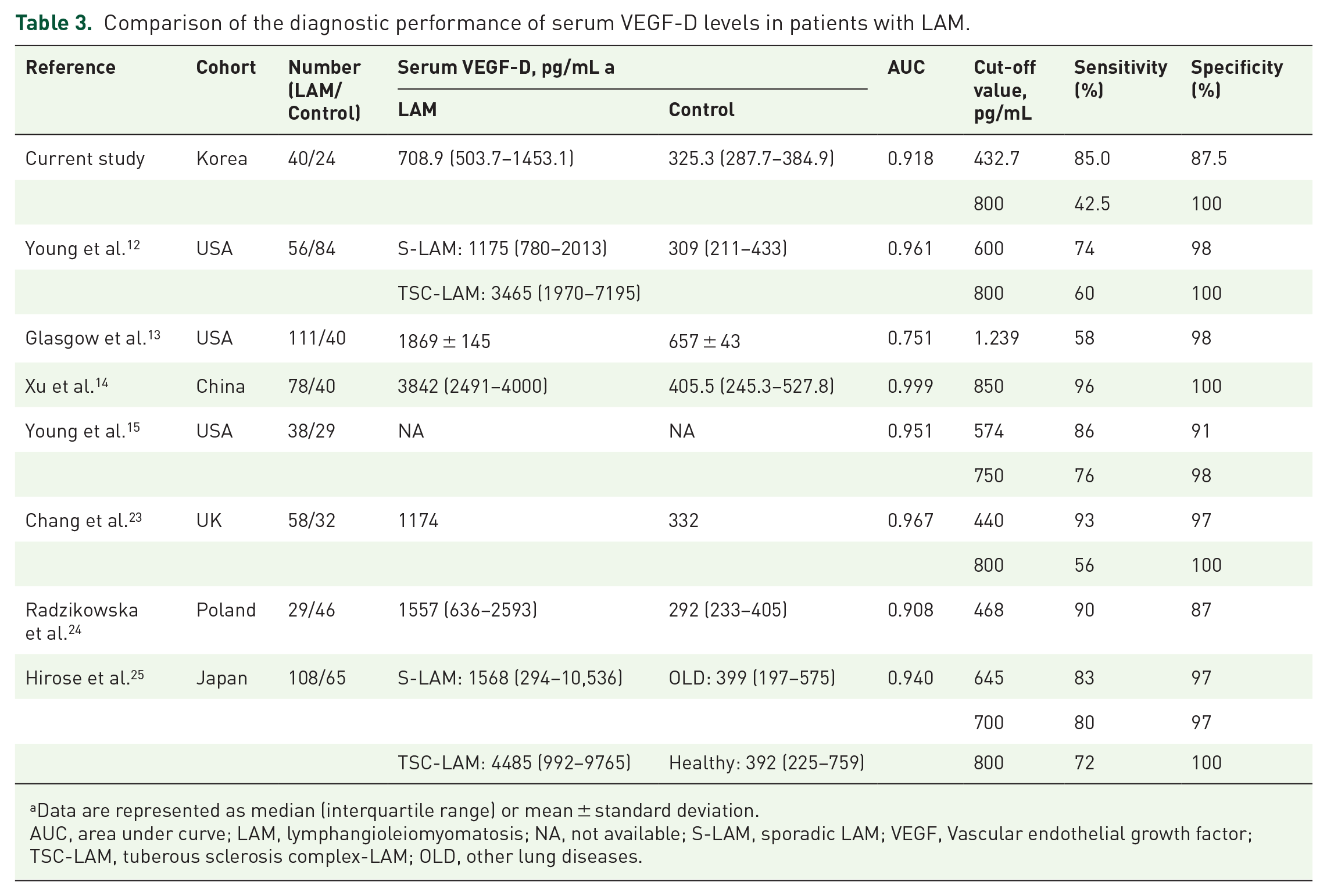
Data are represented as median (interquartile range) or mean ± standard deviation.
AUC, area under curve; LAM, lymphangioleiomyomatosis; NA, not available; S-LAM, sporadic LAM; VEGF, Vascular endothelial growth factor; TSC-LAM, tuberous sclerosis complex-LAM; OLD, other lung diseases.
