
Abstract
Background:
The long-term efficacy of the Dumon stent in the treatment of benign airway stenosis is unclear.
Objective:
The objective of this study was to evaluate the long-term efficacy and safety of the Dumon stent in patients with benign airway stenosis.
Methods:
We retrospectively reviewed patients with benign airway stenosis who were treated with a Dumon stent at the First Affiliated Hospital of Guangzhou Medical University between March 2014 and October 2021. We included patients with successful removal of silicone stents after implantation. The clinical data and information on bronchoscopic interventional procedures and related complications were collected and analyzed.
Results:
Ninety-nine patients with benign airway stenosis were included. The stent was placed mainly in the trachea (44.4%) and left main bronchus (43.4%). The main type of stenosis was post-tuberculosis bronchial stenosis (57.6%). The overall cure rate was 60.6%. Stent-related complications included retention of secretions (70.7%), granuloma formation (67.7%), stent angulation (21.2%), and stent migration (12.1%). The stent was less effective for left main bronchus stenosis (p = 0.012). Multivariate logistic regression analysis identified that stent placement for more than 13 months, a stent-intervention number of ⩽ 1 predicted a favorable outcome.
Conclusion:
The efficacy and safety of the Dumon stent for benign airway stenosis need improvement. The stent is less effective for left main bronchus stenosis; regular follow-up is required in such cases. Stent placement for > 13 months and no more than once stent intervention within a 6-month period were associated with a favorable outcome.
Introduction
Benign airway stenosis refers to a narrowing of the airway as a result of the destruction of the airway wall, which can occur in various non-malignant diseases. Patients with benign airway stenosis can present with cough, hemoptysis, wheezing, or even dyspnea. The common types of airway narrowing are post-tuberculosis bronchial stenosis (PTBS), post-intubation tracheal stenosis (PITS), and post-tracheotomy tracheal stenosis (PTTS).1–3 Surgery is considered to be the primary treatment for benign airway stenosis and had a success rate of up to 95% in a study with a follow-up duration of 53 months. 4 However, not all patients are suitable for surgery on account of poor cardiopulmonary status, an excessively long stenotic segment (>5 cm), or other surgical contraindications. 5 With the development of endoscopic technology, more treatments are available for benign airway stenosis, including balloon dilatation, argon plasma coagulation, electrotome, laser, cryotherapy, and stent implantation. 3
Currently, implantation of a stent, particularly a silicone stent, is preferred in patients with airway stenosis who are not candidates for surgery and is considered the ‘gold standard’ treatment for benign airway stenosis. 6 Symptoms are rapidly relieved and lung function is improved after stent implantation in almost all patients. 7 However, reports on the efficacy of the silicone stent vary widely according to the number of patients investigated and the experimental design,8–10 and there is still no consensus on the efficacy of silicone stents in the treatment of patients with benign airway stenosis, especially their long-term efficacy. Moreover, the optimal timing for the removal of these stents continues to be debated. Premature stent removal increases the likelihood that the stenosis will recur. Conversely, a prolonged stent dwell time may increase the risk of stent-related complications. 11 Therefore, determining the optimal timing of removal may improve the cure rate achieved by these stents. In this study, we retrospectively reviewed our experience of the long-term efficacy and safety of silicone stents in the treatment of non-neoplastic airway stenosis.
Materials and methods
Patients
We reviewed the clinical data of patients with benign airway stenosis who were treated with Dumon stents at the First Affiliated Hospital of Guangzhou Medical University between March 2014 and October 2021 and for whom long-term follow-up data were available. The study inclusion criteria were as follows: benign airway stenosis diagnosed by bronchoscopy; successful removal of silicone stents after implantation; and a follow-up duration of more than 6 months after stent removal. Patients with neoplastic airway obstruction, those with a follow-up duration of less than 6 months after stent removal, those who underwent silicone stent implantation without removal, and those with airway fistula were excluded (Figure 1).

Flowchart of study population selections and outcomes.
Information on general clinical characteristics, diagnoses, interventional bronchoscopic procedures, and follow-up data was retrieved and analyzed. The study was approved by the ethics committee of the First Affiliated Hospital of Guangdong Medical University (ethics review number 2018-16). Informed consent was obtained from all study participants.
