
Abstract
Background:
The use of maintenance medication in patients with chronic obstructive pulmonary disease (COPD) in real life is known to deviate from recommendations in guidelines, which are largely based on randomized controlled trials and selected populations.
Objectives:
We used the COSYCONET (
Design:
COSYCONET is an ongoing, multi-center, non-interventional cohort of patients with COPD.
Methods:
Patients with COPD of Global Initiative for Chronic Obstructive Lung Disease (GOLD) grades 0–4 participating in visits 1–5 were included. Data covered the period from 2010 to 2018. Generalized linear models were used to examine the relation of COPD characteristics to different types of respiratory medication.
Results:
A total of 1043 patients were included. The duration of observation was 4.5 years. Use of respiratory medication depended on GOLD grades 0–4 and groups A-D. Long-acting muscarinic antagonist therapy increased over time, and was associated with low carbon monoxide (CO) diffusing capacity, while inhaled corticosteroid (ICS) use decreased. Active smoking was associated with less maintenance therapy in general, and female sex with less ICS use. From the eight items of the COPD Assessment Test, only hill and stair climbing were consistently linked to treatment.
Conclusion:
Using data from a large, close to real-life observational cohort, we identified factors linked to the use of various types of respiratory COPD medication. Overall, use was consistent with GOLD recommendations. Beyond this, we identified other correlates of medication use that may help us to understand and improve therapy decisions in clinical practice.
Trial registration:
ClinicalTrials.gov NCT01245933.
Keywords
Introduction
Chronic obstructive pulmonary disease (COPD), as a common respiratory disease globally, requires substantial resources for its treatment. 1 In addition to smoking cessation, inhaled medications such as bronchodilators and inhaled corticosteroids (ICS) are of major importance for managing the disease. Various recommendations have been made on the basis of patients’ clinical and functional characteristics, 2 largely relying on data from randomized controlled trials (RCTs) in well-defined and selected groups of patients. Several studies, however, have found therapy in ‘real-life’ to be only partially concordant with these recommendations. 3 Furthermore, comorbidities might influence therapy choice – although such patients are typically excluded from RCTs. Moreover, recommendations have evolved and changed over time.4–7 It was thus of interest to analyze which COPD characteristics were associated with patterns of COPD therapy under real-life conditions
We therefore analyzed data from the COPD cohort COSYCONET. 8 To reflect clinical practice as closely as possible, COSYCONET recruited not only patients of Global Initiative for Chronic Obstructive Lung Disease (GOLD) spirometric grades 1–4 (i.e. with a post-bronchodilator ratio of forced expiratory volume in 1 s to forced vital capacity [FEV1/FVC] <0.7), 1 but also those with a diagnosis of COPD who had a higher FEV1/FVC ratio, formerly named GOLD 0.9,10 This is relevant, as these patients represent a significant percentage of the COPD population and often receive COPD medication,11–14 and thus should be included into the analysis. Importantly, since COSYCONET is collecting data over a prolonged period, we could potentially address the question of whether patterns of medication use have changed over time.
