
Abstract
Objective:
The data in regard of the clinical characteristics and diagnosis of somatic cough syndrome in adults were limited. The aim of this study was to fill that gap.
Methods:
This was a retrospective analysis of patients with somatic cough syndrome. We described clinical characteristics of adult patients with somatic cough syndrome.
Results:
Twenty-three somatic cough syndrome patients were identified in 543 adult patients with chronic cough. Psychiatric disorder of these patients was identified as anxiety (n = 8), obsessive-compulsive (n = 7), somatoform (n = 6), depression (n = 3), and cognitive bias (n = 1). Twelve patients showed abnormal results of investigations related with common causes of chronic cough, including gastroesophageal reflux, sputum eosinophilia, bronchial hyper-responsiveness, or signs of sinusitis but did not respond to the treatments directed to those conditions. All these patients were ever misdiagnosed as other causes of chronic cough. Compared to 520 non-somatic cough syndrome patients, patients with somatic cough syndrome were younger (32 (29.0–43.0) vs 42.0 (32.0–55.0) years, p = 0.013), longer disease duration (48.0 (19.5–102.0) vs 24.0 (9.0–72.0) months, p = 0.037), more common in dry cough (100% vs 57.6%, p < 0.001), and lower proportion of nocturnal cough (13.0% vs 40.2%, p = 0.009). Common cold (60.9%) was the most common initial trigger of cough and itchy throat (60.9%) was the most common accompanying symptom in patients with somatic cough syndrome. Notably, there were similar distribution in cough triggers and accompanying symptoms between two groups.
Conclusion:
In spite of much higher proportion of dry cough and smaller proportion of nocturnal cough, adult patients with somatic cough syndrome show similar clinical characteristics with other chronic cough patients, in regard of cough triggers, accompanying symptoms as well as abnormal results of investigations, which should be an important reason for misdiagnosis of somatic cough syndrome. Psychiatric disorder should be addressed in clinical management of chronic cough.
Background
Chronic cough is one of common complains for patients who seek medical attention in both of respiratory specialist clinic and community clinic, and the estimated global prevalence is 9.6% (range: 2.3–18.1%). 1 Many conditions present chronic cough as sole symptom, including cough variant asthma, eosinophilic bronchitis, upper-airway cough syndrome, gastroesophageal reflux cough,2,3 as well as some rare causes like protracted bacterial bronchitis, obstructive sleep apnea syndrome, and vocal cord disfunction. 4 Sometime no pathological causes of cough could be identified even after full investigations or cough still persist after treatment directed to the potential conditions. Those patients are defined as refractory chronic cough or unexplained chronic cough. In spite of pathological causes, chronic cough could be related to functional and psychologic conditions, including somatic cough syndrome (previously referred to as psychogenic cough), habitual cough, and tic cough.5,6 Since somatic cough syndrome often fails to improve with therapies neglecting target the potential causes of psychological factors, these patients may be misdiagnosed as chronic refractory cough or unexplained chronic cough, leading to repeated investigations and inappropriate medications. It is therefore important to consider this particular condition in clinical practice.
Previous studies on somatic cough syndrome have been mainly conducted on children or adolescents. One study ever showed that somatic cough syndrome was one of common cause of chronic cough in children. 7 On contrast, only a few adult cases with somatic cough syndrome has been reported8–10 Clinical features, diagnosis, and therapy of somatic cough syndrome in adult patients is poorly understood. In this study, we retrospectively analyzed the clinical characteristics of adult patients with psychogenic versus non-somatic cough syndrome recruited from our cough clinic aiming to enhancing the recognition of somatic cough syndrome in adults.
Method
Subjects and diagnosis
This was a retrospective study. Data were extracted from the medical records of consecutive chronic cough patients from 2012 to 2017 who underwent full examinations and treatment who received outpatient care at cough specialist clinic of the First Affiliated Hospital of Guangzhou Medical University. As described previously, 11 the medical record included demographics, clinical features, laboratory results, primary diagnosis, response to therapy, follow-up, and final diagnosis of chronic cough patients. This retrospective study was approved by the Ethics Committee of the First Affiliated Hospital of Guangzhou Medical University (approval no. 201778).
