
Abstract
Background:
The adverse effects of the COVID-19 pandemic on sleep have been well studied. However, whether the COVID-19 pandemic impacted positive airway pressure (PAP) adherence in patients with obstructive sleep apnea (OSA) remains unclear.
Objectives:
To evaluate the impact of the COVID-19 pandemic on adherence to PAP therapy in patients with OSA.
Design:
A retrospective cohort study, systematic review, and meta-analysis.
Data sources and methods:
The retrospective study included adults with OSA who received PAP prescriptions within the year before and the year after the start date of COVID-19 social distancing (22 March 2020) in South Korea. The threshold of clinical significance for PAP adherence was defined as 0.5 h/day. We also searched for relevant studies published up to 15 January 2023 using the MEDLINE and Embase databases. We performed a random-effects meta-analysis of our findings with the identified studies regarding the standardized mean change (SMC) with a 95% CI of PAP adherence.
Results:
Our study included a total of 306 patients (mean age, 59.7 years; men, 73.5%). The average daily PAP usage was 5.10 ± 1.63 h before the COVID-19 pandemic and 4.79 ± 1.96 h during the pandemic (mean difference, −0.31 h/day; 95% CI, −0.46 to −0.15 h/day; p < 0.001 using paired t-test). After identifying 10 observational before-and-after studies through a systematic review, we conducted a meta-analysis that included our original data and showed that adherence to PAP treatment was not different before and during the COVID-19 pandemic (SMC, 0.01; 95% CI, −0.18 to 0.19; p = 0.952).
Conclusion:
Although the COVID-19 pandemic had a statistically negative impact on adherence to PAP treatment in South Korea, the effect was not clinically relevant in patients with OSA. According to our meta-analysis, adherence to PAP treatment was not different before and during the COVID-19 pandemic in patients with OSA.
Trial registration:
PROSPERO database; No.: CRD42023414268; URL: https://www.crd.york.ac.uk/PROSPERO.
Introduction
The global prevalence of obstructive sleep apnea (OSA) has been increasing over the last several decades.1,2 Currently, nearly 1 billion middle-aged people may be affected by OSA worldwide. 3 In South Korea, 8 million people are estimated to have OSA.3,4 Positive airway pressure (PAP) therapy is highly effective in treating OSA, but its efficacy relies heavily on adherence to PAP treatment. 5 However, a meta-analysis that showed trends in PAP adherence indicated that adherence over the last 20 years has remained persistently low, and non-adherence is as high as 30–40%. 6
The adverse effects of the COVID-19 pandemic on sleep – especially poor sleep quality and insomnia – have been documented. 7 However, how the COVID-19 pandemic impacts PAP adherence in patients with OSA is controversial. Studies have reported that PAP adherence significantly increased after lockdowns in France,8–10 Spain, 11 Croatia, 12 and the state of Illinois in the United States. 13 In contrast, research conducted in Turkey 14 showed a decrease in adherence, whereas no difference was reported in studies in the US state of Massachusetts, 15 Thailand, 16 and Poland. 17
Instead of enforcing a national lockdown – the strictest enforcement of physical distancing and one that was frequently implemented by Western countries – the Korean government enacted social distancing on 22 March 2020 to control COVID-19 transmission. 18 In this study, we evaluated the impact of the COVID-19 pandemic on adherence to PAP therapy in patients with OSA in South Korea. To consolidate all available evidence on this issue, we conducted a meta-analysis of our findings with published studies identified through a systematic review.
Methods
Original study: Design and participants
This retrospective cohort study included adults ⩾ 19 years of age with OSA who received PAP prescriptions at Seoul National University Hospital in South Korea within a year before and a year after the start date (22 March 2020) of COVID-19 social distancing. Patients who used PAP devices for less than 90 days before the start of COVID-19 social distancing were excluded.