Materials and methods
Study population
COSYCONET is an ongoing, multi-center, non-interventional cohort of patients with COPD of GOLD grades 0–4,1,10 that is being conducted in 31 study centers across Germany. Details of its design and the baseline characteristics of participants have been reported previously. 8 Regular follow-up visits 2–5 were conducted 6, 18, 36, and 54 months after enrolment, which started at the end of 2010 and was completed at the end of 2013, with the follow-up period covering 4.5 years. 15 Patients were required to be free of exacerbations for at least 4 weeks prior to each visit. COSYCONET has been approved by the ethics committees of all study centers, was performed in accordance with the Declaration of Helsinki, and was registered at ClinicalTrials.gov: NCT01245933. All participants provided written informed consent. The reporting of this study conforms to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement. 16
Assessments
Baseline characteristics included age, sex, and body mass index (BMI), smoking status, COPD duration prior to enrolment, and post-bronchodilator lung function, with FEV1 and FVC measured following GOLD recommendations, 1 using Global Lung Function Initiative (GLI) equations to express the results as % predicted. 11 Body plethysmography was used to determine residual volume (RV) and total lung capacity (TLC), also deriving the RV/TLC ratio. Single-breath diffusing capacity for carbon monoxide (CO) comprised the transfer factor (TLCO) and the transfer coefficient (KCO, ratio of TLCO to alveolar volume), which were again expressed relative to GLI reference values. 12 Following the 2017 GOLD recommendations, 1 patients were categorized at each visit in spirometric GOLD grades 1–4 (FEV1/FVC < 0.7), as well as groups A to D based on symptoms [modified Medical Research Council (mMRC) dyspnea scale] and exacerbation history. Moreover, we included two categories of patients with a preserved FEV1 to FVC ratio (⩾0.7) – either FEV1 <80% predicted (preserved ratio, impaired spirometry [PRISm]), and FEV1 ⩾80% predicted (non-PRISm) 17 per visit. All eight items of the multidimensional COPD Assessment Test (CAT, Supplemental Table S1) were used to distinguish between symptoms ranging from cough, sputum, and dyspnea to limitations of activity and self-confidence.18–20 Self-reported comorbidities based on physicians’ diagnoses were recorded, including asthma, cardiac disease, diabetes mellitus and osteoporosis. 21 For generic quality of life, the visual analog scale (VAS) of the EuroQoL-5-dimension (EQ-5D-3L) questionnaire was used. Patients’ characteristics and measured values were determined in the same manner at all visits. 8
Respiratory medication
The use of medication was assessed at each visit via Anatomical Therapeutic Chemical classification codes. 22 Respiratory maintenance medication included long-acting beta2-agonists (LABA), long-acting muscarinic antagonists (LAMA) and inhaled corticosteroids. These compounds were evaluated as single substances, and in the combinations LABA+ICS, LABA+LAMA, or triple therapy.
Statistical analysis
For descriptive purposes, mean values and standard deviations, median values, or numbers and percentages are given, depending on the type of data and their distribution. Generalized linear models with repeated-measures design and logit link (equivalent to longitudinal logistic regression analysis) were used to examine the relationship of predictors to medication. 15 Thus, all associations identified describe combined cross-sectional and longitudinal relationships. The presence of a specific respiratory medication was the binary dependent variable, in terms of any LABA, any LAMA, or any ICS, as well as the combinations of any LABA+ICS, any LABA+LAMA, or triple therapy. Predictors at each visit were demographic and baseline characteristics including sex, BMI category ⩾30 kg/m² as marker of obesity, age category ⩾65 years as marker of higher age, active smoking status versus ex/never, GOLD grades (with grade 1 as reference), non-PRISm-GOLD 0, PRISm, and GOLD groups (with group A as reference), the comorbidities asthma, cardiac disease (comprising coronary artery disease, heart failure, cardiac infarction), diabetes mellitus and osteoporosis, EQ-5D-3L VAS, duration of COPD, TLCO category ⩽65% predicted as surrogate marker of lung emphysema, and each CAT item. Four indicator variables representing visits 2–5 were included, relative to visit 1 which served as reference.
Patients had to complete visit 5 to be eligible for this analysis. There were single patients in whom one of the planned interim visits was missing mainly due to organizational reasons. Of the 1043 patients at visit 1, data was missing for 13 patients at visit 2, 6 patients at visit 3, and 5 patients at visit 4. The respective visit of each patient was omitted from the longitudinal analysis. p Values <0.05 (two-sided) were considered statistically significant. Analyses were performed using procedures including GENLIN from the software package IBM SPSS Statistics (Version 26.0.0.0, Armonk, NY, USA).
Results
Study population
At visit 1, 2741 patients were included, 8 with 206/962/874/249 patients of initial GOLD grades 1–4, and 450 patients GOLD 0. Of these, 1043 participated in the study until visit 5, the functional and clinical characteristics of whom are given in Table 1. Mean FEV1 % predicted, FVC % predicted, FEV1/FVC, RV/TLC, TLCO % predicted, KCO % predicted, total CAT score, and EQ-5D-3L VAS significantly differed over the five visits, as did the proportion of active smokers (p < 0.05).
Patient characteristics.