In this study, chronic cough was defined as a cough lasting more than 8 weeks, presenting with sole or predominate symptom without obvious abnormal X-ray chest or evidence of obvious lung diseases. The standard diagnostic workflow was used to identify the causes of chronic cough as described previously. 11 Briefly, detailed medical history were recorded first, including initial triggers, cough duration, nature of cough, cough severity scores, and accompanying symptoms. Then chest radiography/computerized tomography, spirometry, bronchial provocation test, and differential cell in induced sputum were performed in all enrolled patients, and 24 h esophageal pH value monitoring, sinus computed tomography (CT), bronchoscopy, or other investigations were selected in some patients. The primary diagnosis was made based on medical history and investigations, and the etiological treatment was initiated. The cause of cough was determined if cough resolved after the etiology-specific treatment. The diagnostic criteria of somatic cough syndrome in this study were as follows:
There was no any response to the treatment directed to potential conditions related with common causes or other uncommon causes of chronic cough.
Excessive thoughts, feelings, or behaviors related to cough, manifested by at least one of the following:
a. Disproportionate and persistent thoughts about the seriousness of cough. b. Persistently high level of anxiety or depression about cough or health. c. Excessive time and energy devoted to cough or health concerns. d. Voluntary cough due to disorders of sensation related with dyspnea, tight chest, or other senestopathia. e. Persistent cough associated with secondary gain.
Excessive stress in learning, job, business, family, or poor relationship with family member or colleagues.
Obvious improvement in cough after pharmacologic interventions (anxiolytics, antidepressants, etc.) or non-pharmacologic interventions (hypnosis, suggestion therapy, etc.) or combinations of both.
The assessment of cough severity included the cough visual analogue scale (VAS) and Cough Symptom Score (CSS). VAS was a 10-cm scale on which patients indicate the severity of cough, and higher score mean more severe cough. CSS is a two-part questionnaire relating to cough symptoms, in which each part score ranges from 0 to 5. ‘0’ means no cough; ‘5’ indicates that distressing coughs most of the day, or distressing coughs preventing any sleep. 12
Statistical analysis
Statistical analysis was performed using SPSS version 19.0 (IBM Corporation). The incidence of clinical characteristics and accompanying symptoms were expressed as percentages. Inter-group differences were analyzed by independent samples t-test or χ2 test as appropriate. Non-normal distribution or heterogeneity of variances was calculated using Mann–Whitney U-test. Two-sided p value < 0.05 was considered statistically significant.
Results
Cause of somatic cough syndrome
Twenty-three somatic cough syndrome was identified in 543 patients with chronic cough. Psychiatric disorder of these 23 patients were identified as anxiety (n = 8), obsessive-compulsive (n = 7), somatoform (n = 6), depression (n = 3), and cognitive bias (n = 1) (Table 1). These patients showed an underlying psychological factor including job/economic pressure, excessive attention to their illness, poor family relationships, love failures, and stress from study. The family relationship was the most common issue among female patients (77.8%), while job/economic pressure was the predominant factor among males.
Features of somatic cough syndrome.

VAS, cough visual analogue scale.
All patients with somatic cough syndrome underwent psychotherapy and/or psychotropic drug treatment, including sertraline hydrochloride, escitalopram, sulpiride, flupentixol-melitracen, paroxetine hydrochloride, olanzapine, and alprazolam. Cough improved within 2–4 weeks in most patients with psychological counseling and drug treatment. These patients achieved completed resolution of cough gradually, usually with several months. Cough did not relapse during 1 year following up.
Clinical characteristics
The patients with somatic cough syndrome were younger (32 (29.0–43.0) years vs 42.0 (32.0–55.0) years, p = 0.013) than those with non-somatic cough syndrome that consisted of 520 chronic cough subjects whose causes were asthma (n = 80), eosinophilic bronchitis (n = 72), gastroesophageal reflux (n = 64), chronic bronchitis (n = 44), upper-airway cough symptom (n = 42), atopic cough (n = 33), unexplained cough/refractory chronic cough (n = 93), and other causes. In addition, compared to non-somatic cough syndrome, the duration of cough was longer in somatic cough syndrome patients (48.0 (19.5–102.0) months vs 24.0 (9.0–72.0) months, p = 0.037). All somatic cough syndrome patients presented dry cough, which was significantly higher than non-psychogenic group (100% vs 57.6%, p < 0.001). However, the incidence of nocturnal cough was significantly lower (13.0% vs 40.2%, p = 0.009) in somatic cough syndrome. As for subjective cough severity, the VAS and CSS-daytime score in patients with somatic cough syndrome were significantly higher than that in non-psychogenic group (Table 2).