Interventional procedure
A preprocedural imaging evaluation of the airway anatomy was performed in all patients using three-dimensional computed tomography image reconstruction and bronchoscopy (BF-260, Olympus Corporation, Tokyo, Japan). Under general anesthesia, a rigid bronchoscope (Storz Medical AG, Jena, Germany) was advanced through the trachea into the stenotic airway segment, after which the silicone stent (Dumon, Novatech, France) was directly implanted. Bronchoscopic treatments, including electrosurgery, balloon bronchoplasty, and cryotherapy were used to dilate the airway as needed. The attending physician decided the timing of stent removal according to tolerability and the status of the airway.
Assessment of severity of airway stenosis
The severity of airway stenosis was assessed using the Freitag classification, 12 whereby stenosis is classified according to the ratio of the stenotic cross-sectional area to the normal cross-sectional area of the trachea as grade I (<25%), grade II (26%–50%), grade III (51%–75%), grade IV (76%–90%), or grade V (90% to complete obstruction).
Evaluation of efficacy and safety
The airway stenosis was considered cured if the bronchoscopy determined the severity of airway stenosis has significantly improved after 6 months post stent removal. The safety evaluation was based on stent-related complications, including granuloma formation (moderate to severe), secretion retention (moderate to severe), stent angulation, and stent migration (the silicone stent forms an angle with the airway under bronchoscope, shown in Figure S1).
Statistical analysis
The unpaired t-test, chi-square test, and logistic regression model were used to analyze the differences in the related indicators of efficacy, duration of stent placement, and the number of bronchoscopic interventions. As age, duration of stent placement, and number of bronchoscopic interventions were continuous variables, the medians were used to classify them as categorical variables, after which they were included in logistic regression analysis. The X-tile software (YSM, New Haven, CT, USA) was used to determine the optimal cutoff value of stent placement duration. The relationship between duration of stent placement and efficacy was examined using the log-rank test. All statistical analyses were performed using SPSS version 25 (IBM Corp., Armonk, NY, USA). An alpha value of < 0.05 was considered statistically significant.
Results
Patient characteristics
Of 352 patients with benign airway stenosis treated by silicone stents during the study period, 99 were treated with a Dumon stent and met the inclusion criteria. Forty-two patients (42.4%) were male and 57 (57.6%) were female. The mean age was 40.9 ± 14.9 years (range, 15–70). Fifty-seven patients (57.6%) had PTBS, 17 (17.2%) had PTTS, 16 (16.2%) had PITS, and 9 (9.1%) had other types of stenosis.
The stenotic segment was located in the left main bronchus in 43 patients (43.4%), the trachea in 44 (44.4%), and the right main bronchus in 12 (12.1%). The median duration of stent placement was 15.5 months. The median follow-up duration after stent removal was 22 months (range, 6–53.47) (Table 1).
Baseline characteristics of patients.

Data are n/N (%), mean ± SD, median (range). N is the total number of patients with available data. Percentage is the proportion of the total number of people.
BD, bronchial stent; CB, carina-bronchus stent; PITS, post-intubation tracheal stenosis; PTBS, post-tuberculosis bronchial stenosis; PTTS, post-tracheotomy tracheal stenosis; SD, standard deviation; ST, hourglass stent; TD, standard tracheal stent; Y, bifurcation stent.
Outcomes
Overall efficacy and complications
The overall cure rate was 60.6%. Efficacy was analyzed according to type and site of stenosis (Table 2). The cure rate was markedly lower for PTBS than for other types of stenosis (50.9% versus 73.8%, p = 0.021) and for stenosis of the left main bronchus than for stenosis at other sites (46.5% versus 71.4%, p = 0.012). A comparison of the baseline patient characteristics according to whether the stenosis was in the left main bronchus or at another site and according to whether the stenosis was PTBS or non-PTBS is provided in the Supplementary materials (Tables S1–S2).
The total efficacy of different classification.