Data are given as mean ± standard deviation, or number (percentage). GOLD grades 0–4 and groups A–D refer to Global Initiative for Chronic Obstructive Lung Disease (GOLD) criteria. Statistical comparisons of continuous variables between visits were performed by repeated-measures ANOVA.
According to contingency tables and chi-square statistics of yes/no categories versus visits 1–5.
According to contingency tables and chi-square statistics of all four categories of either grades 1–4 or groups A–B versus visits 1–5.
BMI, body-mass index; CAT, COPD Assessment Test; EQ-5D-3L VAS, EuroQoL 5 dimension EQ-5D-3L visual analog scale; FEV1 = forced expiratory volume in 1 s; FVC, forced vital capacity; GLI, Global lung function initiative; KCO, transfer coefficient for carbon monoxide; PRISm, preserved ratio, impaired spirometry; RV/TLC, ratio of residual volume to total lung capacity; TLCO, transfer factor for carbon monoxide.
Respiratory medication at visits 1–5
Use of respiratory maintenance medication over visits is shown in Figure 1. The overall mean percentage of patients receiving any LABA was 77.4%, and percentages did not show a trend over visits. The use of any ICS was reported overall by 59.9% of patients, with a non-significant decrease from visit 3 to 5. In contrast, overall LAMA use was 69.9%, with a significant increase over visits (p < 0.001). A similar picture emerged for the combined treatments: While there was no significant trend for LABA+ICS use (with overall use of 57.2%), or triple therapy (overall 46.0%), dual bronchodilation with LABA+LAMA significantly increased over visits (p < 0.001), with an overall use of 61.5%.
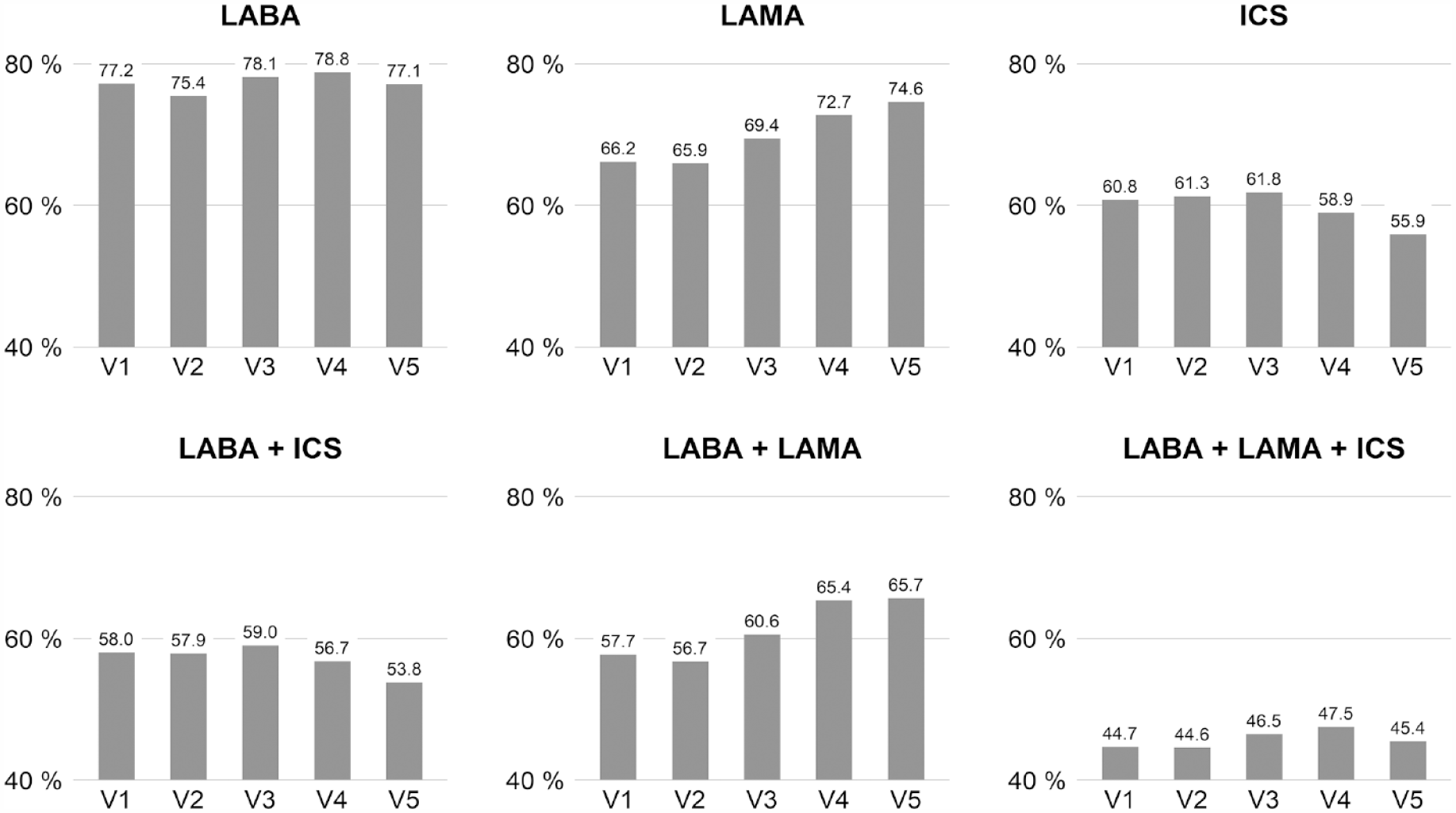
Prevalence of respiratory maintenance medication at visits 1–5 (N = 1043). LABA = long-acting beta2-agonists; LAMA = long-acting muscarinic antagonists; ICS = inhaled corticosteroids. Compounds were evaluated as single substances as well as in usual combinations. The p values refer to the analysis of contingency tables comprising all five visits by chi-square statistics.
Association between medication and COPD characteristics
The relationship between each of the six medication groups and patient characteristics is illustrated in Figure 2(a) and (b); numerical values of the parameter estimates are given in Supplemental Tables S2A and S2B.