Clinical feature across different causes of chronic cough.
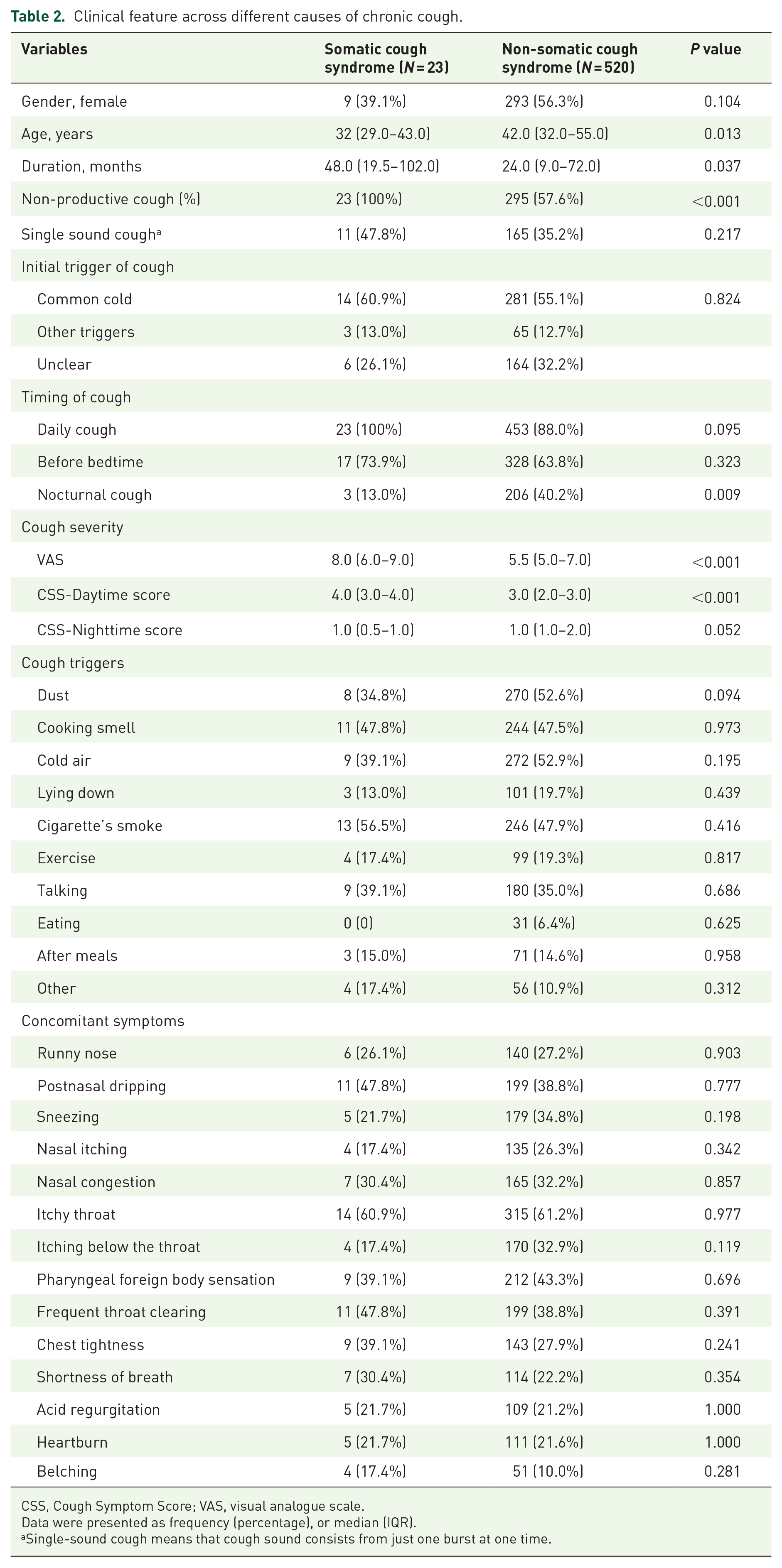
CSS, Cough Symptom Score; VAS, visual analogue scale.
Data were presented as frequency (percentage), or median (IQR).
Single-sound cough means that cough sound consists from just one burst at one time.