PAP prescriptions in South Korea
Health insurance in South Korea is provided by the National Health Insurance (NHI) program, which covers 97% of the population and the Medical Aid Program, which covers the low-income population, which represents the remaining 3%. 19 PAP treatment for patients with sleep apnea has been covered in South Korea by the NHI since 1 July 2018 and by the Medical Aid Program since 1 August 2018. Clinicians can issue PAP application forms to register patients with sleep apnea who meet the following coverage criteria: (1) patients with an apnea-hypopnea index (AHI) ⩾ 15/h on type 1 polysomnography or (2) patients with an AHI ⩾ 5/h on type 1 polysomnography with one or more signs or symptoms or comorbidities such as insomnia, daytime sleepiness, decreased cognitive function, mood disorder, hypertension, ischemic heart disease, stroke, or oxygen saturation less than 85%. Then, clinicians can issue PAP prescription forms that include information on the type of PAP device [continuous PAP (CPAP), auto-adjusting PAP (APAP), and bilevel PAP (BPAP)], the pressure of the PAP device, the prescription period, and the average daily PAP usage in hours during the previous prescription period. Average PAP usage is defined as the number of hours of PAP use divided by the number of total calendar days prescribed, which is based on compliance reports downloaded from the PAP device itself or its cloud database used for telemonitoring. After the initial PAP prescription, clinicians can renew prescriptions for patients who meet the adherence criteria: use of the PAP device for at least 4 h/day for 70% of days during a consecutive 30-day period at any time during the first 90 days of the initial prescription. Clinicians periodically renew PAP prescriptions for a maximum of 6 months for patients who meet the initial adherence criteria. Since 10 February 2020, insurance coverage can be extended temporarily without a prescription renewal by a clinician to reduce routine clinic visits by patients. Thus, beneficiaries can choose to continue using their PAP device without renewing their PAP prescription. Since 1 December 2020, the detailed coverage criteria for initial registration for PAP treatment and renewal of PAP prescriptions were revised, which did not influence the results of this study because we included only patients who received PAP prescriptions before 22 March 2020.
Original study: Data collection and outcomes
In addition to information on demographics and comorbidities, the following data were collected by reviewing electronic medical records of PAP application and prescription forms: types of health insurance (NHI beneficiaries versus Medical Aid Program recipients), AHI (⩾15/h versus <15/h), type of PAP device (CPAP, APAP, and BPAP), and average daily PAP usage in hours. The study outcome was the difference in average daily PAP usage in hours before and during COVID-19 social distancing. The clinical significance threshold for adherence to PAP therapy was defined as 0.5 h/day. 20
Original Study: Statistical analysis
Continuous variables were presented as means with SD, and categorical variables were presented as counts and percentages. Missing average daily PAP usage values on PAP prescription forms were imputed using the multivariate imputation by chained equations (MICE, version 3.14.0) package in R (R Foundation for Statistical Computing, Vienna, Austria). 21 The differences in daily PAP usage hours before and during the COVID-19 pandemic were analyzed using paired t-test. We compared the PAP adherence in subgroups of age (⩾60 years versus <60 years); sex; socioeconomic status (NHI beneficiaries versus Medical Aid Program recipients); the presence of comorbidities such as hypertension, type 2 diabetes, cardiovascular disease including ischemic heart diseases, heart failure, stroke or transient ischemic attack, and atrial fibrillation or flutter; OSA severity (AHI ⩾ 15/h versus <15/h); and average daily PAP usage before the COVID-19 pandemic (⩾4 h/day versus <4 h/day). To evaluate factors associated with changes in PAP adherence, we used a linear mixed-effects model with a random intercept for each participant, adjusting for variables selected by the least absolute shrinkage and selection operator (Lasso) method (R-package: glmmLasso, version 1.6.2; R Foundation for Statistical Computing, Vienna, Austria). 22 The Lasso method shrinks some coefficients of variables and sets others to zero, and hence attempts to retain the good variables of subset selection. All comparisons were two-sided, and p values of <0.05 were considered statistically significant. All analyses were performed with R version 4.2.2.
Systematic review: Literature search and eligibility criteria
The systematic review and meta-analysis were performed in accordance with the preferred reporting items for systematic reviews and meta-analyses (PRISMA) statement 23 and the meta-analyses of observational studies in epidemiology (MOOSE) guidelines. 24 The protocol was registered in the international prospective register of systematic reviews (PROSPERO) database (CRD42023414268). The search strategy using MEDLINE is available in e-Appendix 1. MEDLINE and Embase were searched by two independent researchers for relevant studies published up to 15 January 2023. The search was limited to English-language publications, but no other restrictions were applied. We considered eligible studies that included adult patients with OSA who received PAP treatment before the COVID-19 pandemic and reported average daily PAP usage in hours before and during the COVID-19 pandemic. Study selection was conducted by two independent researchers based on the PRISMA flow diagram. 23 The two researchers discussed any disagreements regarding eligibility until a consensus was reached.