(a) and (b) Results from generalized linear models for respiratory medication as (binary) dependent variable given in the headline of each subpanel. Panel A comprises the three subpanels referring to the single compounds, panel B the three subpanels referring to the three combinations. Odds ratios of each predictor with 95% confidence intervals are listed as rows, and odds ratios are shown on the horizontal axis which has been chosen to be identical for better comparability. Odds ratios were converted via exponentiation (base e) from the estimates given in the Supplemental Tables S1A and B. Visits 2–5 refer to visit 1 as reference, GOLD grades 2–4 refer to GOLD grade 1 as reference, as well as GOLD 0, either as PRISm or no PRISm. PRISm = preserved ratio impaired spirometry (for definition see text). GOLD groups B to D refer to GOLD group A as reference; EQ-5D-3L VAS = EuroQoL 5 dimension visual analog scale; TLCO = transfer factor of single-breath diffusing capacity for CO; BMI = body mass index; smoking refers to active smoking (yes versus no). The corresponding numerical values are given in the Supplemental Tables S1A and B.
GOLD grades and groups
Therapy with LABA, LAMA or ICS, or the combinations LABA+ICS, LABA+LAMA, and triple therapy was related to spirometric COPD severity as indicated by odds ratios of GOLD grades 2–4 compared to grade 1 that were significantly (p < 0.05) greater than 1 and increased with increasing grade. Conversely, patients of non-PRISm-GOLD grade 0 less often received LAMA and LABA, and there was also lower use of LABA+LAMA and triple therapy than in those with GOLD grade 1. In contrast, patients in the PRISm group had similar use of all medication categories to those in GOLD grade 1. Patients in GOLD groups C and D were more likely to use the six medication categories than those in group A; patients in group B were only more likely to use LAMA, or LABA+LAMA, with a tendency for triple therapy.
Anthropometric characteristics and diffusing capacity
Female sex correlated with lower use of ICS, LABA+ICS, and triple therapy (p < 0.05). Elevated BMI was associated with higher use of LABA, while there were no correlations between higher age and any maintenance medication category. For all six medication categories, active smoking was associated with significantly lower use compared with non- or ex-smokers. A longer time since COPD diagnosis was linked to increased use of ICS and LABA+ICS, with a tendency for increased triple therapy, suggesting an overall increased utilization of ICS in patients with a longer history of COPD. A reduction in CO diffusing capacity (TLCO) was associated with higher use of LABA, LAMA, LABA+LAMA, and triple therapy but not of ICS per se or LABA+ICS, suggesting that ICS were primarily given in combination with LAMA.