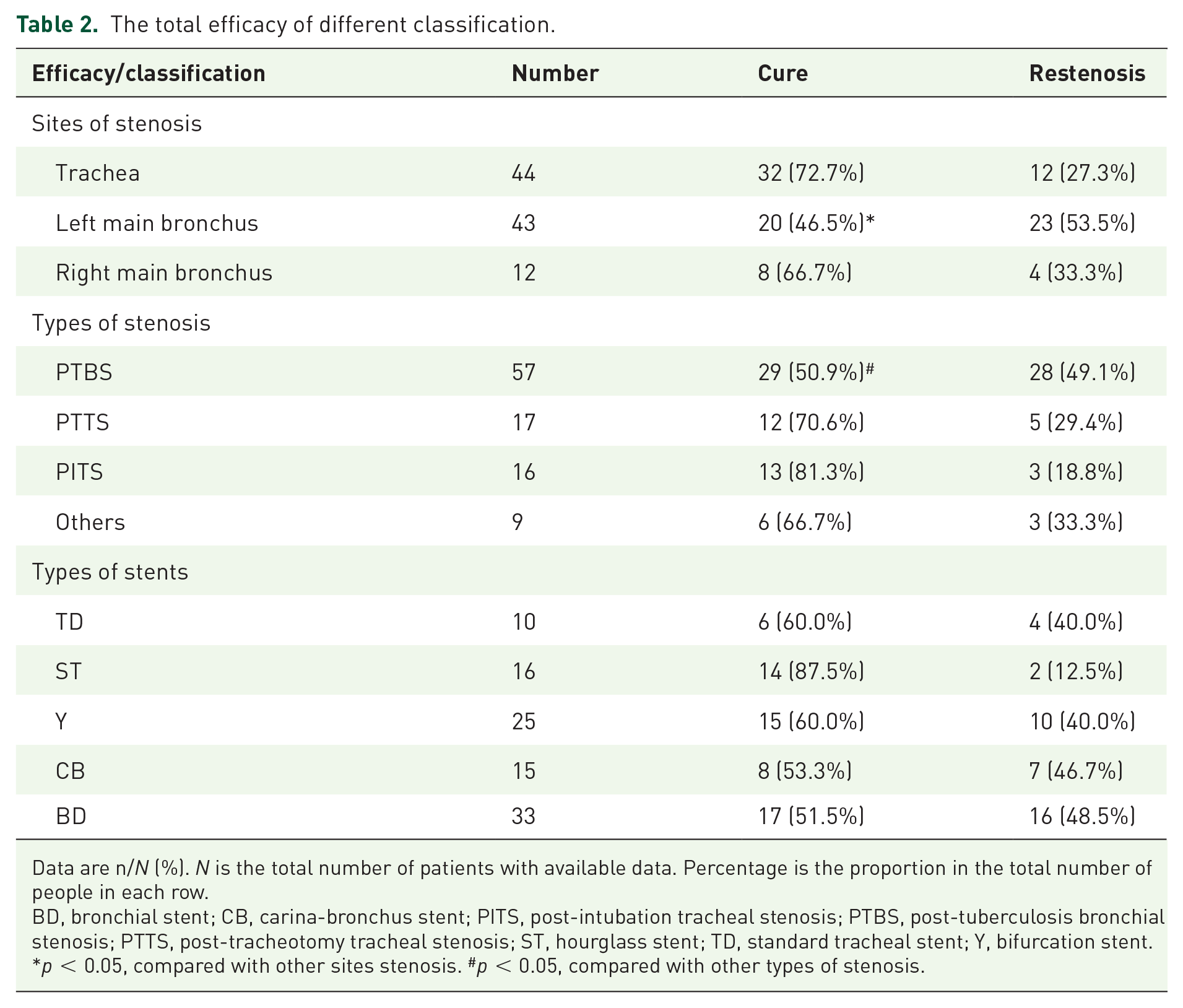
Data are n/N (%). N is the total number of patients with available data. Percentage is the proportion in the total number of people in each row.
BD, bronchial stent; CB, carina-bronchus stent; PITS, post-intubation tracheal stenosis; PTBS, post-tuberculosis bronchial stenosis; PTTS, post-tracheotomy tracheal stenosis; ST, hourglass stent; TD, standard tracheal stent; Y, bifurcation stent.
p < 0.05, compared with other sites stenosis. #p < 0.05, compared with other types of stenosis.
Stent replacement occurred in 22 patients due to the granulation hyperplasia (17 patients) and migration (5 patients) of the stents in the 6th and 2.6th months. Stent-related complications included secretion retention (70.7%), granuloma formation (67.7%), stent migration (12.1%), and stent angulation (21.2%). The total complication rate was 91.9%, and there were no stent-related deaths.