Common cold (60.9%) was the most common initial trigger of cough in patients with somatic cough syndrome. The most common accompanying symptom was itchy throat (60.9 %) in patients with somatic cough syndrome, following by frequent throat clearing (47.8%), postnasal dripping (47.8%), pharyngeal foreign body sensation (39.1%), chest tightness (39.1%), and shortness of breath (30.4%). Notably, there were similar distribution in cough triggers and accompanying symptoms between two groups (p > 0.05 for all; Table 2).
Laboratory investigations and misdiagnosis
The 12 patients (52.2%) with somatic cough syndrome had abnormalities in laboratory investigations related with cough, including pathological reflux showed by 24 h esophageal pH monitoring (n = 4), eosinophilia in induced sputum (n = 4), bronchial hyper-responsiveness (n = 2), and sinus CT (n = 2). However, the cough did not improve after the treatments directed to these potential causes. Among 23 patients with somatic cough syndrome, four patients were ever diagnosed as gastroesophageal reflux previously, seven as chronic bronchitis, six as chronic pharyngitis, four as cough variant asthma, and two as upper-airway cough syndrome.
Discussion
In this study, we analyzed clinical features of somatic cough syndrome in adult patients and found they were more often younger with depression, anxiety, or other psychological disorders, and the most frequent initial trigger is common cold. Being similar to non-psychological patients, several concomitant symptoms and abnormal including results were found in many somatic cough syndrome patients.
There was no significant difference in sex between the study groups, which is consistent with previous report with almost equal proportion of males and females in pediatric and adult patients with somatic cough syndrome. 9 The common psychological factors underlying somatic cough syndrome in children and adolescents are attention seeking, school phobia, and unpleasant interpersonal relationships on campus. Bhatia et al. 9 reported an underlying psychological factor in 62.5% of adult and pediatric patients with somatic cough syndrome, including dissatisfaction in family, social distress, stress due to heavy work, and quarrel with spouse. In this study, all the patients had a psychological factor for cough. Poor family relationships were the main cause for female patients, whereas job/economic stress was more common in male patients, which is consistent with conventional gender roles.
Our study showed that common cold was the initial trigger of psychogenic cough in most adult patients, which is consistent with a previous study in children with psychogenic cough who usually preceded by an upper respiratory tract infection.8,13,14 Another study showed that 36% children developed cough related with an obvious psychosocial stressor (e.g. new school and exams) after a viral cold. 15 The correlation between preceding upper respiratory tract infection and psychogenic cough is unclear at present. One possible explanation is that the primary disease leads to a habitual, subconscious behavioral pattern. And the lower cough threshold caused by upper respiratory tract infection make cough ‘easier’ for patients, and some gradually evolved into ‘no cause’ cough. 16
We found that all patients with somatic cough syndrome had dry cough, while the prevalence of nocturnal cough was significantly lower in the psychogenic compared to the non-psychogenic group. This is in agreement with Gay and Mastrovich who reported lack of nocturnal coughing in five of six adults with somatic cough syndrome.8,10 Haydour et al. 17 conducted a systematic review on 147 patients (including adults and children) and found that only 5% of the patients experienced coughing during sleep. Previous studies show that a ‘barking’ or ‘honking’ cough and absence of nocturnal coughing are indicative of the presence of a somatic cough syndrome.5,10 However, the 2015 American College of Chest Physician cough guidelines suggest that the aforementioned factors are not a decisive diagnostic criterion for psychogenic or habitual cough since other etiologies like bronchiectasis, gastroesophageal reflux disease, and chronic bronchitis may also present with similar characteristics. 18 In our study, although the incidence of nocturnal coughing in somatic cough syndrome was significantly lower than that in non-somatic cough syndrome, there were still a few patients who had nocturnal cough. Therefore, presentation of night cough should not be used to exclude somatic cough syndrome.
There are limited reports on the accompanying symptoms in children and adolescents with somatic cough syndrome. Wright and Balfour-Lynn 15 reported that 64% of the children with habitual/tic cough presented no respiratory symptoms other than cough, whereas 36% had at least one respiratory symptom, such as chest pain, throat discomfort, breathlessness, and wheezing, and 20% of the patients had gastrointestinal symptoms like nausea, vomiting, and abdominal pain. In our study, similar distribution in accompanying symptoms was found between two groups. In addition, there were some examination abnormities as indicated by 24-hour esophageal pH value monitoring, eosinophilia in induced sputum, and/or bronchial hyper-responsiveness. These companying symptoms or abnormal results of investigation may explain that somatic cough syndrome patients were often misdiagnosed as UACS, GERC, EB, or CVA before. Therefore, somatic cough syndrome should be considered if these patients were not responsive to the therapies targeting the potential causes with the different respiratory symptoms or positive results of investigations.