Comorbidities
An asthma diagnosis was linked to higher use of all maintenance medication categories with the exception of LAMA. In contrast, the presence of diabetes was linked to lower use of all compounds and combinations, although not significantly for LABA. There were no correlations between cardiac disease or osteoporosis and any medication category.
Symptoms and quality of life
The presence of phlegm (CAT item 2) positively correlated (p < 0.05) to LABA+ICS and triple therapy use, with difficulties in climbing hills or stairs (CAT 4) correlating with increases in all six medication categories. The feeling of less energy (CAT 8) was associated with less prescription of LABA only. There were no associations between medication category and any other CAT item. A higher generic quality of life in terms of EQ-5D-3L VAS correlated with increased use of LABA, ICS, LABA+ICS, and triple therapy, but not with LAMA or LABA+LAMA use.
Discussion
This study examined the relationship between the use of six COPD maintenance medication categories and a panel of clinical and functional characteristics in patients with COPD. The findings obtained in a large observational COPD cohort indicate an increase in LAMA use over the time period from 2010 to 2018. As expected, higher GOLD grades and groups were associated with higher use of all compounds. Active smoking and the diagnosis of diabetes were associated with less maintenance use in general, and female sex with less use of ICS-containing medication. It seems noteworthy that among the symptoms covered by the CAT questionnaire, only difficulty in climbing hills or stairs was consistently linked to increased use of all medication categories. Finally, most medication categories, especially LABA+ICS and triple therapy, were associated with higher quality of life. Overall, these findings demonstrate that in clinical practice, although GOLD categories appear to be major determinants of medication selection, as recommended, further patient characteristics including specific symptoms, particularly limitations in exercise capacity may guide the choice.
Patients of GOLD groups C and D received more therapy than the reference group GOLD A, 1 with use of LAMA (either mono or dual bronchodilation) increasing over time, whereas that of ICS tended to decrease. This difference in therapy was consistent with treatment recommendations at the time of the study. The 2023 update to GOLD recommendations combined the previous groups C and D into the new group E. 23 Interestingly, the parallel medication use in groups C and D indicates that this update is consistent with treatment choices already used by treating physicians. The intensity of medication also increased with increasing GOLD grades 1–4, while patients of grade 0 had less medication use, if categorized as non-PRISm. In contrast, patients categorized as PRISm used similar patterns of medications to those categorized as GOLD grade 1 (the reference category), suggesting that these two groups showed the same relationships between clinical measures and medication. A comparison of the magnitude of coefficients (see Supplemental Table S2A and Figure 2) suggested that overall, the association of medication with GOLD grades was similarly strong as that with GOLD groups.
We observed positive associations between generic quality of life and the use of COPD maintenance medication, suggesting an overall benefit. Interestingly, this positive association occurred only when data were adjusted for the COPD characteristics in the present analysis. Without adjustment, the sign of coefficients reversed indicating negative associations, which is understandable as more severely ill patients with lower quality of life are likely to receive more medication. This observation underlined the importance of adjustment for the state of the disease, including comorbidities, when studying associations of medication use with health outcomes in observational settings, in accordance with previous findings in the COSYCONET cohort. 24
Active smokers were less likely to use all medication categories studied. As the effects of medication are known to be reduced in smokers, 25 one might have expected a higher use to compensate for this. One explanation could be that active smokers had less severe COPD, and indeed patients in GOLD grades 1/2 were more likely to be smokers than those in GOLD 3/4 (26% versus 15% at visit 1), as were those in GOLD group A versus BCD (25% versus 19%). However, since we accounted for severity in our analyses and it seems unlikely that smokers refused maintenance therapy, it is perhaps more likely that treating physicians were reluctant to prescribe this therapy in current smokers. In addition, the perceived risk of side effects from ICSs, especially osteoporosis, might explain why female patients were less likely to receive ICS-containing therapy than males. Patients with lower-than-average TLCO had an increased likelihood of LAMA-containing medication use, perhaps due to the fact that TLCO is a marker of lung emphysema, 26 and that LAMAs which are generally recognized as ‘typical’ COPD therapy might more often be prescribed in patients with the diagnosis or suspicion of emphysema, although currently there is no convincing evidence that patients with emphysema show a good response to LAMA treatment. Although the present data are only observational, they support the idea of considering the potential value of TLCO as additional lung function measure in future refinements of treatment recommendations.