Factors influencing efficacy
Univariate analysis using the t-test and chi-square test showed that long-term efficacy was associated with age, granuloma formation, site and type of stenosis, duration of stent placement, the Charlson Comorbidity Index (CCI) grading, number of bronchoscopic interventions every 6 months during stent placement (stent-intervention number), and number of bronchoscopic interventions before stent placement. Variables with a p value < 0.10 in univariate analysis were included in multivariate logistic regression analysis. In multivariate logistic regression analysis, only duration of stent placement and stent-intervention number were independently associated with long-term efficacy. Patients with stent placement for longer than 13 months (odds ratio 3.317, 95% confidence interval 1.187–9.266, p = 0.022) and stent-intervention number ⩽ 1 (odds ratio 0.3, 95% confidence interval 0.107–0.839, p = 0.022) had a higher probability of cure after stent removal (Table 3).
Univariate and multivariate logistic regression for long-term efficacy of the Dumon stents in benign airway stenosis.

CCI, Charlson Comorbidity Index; CI, confidence interval; OR, odds ratio; PTBS, post-intubation tracheal stenosis; ST, hourglass stent; stent-intervention number, number of bronchoscopic interventions every 6 months during stent placement; TD, standard tracheal stent; Y, bifurcation stent.
Subgroup analysis
Duration of stent placement
Given that duration of stent placement was a major determinant of efficacy, we analyzed this relationship further. First, we determined the optimal cutoff value of stent placement duration was 13.1 months using the X-tile analysis (Figure 2), which suggested that perhaps patients could benefit the most when the stent was placed for 13.1 months. Then, using the optimal cutoff value of 13 months, the samples were divided into long-duration and short-duration stent placement groups. The restenosis rate was found to be significantly lower in the long-duration group than in the short-duration group (24.6% versus 63.2%, p < 0.001), and the long-duration group derived more effective than the short-duration group (p = 0.001, log-rank test; Figure 3). Compared with the short-duration group, the long-duration group had lower incidence of granuloma formation (84.2% versus 57.4%, p = 0.006). There was no significant between-group difference in incidence of secretion retention, stent migration, or stent angulation.

The optimal cutoff value of stent placement duration identified by X-tile analysis.

The stent placement duration, 13 months, was used to divide samples into a long-duration stent placement group and a short-duration stent placement group. The free-relapse survival curve showing the free-relapse rate between a long placement time group and a short placement time group. The long-rank test were conducted (p = 0.001).
Number of stent interventions
The relationship between stent-intervention number and efficacy was examined. The cure rate was found to be significantly higher when the number of stent interventions was ⩽ 1 than when it was > 1 (80% versus 36.4%, p < 0.001). In terms of stent-related complications, the incidence of granuloma formation was significantly higher when the stent-intervention number was > 1 than when it was ⩽ 1 (93.2% versus 47.3%, p < 0.001); however, there was no apparent between-group difference in the rate of secretion retention, stent migration, or stent angulation.
Discussion
In this study, the Dumon stent had moderate long-term efficacy and safety in the treatment of benign airway stenosis. Patients with stenosis in the left main bronchus were more prone to restenosis. Duration of stent placement, the stent-interventions number, and a CCI score were found to be major determinants of long-term efficacy. Patients in whom the Dumon stent is placed for longer than 13 months may derive the most benefit. To the best of our knowledge, this is the first study to assess the long-term efficacy and safety of silicone stents when used to treat benign airway stenosis in detail and in such a large sample size. This study is also the first to identify that the efficacy of the Dumon stent may be affected by the site of stenosis. Our findings could be helpful in terms of decision-making regarding the clinical treatment of benign airway stenosis and stent removal.