Our results suggested a marginal association between serum VEGF-D levels and disease severity in patients with LAM. This finding aligns with previous studies, such as the MILES trial (n = 87), which demonstrated significantly higher baseline VEGF-D levels in LAM patients requiring oxygen supply than those who did not (median: 1.7 ng/mL (oxygen) vs 0.84 ng/mL (no-oxygen), p < 0.001). 27 The MILES trial also reported a significant association between baseline VEGF-D levels and lung function parameters, including DLCO (β = −2.38, p < 0.001), FVC (β = 0.21, p = 0.006), and TLC (β = 0.54, p < 0.001). 27 In addition, another study conducted in a Brazilian LAM cohort (n = 104) also showed a weak negative correlation between serum VEGF-D level and DLCO (r = −0.26, p = 0.001). 28 Other studies have similarly found a significant correlation between VEGF-D levels and DLCO in patients with LAM.13,25 However, only a marginal correlation between baseline VEGF-D and DLCO or resting/lowest SpO2 during the 6MWT was observed in our study. The smaller size of our cohort and the higher proportion of patients receiving sirolimus (56.5%) than that in previous studies (0%–52%)13,25,27 could have influenced these findings.
Taveira-DaSilva et al. observed a significant reduction in VEGF-D levels from 3720 pg/mL to 945 pg/mL (p < 0.001) after administration of sirolimus to 25 patients with LAM. 29 However, in our study, no differences in serum VEGF-D levels were observed between patients receiving sirolimus and those not receiving sirolimus. This may be due to the difference in severity between the two groups; patients not receiving sirolimus had higher lung function than those treated with sirolimus, suggesting that untreated patients may have milder disease severity than treated patients. This difference in severity may have contributed to the finding that the untreated patients had similarly low VEGF-D levels as the treated group. Therefore, larger studies with longer follow-up periods are needed to clarify the impact of sirolimus on VEGF-D levels and its relationship with lung function in LAM.
Our study has some limitations. First, the number of patients included was small due to the rarity of the disease, which might have limited the statistical power of the study. However, the inclusion of patients from multiple centers enhances the generalizability of the findings. Additionally, the baseline characteristics of the patients in this study were comparable to those reported in other studies,12–15,24,25 thus increasing the reliability of our results. Second, grouping various lung diseases in patients and healthy participants (controls) could have introduced confounding factors affecting serum VEGF-D levels. However, previous studies have consistently shown that VEGF-D levels are elevated explicitly in LAM and not in other lung diseases, minimizing the impact of this limitation.15,25 Third, due to the rarity of LAM, this observational study did not consider a predefined sample size calculation. Lastly, more than half of the patients in our study were receiving sirolimus. Since sirolimus administration can affect VEGF-D levels, 30 it may have influenced the results of the correlation between VEGF-D and disease severity. Future studies should consider recruiting patients before sirolimus administration to address this limitation. Despite these limitations, to our knowledge, our study is the first to demonstrate the diagnostic value of serum VEGF-D in Korean patients with LAM from a multicenter perspective cohort.
Conclusion
Our results suggest that serum VEGF-D can be a valuable biomarker for diagnosing LAM in Korean patients. As stated in the international guideline, the recommended cut-off level of serum VEGF-D (⩾ 800 pg/mL) for LAM diagnosis may be appropriate for the Korean population. Further large-scale prospective studies are necessary to confirm our findings.
Supplemental Material
sj-docx-1-tar-10.1177_17534666241272928 – Supplemental material for Diagnostic value of serum vascular endothelial growth factor-D in Korean patients with lymphangioleiomyomatosis
Supplemental material, sj-docx-1-tar-10.1177_17534666241272928 for Diagnostic value of serum vascular endothelial growth factor-D in Korean patients with lymphangioleiomyomatosis by Hee-Young Yoon, Su-jin Moon, Song Yee Kim, Jong Sun Park, Sun Mi Choi, Hyung Koo Kang and Jin Woo Song in Therapeutic Advances in Respiratory Disease
Supplemental Material
sj-docx-2-tar-10.1177_17534666241272928 – Supplemental material for Diagnostic value of serum vascular endothelial growth factor-D in Korean patients with lymphangioleiomyomatosis
Supplemental material, sj-docx-2-tar-10.1177_17534666241272928 for Diagnostic value of serum vascular endothelial growth factor-D in Korean patients with lymphangioleiomyomatosis by Hee-Young Yoon, Su-jin Moon, Song Yee Kim, Jong Sun Park, Sun Mi Choi, Hyung Koo Kang and Jin Woo Song in Therapeutic Advances in Respiratory Disease
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.