Obesity was associated with slightly higher use of LABA only. It is increasingly recognized that obesity can be associated with mechanically induced airway obstruction imposed by factors acting from outside the lung, 27 which can aggravate the obstruction caused by lung disease. Patients with obesity had higher FEV1 and lower FVC % predicted values than those without (64.6% versus 60.3% and 80.5% versus 83.8%, respectively, at visit 1). Furthermore, in a previous analysis we have shown that obesity-induced obstruction, indicated by the ratio of total to effective specific airway resistance was often increased in obese patients, indicating a specific form of body plethysmographic breathing loops that is characteristic of obesity-induced airway obstruction. 27 As this type of obstruction is unlikely to be sensitive to anti-inflammatory therapy and associated to symptoms and physical limitations, its presence may increase the likelihood of administering (additional) LABA bronchodilator therapy. The assessment of obesity-induced airway obstruction is worthy of further consideration in view of the prevalence of obesity. 27
While the association of ICS-containing medication with asthma was not surprising and in line with former cross-sectional results, 3 the negative relationship between all medications, except any LABA, with diabetes was unexpected. Patients with diabetes were slightly more often in GOLD groups B/D compared to those without (42% versus 36%), that is, they were more symptomatic. This should have resulted in higher therapy use rather than lower. However, patients with diabetes were more often in spirometric GOLD grade 0 than those without (22% versus 15%), which would be consistent with lower maintenance therapy use. It is possible that the higher level of symptoms was related to a higher frequency of obesity, so favoring a restrictive pattern of ventilator disorder (see above). As we accounted for covariates in a broad panel of COPD characteristics, the explanation remains unclear and deserves further research. Additional research might also be justified by the prior observation that patients with comorbid COPD and diabetes have a specific COPD phenotype and disease course, potentially related to their diabetes medication.26,28
The eight-item CAT is often used to assess patients’ clinical state in both trials and clinical practice. In previous analyses we demonstrated that the commonly used total score might provide even less information than single items.20,29 This was the reason why we used the individual items in these analyses. Indeed, only two were related to medication use: While phlegm (item 2) correlated only to LABA+LAMA use, difficulty in hill and stair climbing (item 4) was associated with all six medication categories. The coefficients were positive, indicating more symptoms in the presence of therapy, or more therapy in the presence of symptoms. This could be interpreted as an indication that the treating physicians used these disease impacts, all of which are highly relevant to patients’ daily life, as indicators for the need for treatment.
These observations regarding CAT emphasize the difficulties inherent in attempts to conduct a causal analysis of clinical characteristics in patients receiving long-term maintenance therapy that is aiming to improve these characteristics. Of course, this raises the question of actual adherence to therapy in the patients studied. At each visit, COSYCONET patients were asked to bring all of their medication with them, which was then coded and categorized. 22 It is certainly true that possession does not imply intake, but in a COSYCONET substudy, we observed very high adherence to medication, of at least 90%. This favors the assumption that the associations of COPD characteristics with COPD maintenance medication reflected the combined effects of disease severity, actual treatment, and effects on the disease state. We would like to emphasize that we aimed to describe the relationship between clinical characteristics and prescription under conditions as close as possible to real-world circumstances, which precluded selection of subpopulations according to comorbidities such as asthma or conditions such as GOLD 0.