Systematic review: Data extraction and quality assessment
The two independent researchers extracted the following data from each included study: the last name of the first author, article type, year of publication, the total number of patients, country, index date of the COVID-19 pandemic, average daily PAP usage in hours before and during the COVID-19 pandemic [mean ± SD or median (interquartile range, IQR)]. The independent researchers assessed the risk of bias using the risk of bias in non-randomized studies – of exposure (ROBINS-E) 25 and discussed any disagreements until a consensus was reached.
Meta-analysis
The primary study outcome was the change in PAP adherence before and during the COVID-19 pandemic. As previously suggested, 26 the missing values for mean (±SD) PAP adherence in each study were estimated from the sample size, median, and IQR. When the missing SD values could not be estimated from available data, the SD of another study conducted in the same country was used instead. The standardized mean change (SMC) with a 95% CI for PAP adherence was calculated using the R-package metafor (version 3.8-1; R Foundation for Statistical Computing, Vienna, Austria) 27 and was used for the summary estimates. We performed a meta-analysis that included our original data using a random-effects model and visualized the analysis with forest plots. Heterogeneity was assessed using the I2 statistic. We conducted a sensitivity analysis by incorporating studies that only included patients with moderate-to-severe OSA (AHI ⩾ 15/h) and the subset of our data for moderate-to-severe OSA. Publication bias was assessed visually using funnel plots and quantitatively using Egger’s and Begg’s tests. All comparisons were two-sided, and p values of less than 0.05 were considered statistically significant. All analyses were performed with R version 4.2.2.
Results
Original study
Among a total of 506 patients with OSA who received PAP prescriptions during the study period, 200 patients who used PAP devices for less than 90 days before the start of COVID-19 social distancing were excluded. Among the 306 study patients (mean age, 59.7 years; men, 73.5%), those with low incomes (i.e. Medical Aid Program recipients) represented 4.6% (Table 1). A quarter of the patients had hypertension and a sixth had type 2 diabetes. A total of 71 (23.2%) patients had cardiovascular disease including ischemic heart disease, heart failure, stroke or transient ischemic attack, and atrial fibrillation or flutter. The majority of patients had moderate to severe OSA (AHI ⩾ 15/h; 88.2%) and used APAP devices (86.3%).