Silicone stents have been widely used to treat benign airway stenosis, but the timing of removal and their long-term efficacy thereafter have been unclear. Previous studies have found that these stents have a long-term efficacy rate in the range of 50.0%–85.7%.7–10,13 In our present study, 60.6% of patients with airway stenosis were treated successfully with no restenosis after stent removal. We also determined that patients with PTBS or left main bronchus stenosis derived less benefit. The incidence of stent-related complications was higher in our patients than in the previous studies.8,14,15 Our findings deviated from previous studies, we considered the following reasons. First, endobronchial tuberculosis probably was the main cause of poor efficacy and the high incidence of complications. PTBS is the most common type of benign airway stenosis in China, and the left main bronchus is particularly vulnerable to tuberculosis. 1 Our study showed that in the cases of stenosis in the left main bronchus, 95.35% of cases were caused by tuberculosis, which may be one of the reasons why the efficacy of the left was not obvious. Local infection with Mycobacterium tuberculosis may increase the tendency to produce thick secretions and granulation formation. We observed that among all patients with stent-related complications, about 56.6% of these complications occurred in patients with PTBS. Lim et al. observed that 64.8% of patients in whom a silicone stent was placed for PTBS developed granulomatous hyperplasia. 16 Accordingly, to improve the efficacy of silicone stent placement in the left main bronchus or in patients with PTBS, it is necessary to combine anti-tuberculosis therapy with regular bronchoscopic examination. 17 Second, another one that probably affected the efficacy and complications perhaps was the stent placement duration. We observed that patients with longer stent placement duration had significantly lower restenosis rate and a higher incidence of granuloma formation. Prolonging the duration of stent placement is beneficial to repair the damage of airway mucosa and obtain a stable stenotic segment. Few studies have shown that patients with a relatively longer stent placement duration performed better. 18 However, prolonged stent placement was accomplished with long and persisting irritation of the airway wall, which may have induced granulation hyperplasia. Freitas’s study supported this view and reported that the frequency of stent-related complications was associated with the stent placement duration (p < 0.001). Finally, on account of Dumon stent implantation, the thick stent wall and impairment of ciliary movement further aggravated the incidence of complication.19,20 Due to the high incidence of complications, patients still require regular follow-up after stent placement.
A proportion of patients still relapse after stent removal. Accordingly, it is important to focus on risk factors associated with restenosis after stent removal. Our study determined that stent placement for longer than 13 months was an important determinant of a favorable outcome after stent removal. It is widely recommended that a silicone stent be placed for 6–18 months.8,21,22 A too long or too short duration of stent placement would not facilitate treatment of stenosis. The timing of stent removal is still controversial. Eom et al. suggested that the silicone stent should be removed after the mucosal trauma in the narrowed segment of the airway has completely recovered, which may take at least 12 months. 18 Furthermore, Verma et al. pointed out that the length of air pockets seen on computed tomography scan can help to guide the timing of stent removal, having found that patients with a stent placed for 16 months had a better curative effect and that their air pockets were longer. 11 In our study, patients with a stent dwell time of more than 13 months derived significantly more benefit with a lower risk of granuloma formation, which implies that a prolonged stent dwell time could make it easier to obtain a stable stenotic segment. Therefore, placement of a silicone stent for longer than 13 months was probably a protective factor. However, further research is needed regarding the indications for stent removal.
Another prognostic factor in our study was the stent-intervention number ⩽ 1. Granuloma formation was more likely in patients who underwent more than once stent intervention within 6 months. The fewer the number of complications that occur, the fewer the number of bronchoscopic interventions that are required, 16 and this suggests an opportunity to remove the stent if it has stabilized the airway for more than 6 months. It may be possible to selectively remove a silicone stent that has had a dwell time of more than 13 months and the stenotic airway has remained stable during at least 6 months of follow-up.
This study has several limitations. First, it had a retrospective design and included participants from a single institution in China. Therefore, multicenter prospective trials are needed to confirm our findings. Second, PTBS was the predominant type of stenosis, so our findings may not be generalizable to all types of airway stenosis. Third, we analyzed data for different types of stent, which may have introduced a degree of bias in terms of the results for a single type of silicone stent. However, despite these limitations, our results should provide some guidance regarding use of silicone stents for benign airway stenosis.
Conclusion
The Dumon stent has moderate efficacy and safety in the treatment of benign airway stenosis but needs further improvement. The stent was least effective in patients with stenosis in the left main bronchus. Moreover, patients with a stent placed for more than 13 months or a stent-intervention number of ⩽ 1 may have a favorable prognosis. If a silicone stent has a dwell time of 13 months and the stenotic segment remains stable for more than 6 months, consideration could be given to its removal. Stent placement for more than 13 months, and a stent-intervention number of ⩽ 1 predicted a favorable outcome.
Supplemental Material
sj-docx-1-tar-10.1177_17534666231181269 – Supplemental material for Long-term efficacy and safety of the Dumon stent for treatment of benign airway stenosis
Supplemental material, sj-docx-1-tar-10.1177_17534666231181269 for Long-term efficacy and safety of the Dumon stent for treatment of benign airway stenosis by Li-Qin Lin, Di-Fei Chen, Hong-Kai Wu, Yu Chen, Chang-Hao Zhong, Xiao-Bo Chen, Chun-Li Tang, Zi-Qing Zhou and Shi-Yue Li in Therapeutic Advances in Respiratory Disease
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.