Limitations
As in any observational study, we assessed only associations (and not causation), but these seemed plausible and robust. Data on comorbidities were taken from patients’ reports of physician-based diagnoses and were not validated by independent procedures. However, all previous analyses of COSYCONET data that used these data yielded plausible results. We cannot exclude that economic factors played a role in the prescription behavior, but this is not very likely, as reimbursement of medication costs is high in Germany. In addition to international recommendations, 1 national guidelines exist,30–34 which are, in general, very similar and show only minor differences. 35 For the present analysis, GOLD 2017 recommendations were used for all patients to achieve a consistent evaluation. Although COPD categorization and treatment recommendations have developed since the start of COSYCONET in 2010,1,9,23 the consistency of our results and the fact that these changes were relatively small supports the validity of our conclusions.
Conclusion
In an observational cohort of patients with COPD, use of maintenance COPD medication, including LABA, LAMA, ICS, and their combinations was dependent on disease severity as indicated by GOLD grades and groups. Importantly, while the data illustrated a pattern of medication use under close to real-life conditions that was consistent with that of guideline recommendations, we also identified other, more specific correlates of medication use that may help us to understand and potentially refine therapy decisions in clinical practice.
COSYCONET Study Group
Andreas, Stefan (Lungenfachklinik, Immenhausen); Bals, Robert Universitätsklinikum des Saarlandes); Behr, Jürgen and Kahnert, Kathrin (Klinikum der Ludwig-Maximilians-Universität München); Bahmer, Thomas (Universitätsklinikum Schleswig Holstein) and Bewig, Burkhard (Städtisches Krankenhaus Kiel); Ewert, Ralf and Stubbe, Beate (Universitätsmedizin Greifswald); Ficker, Joachim H. (Klinikum Nürnberg, Paracelsus Medizinische Privatuniversität Nürnberg); Grohé, Christian (Ev. Lungenklinik Berlin); Held, Matthias (Klinikum Würzburg Mitte gGmbH, Standort Missioklinik); Behr, Jürgen and Henke, Markus (Asklepios Fachkliniken München-Gauting); Herth, Felix (Thoraxklinik Heidelberg gGmbH); Kirsten, Anne-Marie and Watz, Henrik (Pneumologisches Forschungsinstitut an der Lungenclinic Grosshansdorf GmbH); Koczulla, Rembert (Schön Klinik Berchtesgadener Land); Kronsbein, Juliane (Berufsgenossenschaftliches Universitätsklinikum Bergmannsheil, Bochum); Kropf-Sanchen, Cornelia (Universitätsklinikum Ulm); Herzmann, Christian (Forschungszentrum Borstel); Pfeifer, Michael (Klinik Donaustauf); Randerath, Winfried J. (Wissenschaftliches Institut Bethanien e. V., Solingen); Seeger, Werner (Justus-Liebig-Universität Gießen); Studnicka, Michael (Uniklinikum Salzburg); Taube, Christian (Ruhrlandklinik gGmbH Essen); Timmermann, Hartmut (Hamburger Institut für Therapieforschung GmbH); Alter, Peter; Schmeck, Bernd and Vogelmeier, Claus (Universitätsklinikum Gießen und Marburg GmbH, Standort Marburg); Welte, Tobias (Medizinische Hochschule Hannover); Wirtz, Hubert (Universitätsklinikum Leipzig).
The study was based on patients recruited within the COSYCONET framework (ClinicalTrials.gov, Identifier: NCT01245933). For further information see Karch et al.
Supplemental Material
sj-docx-1-tar-10.1177_17534666231208584 – Supplemental material for Clinical factors linked to the type of respiratory medication in COPD: results from the COSYCONET cohort
Supplemental material, sj-docx-1-tar-10.1177_17534666231208584 for Clinical factors linked to the type of respiratory medication in COPD: results from the COSYCONET cohort by Peter Alter, Kathrin Kahnert, Franziska C. Trudzinski, Robert Bals, Henrik Watz, Tim Speicher, Sandra S�hler, Tobias Welte, Klaus F. Rabe, Emiel F. M. Wouters, Claus F. Vogelmeier and Rudolf A. J�rres in Therapeutic Advances in Respiratory Disease
Footnotes
Acknowledgements
We are grateful to all COSYCONET study centers, especially to all study nurses, for their excellent and enduring work in data collection, as well as to all patients who were willing to participate in this study over an extended period of time. We also thank David Young for helpful comments on the manuscript.
Declarations
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.