Baseline patient characteristics before the COVID-19 pandemic.
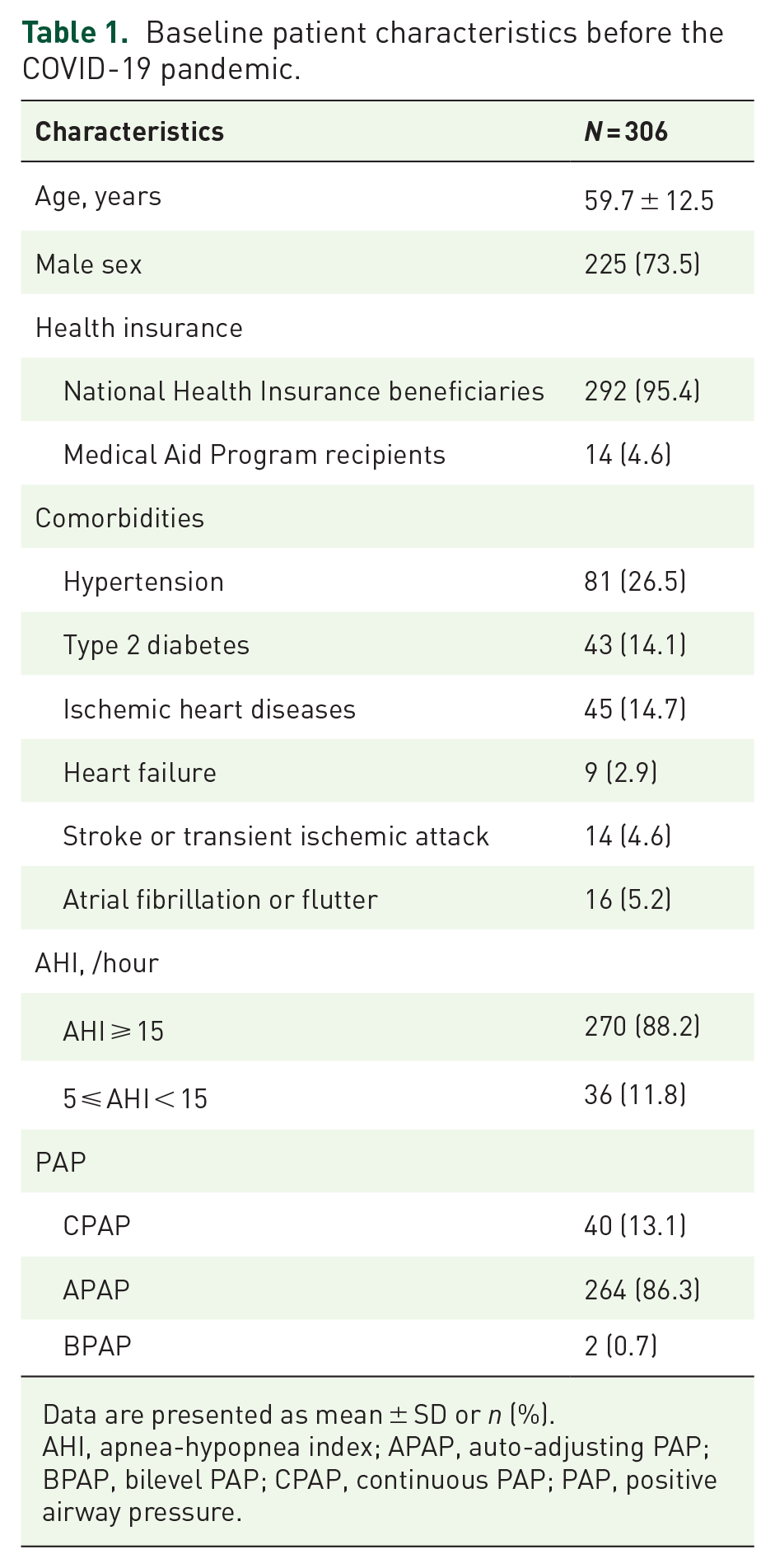
Data are presented as mean ± SD or n (%).
AHI, apnea-hypopnea index; APAP, auto-adjusting PAP; BPAP, bilevel PAP; CPAP, continuous PAP; PAP, positive airway pressure.
The average daily PAP usage was 5.10 ± 1.63 h before the COVID-19 pandemic and 4.79 ± 1.96 h during the pandemic (Figure 1). Although PAP adherence significantly decreased by 0.31 h/day (95% CI, −0.46 to −0.15 h/day; P < 0.001 using paired t-test) during the COVID-19 pandemic, it did not meet the clinical significance threshold of 0.5 h/day for PAP adherence. 20 Results of subsequent analyses with designated subgroups were generally consistent with the main findings (Table 2).

Changes in average daily PAP usage in hours before and during the COVID-19 pandemic.
Changes in average daily PAP usage in hours by subgroup.

p Values were determined using paired t-test.
Cardiovascular disease included ischemic heart diseases, heart failure, stroke or transient ischemic attack, and atrial fibrillation or flutter.
AHI, apnea-hypopnea index; APAP, auto-adjusting PAP; CPAP, continuous PAP; PAP, positive airway pressure.
Similar findings were observed in our linear mixed-effects model that adjusted for age, sex, socioeconomic status, and PAP adherence before the COVID-19 pandemic – variables selected by the Lasso method. PAP adherence decreased by 0.31 h/day (95% CI, −0.46 to −0.15 h/day; p = 0.003 using the linear mixed-effects model) during the pandemic. The interaction between PAP adherence before the pandemic (⩾4 h/day versus <4 h/day) and time (before versus during the pandemic) was significant (p for interaction <0.001). Our model showed that patients who used PAP more than 4 h/day before the pandemic had a greater decrease in their adherence to PAP (−0.44 h/day; 95% CI, −0.61 to −0.27 h/day; p < 0.001 using the linear mixed-effects model; Table 3). However, the difference did not reach the designated clinical significance threshold. 20
Multivariable analysis of changes in average daily PAP usage in hours.