Cough hypersensitivity is a clinical and pathophysiological feature of chronic cough, which has been proposed as the basis of persistence of cough with increasing number of reports detailing the phenotypic aspects of cough hypersensitivity.19–21 In this study, a significant proportion of psychogenic patients also experienced the same type of symptoms of itchy throat, easy cough triggering to smells, cold air, changes in position, tobacco smoke/dust, and so on, as has been described in other chronic cough patients. While the relationship of psychological factors to cough hypersensitivity are not fully understood, we consider that psychogenic cough should be a special type of cough hypersensitivity syndrome. Cough hypersensitivity can be divided into peripheral hypersensitivity and central hypersensitivity. 22 Peripheral hypersensitivity is related with inflammatory mediators, cytokines, nerve remolding, and so on. 23 Somatic cough syndrome is more likely to be related with central hypersensitivity characterized by dysregulation of higher nervous center. A recent study found that central inhibiting function of cough was decreased in refractory chronic cough patients. 24 Further study is needed to identify whether central inhibiting function is decreased and which neural pathway or nucleus is involved in somatic cough syndrome.
Non-pharmacologic interventions like hypnosis, suggestion therapy, cognitive-behavioral therapy, and counseling are most commonly used to treat somatic cough syndrome. Sedative drugs have been effective in some patients that do not respond to non-pharmacologic interventions.25,26 The systematic review conducted by Haydour et al. 17 found low-quality evidence supporting the invention strategies used in those studies. Most patients in our data received a combination of psychological counseling and pharmacologic intervention. The non-pharmacological interventions alone did not significantly alleviate cough symptoms, whereas the combination with psychotropic drugs were effective, which might be related with the relatively rigid modes of thinking, stereotypical values, and strong opinions that are difficult to change in adults compared with children and adolescents. Furthermore, the presence of comorbid psychiatric disorders is another reason why the pharmacologic intervention is needed in adult patients. There is no consensus at present on the duration of non-pharmacologic or drug interventions for somatic cough syndrome. Lokshin et al. 27 found that seven out of nine patients with somatic cough syndrome did not show any recurrence during the average 2.2-year follow-up after suggestion therapy. However, Weinberger 6 reported cough recurrence after cessation of suggestion therapy. The efficacy of non-pharmacologic or pharmacologic interventions should be studies further in a large sample.
There were limitations in the study. One of the biggest challenges in understanding the relationship between psychiatric factors and cough is the bi-directional relationship between the two. It is extremely difficult to ascribe psychological factors as being causal to cough. In the study, the diagnosis of somatic cough syndrome was made, in cooperation with psychiatrist and respiratory specialist. All subjects we enrolled finished full investigations, no potential causes were found or cough could not improve at all after treatment directed to potential conditions. If we doubt cough might be related with psychiatric condition, we then referred the patient to psychiatrist in our hospital further psychogenic evaluation. If patient was considered as somatic cough syndrome, the management directed to somatic cough syndrome would be given, which consisted of psychological counseling, psychotherapy, and/or psychotropic drug. Cough was improved with psychological management. Second, we were not sure whether these psychiatric disorders existed before cough started because psychogenic evaluation was not conducted in most patients before they visited our cough clinic. In our opinion, psychiatric disorders should be existed before cough started. When patients had a common cold or acute upper respiratory tract infection present with cough, cough become a somatic symptom of psychiatric disorders after common cold recovered. Third, we have to admit that not all subjects with preliminary diagnosis of somatic cough syndrome could respond to therapy. The term of unexplained chronic cough would be used if cough did not improve with the psychological management within 1 month.
In conclusion, somatic cough syndrome is common in both young men and women and present as dry cough that is initially triggered by common cold. Somatic cough syndrome is frequently misdiagnosed as common causes of chronic cough due to the presence of accompanying symptoms and abnormal clinical tests. The absence of nocturnal is suggestive less possibility of somatic cough syndrome in adults, but that could not rule it out. The presence of psychiatric comorbidities are reliable diagnostic criteria of somatic cough syndrome. Psychotropic drugs combined with psychotherapy is an effective treatment. Further studies are needed to establish diagnosis and management of somatic cough syndrome in adults.