Analyzed using a linear mixed-effects model that adjusted for age (⩾60 years versus <60 years), sex, socioeconomic status (National Health Insurance beneficiaries versus Medical Aid Program recipients), and PAP adherence (⩾4 h/day versus <4 h/day) before the COVID-19 pandemic.
The p value for interaction between average daily PAP usage (⩾4 h/day versus <4 h/day) before the COVID-19 pandemic and time (before versus during the pandemic) was <0.001.
PAP, positive airway pressure.
Systematic review and meta-analysis
We screened 225 articles and identified 13 potentially eligible articles (Figure 2). After full-text review, 10 observational before-and-after studies8–17 met our inclusion criteria. No relevant randomized controlled trials were found. A summary of study characteristics of 11 studies including our study is shown in Table 4. The risk of bias is summarized in Supplemental e-Figure 1. Most studies had a low risk of bias for confounding, measurement of the exposure, post-exposure interventions, and selection of the reported result. However, we observed that three studies had a high or very high risk of bias overall.
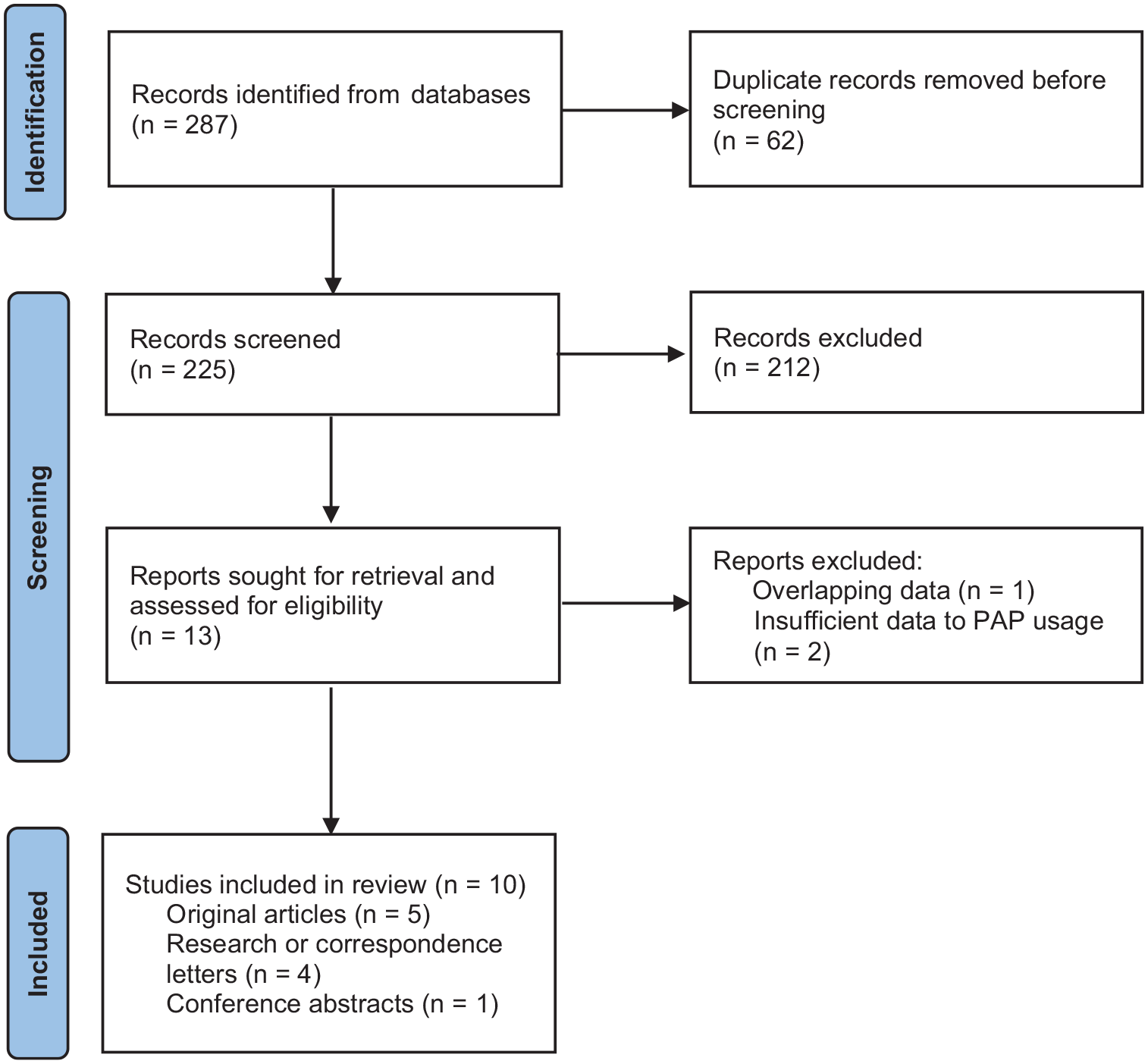
PRISMA flow diagram.
Recent research on PAP adherence and the COVID-19 pandemic.

Data are presented as mean ± SD or median (interquartile range).
AHI, apnea-hypopnea index; NR, not reported; OSA, obstructive sleep apnea; PAP, positive airway pressure.
The random-effects meta-analysis revealed that adherence to PAP treatment was not different before and during the COVID-19 pandemic (SMC, 0.01; 95% CI, −0.18 to 0.19; p = 0.952; Figure 3). Similar findings were observed in a sensitivity analysis incorporating studies for patients with AHI ⩾ 15/h (SMC, 0.03; 95% CI, −0.12 to 0.17; p = 0.725; Figure 4). The test for heterogeneity was significant (Q = 523.61; df = 10; P < 0.0001; I2 = 99.8%). No evidence of publication bias was observed with funnel-plot symmetry (Supplemental e-Figure 2) and the Egger’s (p = 0.588) and Begg’s (p = 0.648) tests.

Forest plot for changes in PAP adherence throughout the COVID-19 pandemic.

Forest plot of sensitivity analysis for changes in PAP adherence: studies only included patients with moderate-to-severe OSA (AHI ⩾ 15/h).
Discussion
Our original study showed that PAP adherence decreased by 0.31 h/day during the COVID-19 pandemic in South Korea relative to the pre-pandemic era; however, this reduction was not clinically relevant for patients with OSA. Our meta-analysis revealed that adherence to PAP treatment was not different before and during the COVID-19 pandemic in patients with OSA.
According to the World Health Organization (WHO), social distancing (often used interchangeably with the term ‘physical distancing’) ensures safe physical distancing by reducing crowding. 18 Social distancing measures range from lockdowns to restrictions on social gatherings in homes and public places.18,28 While avoiding a nationwide lockdown, the Korean government implemented social distancing on 22 March 2020 by restricting unnecessary gatherings and activities to prevent COVID-19 transmission. On 6 May 2020, social distancing was downgraded, and the policy of ‘distancing in daily life’ was introduced. This policy supports a way of life and social interactions that are sustainable and enable society to withstand the potentially lengthy duration of the COVID-19 pandemic. 29 These guidelines consist of four major parts: (1) five key rules for personal distancing; (2) four complementary actions for personal distancing; (3) five key rules for collective distancing; and (4) detailed guidelines for physical distancing in daily life for communities and organizations. 29 The five key rules for personal distancing comprise the following: (1) staying home for 3–4 days if an individual feels unwell, (2) keeping a distance of two arms’ lengths from others, (3) washing hands for 30 s and coughing or sneezing into the sleeve, (4) ventilating spaces at least twice daily and disinfecting regularly, and (5) staying connected while physically distancing. 29
Data are limited on how the COVID-19 pandemic and related social distancing measures (excluding lockdowns) impact PAP adherence in patients with OSA. According to our original study, PAP adherence decreased by 0.31 h/day during the COVID-19 pandemic relative to the pre-pandemic era in the unadjusted and adjusted models. Our adjusted model showed that patients who used PAP for 4 h/day or more before the pandemic had a greater decrease (0.44 h/day) in their adherence to PAP compared with those who used PAP for less than 4 h/day before the pandemic. However, the difference did not reach the designated clinical significance threshold of 0.5 h/day for PAP adherence. 20
Although the impact of the COVID-19 pandemic on PAP adherence was clinically irrelevant in our study, the pandemic had a statistically significant negative effect on PAP adherence. This finding differed from those of studies in Western countries that implemented national lockdowns.8–13 Pépin et al. reported that PAP adherence significantly increased from 6.45 h/day to 6.90 h/day after the first national lockdown in France. 9 A similar finding was observed after the lockdown in Spain. 11 The authors speculated that the lockdowns restricted individuals’ activities and forced them to stay home, thereby increasing sleep duration and the nighttime use of PAP.8,9 Such speculation could not be applied in South Korea, where social distancing was implemented instead of national lockdowns. Various non-pharmaceutical measures against the COVID-19 pandemic may explain the varying impacts of the pandemic on PAP adherence in individuals with OSA.
Given that the variable impact of the COVID-19 pandemic on PAP adherence has been reported, we performed a meta-analysis of our study with 10 published studies identified with a systematic review. The meta-analysis revealed that adherence to PAP treatment was not different before and during the COVID-19 pandemic in patients with OSA. However, considerable heterogeneity was observed among included studies. This interstudy heterogeneity may be attributed to several factors. First, despite the global nature of the COVID-19 pandemic, its evolution and impact on public health have varied by country and region. Second, non-pharmaceutical interventions against the COVID-19 pandemic have ranged from social distancing to complete lockdown. Moreover, detailed social distancing or lockdown measures have differed by country and by pandemic phase. Third, the implementation and accessibility of telemedicine for PAP treatment may have been an important factor in maintaining PAP adherence when access to clinics was limited during the pandemic. However, the utilization of telemedicine differed across countries and regions.
The limitations of our study should be acknowledged. Our original study has several limitations, including its retrospective cohort design at a single institution. Because we included patients who received PAP prescriptions, those who used PAP therapy but did not receive or renew PAP prescriptions were excluded. Especially, to reduce routine clinic visits – since February 10, 2020 – patients were allowed to temporarily extend their insurance coverage without the renewal of the PAP prescription, which could have resulted in selection bias. In addition, there could be missing values or errors in the average daily PAP usage in hours, as we obtained it from medical records of PAP prescription forms. Although the average daily PAP usage in PAP prescription forms was based on compliance reports downloaded from the PAP device itself or its cloud database, we could not check compliance reports themselves because they were not scanned or uploaded into electronic medical records. Such non-differential measurement errors could have led to a bias toward the null, but the negative effect of the COVID-19 pandemic on PAP adherence was statistically significant in our study. Moreover, we imputed missing average daily PAP usage values to reduce the risk of bias due to missing data. Our meta-analysis also had several limitations. As discussed above, we found significant interstudy heterogeneity. Nevertheless, the sensitivity analysis that integrated studies on patients with moderate-to-severe OSA showed consistent findings. In addition, there is a substantial risk of bias from observational studies. Thus, the results of our systematic review and meta-analysis should be interpreted with caution.
In conclusion, although the COVID-19 pandemic had a statistically negative impact on adherence to PAP treatment in South Korea, the effect was not clinically relevant in patients with OSA. According to our meta-analysis, adherence to PAP treatment was not different before and during the COVID-19 pandemic in patients with OSA.
Supplemental Material
sj-docx-1-tar-10.1177_17534666231214040 – Supplemental material for Impact of the COVID-19 pandemic on adherence to positive airway pressure treatment in patients with obstructive sleep apnea: systematic review and meta-analysis
Supplemental material, sj-docx-1-tar-10.1177_17534666231214040 for Impact of the COVID-19 pandemic on adherence to positive airway pressure treatment in patients with obstructive sleep apnea: systematic review and meta-analysis by Soomin Jo and Jaeyoung Cho in Therapeutic Advances in Respiratory Disease
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.