
Abstract
Background:
N-acetylcysteine (NAC) may reduce acute exacerbations of chronic obstructive pulmonary disease through an antioxidant effect. Due to the heterogeneity in studies, the currently available data do not confirm the efficacy of oral NAC therapy in chronic obstructive pulmonary disease patients. We hypothesize that chronic obstructive pulmonary disease patients receiving regular oral NAC therapy do not achieve improved clinical outcomes.
Objectives:
The purpose of this meta-analysis was to determine the efficacy of long-term oral NAC therapy in chronic obstructive pulmonary disease patients.
Data sources and methods:
The literature search was performed using the PubMed, Web of Science, and Cochrane Library databases to identify all included clinical studies. Studies were eligible for inclusion only if they directly compared the outcomes of NAC versus placebo in adults with chronic obstructive pulmonary disease between 1 January 2000 and 30 May 2022. All studies were included if they reported one or more of the following outcomes: number of patients with no acute exacerbations, forced expiratory volume in 1 s (FEV1), forced vital capacity (FVC), St George’s Respiratory Questionnaire score, glutathione level, and adverse events.
Results:
Nine randomized controlled trials were included in the meta-analysis. There were 1061 patients in the NAC group and 1076 patients in the placebo group. The current meta-analysis provides evidence that the number of patients with no acute exacerbations (965 patients receiving NAC therapy, 979 control group patients), change in FEV1 (433 patients receiving NAC therapy, 447 control group patients), change in FVC (177 patients receiving NAC therapy, 180 control group patients), change in St George’s Respiratory Questionnaire score (128 patients receiving NAC therapy, 131 control group patients), change in glutathione levels (38 patients receiving NAC therapy, 40 control group patients), and adverse events (832 patients receiving NAC therapy, 846 control group patients) were not significantly different between the two groups.
Conclusion:
NAC did not reduce the risk of acute exacerbation or ameliorate the decline in lung volume in chronic obstructive pulmonary disease patients.
Keywords
Introduction
Chronic obstructive pulmonary disease (COPD) is a chronic and treatable disease. It is characterized by persistent airflow limitation, mucus hypersecretion, and shortness of breath. COPD patients may suffer from aggravated clinical symptoms with an increase in the amount and/or purulence of sputum and dyspnea. An episode of acute worsening of clinical symptoms is called acute exacerbation. Acute exacerbation of COPD (AECOPD) leads to disease progression, accelerated lung function deterioration, damage to health, and increased mortality.
N-acetylcysteine (NAC) is an effective mucolytic drug that decreases sputum viscosity and elasticity and improves low airway mucociliary clearance. In addition, NAC has antioxidant and anti-inflammatory properties. Glutathione (GSH) has important roles in cellular defense against cellular oxidant aggression. Oral NAC undergoes first-pass effects resulting in most of it being taken up by the liver, thus an effective treatment when hepatic GSH levels are depleted with acetaminophen poisoning. GSH levels are increased in the bronchoalveolar lavage fluid of stable COPD patients and are decreased during exacerbations. Excessive production of reactive oxygen species during COPD exacerbation results in reduced GSH levels. NAC acts as a precursor for the substrate cysteine in the synthesis of GSH, and oral NAC enhances the synthesis of GSH. Increased levels of GSH in the lung might improve clinical outcomes by suppressing oxidant-induced inflammation.1–5 NAC may be able to reduce acute exacerbations of COPD through an antioxidant effect. However, NAC is a weaker antioxidant, and a high dosage of NAC (⩾1200 mg per day) is required for antioxidant activity in COPD patients to reduce the risk of exacerbations.6–8 Poole et al. 9 showed that oral mucolytic agents (including NAC, carbocysteine, erdocysteine, ambroxol, etc.) may produce a small reduction in acute exacerbations in COPD patients. Such treatments were shown to be beneficial in published articles before 2000. In 2005, the Bronchitis Randomized on NAC Cost-Utility Study failed to demonstrate a beneficial effect of NAC on exacerbation frequency. 10 Zheng et al. 11 showed that Chinese patients with moderate-to-severe COPD receiving long-term NAC 600 mg treatment twice daily can exhibit a reduction in the risk of exacerbations. Due to heterogeneity of the studied populations, treatment NAC dose, duration of therapy period, and concomitant COPD treatments, the currently available data do not confirm the efficacy of regular oral NAC therapy on COPD patients, especially regarding acute exacerbation. We hypothesize that COPD patients receiving regular oral NAC therapy do not achieve improvements in clinical outcomes, such as acute exacerbation and amelioration of the decline in lung volume, St George’s Respiratory Questionnaire (SGRQ) scores, and GSH levels. The purpose of this meta-analysis was to determine the efficacy of long-term regular oral NAC therapy in COPD patients. We included only studies published after 2000 in the current meta-analysis.
Methods
Data search strategy
The literature search was performed using the PubMed, Web of Science, and Cochrane Library databases to identify all included clinical studies and meta-analyses or systematic reviews on the topic from 1 January 2000. In the databases, we used the following search string: ‘(N-acetylcysteine OR Acetylcysteine) AND (chronic obstructive pulmonary disease OR COPD OR pulmonary emphysema OR chronic bronchitis)’. We examined treatment studies that directly compared the outcomes of oral NAC versus placebo in adults with COPD and searched relevant articles published from inception to 31 May 2022. We included only randomized controlled trials. Previously published systematic reviews and meta-analyses were reviewed to identify any additional studies that may have been missed in the primary literature search. No language restrictions were imposed.
Study selection and data extraction
To determine the eligibility of the identified trial reports, each study was independently screened and reviewed by two authors. After excluding duplicates, two authors screened the titles and abstracts of all studies retrieved to identify eligible records. After excluding irrelevant studies, all of the relevant articles were reviewed by reading the full texts to determine eligibility. Data regarding the author, year of publication, country, total number of patients receiving NAC, total number of patients receiving placebo, NAC dosage, duration of therapy, total number of patients with no acute exacerbations during study period, the volume of change in forced expiratory volume in 1 s (FEV1) before and after the study, the volume of change in forced vital capacity (FVC) before and after the study, the change in SGRQ score before and after the study, the change in GSH activity before and after the study, and adverse events were extracted from the eligible full-text articles. Any disagreement was subsequently resolved with the consensus of the review team and discussion with a third author.
Inclusion and exclusion criteria
The studies were considered eligible for inclusion only if they directly compared the outcomes of NAC versus placebo in adults with COPD. Oral NAC was administered at dosages ranging from 600 mg every 24 h to 1800 mg every 12 h. All studies were included if they reported one or more of the following outcomes: number of patients with no acute exacerbation during the study period, change in FEV1 volume in liters before and after the study, change in FVC volume in liters before and after the study, change in SGSR score before and after the study, change in GSH level before and after the study, and adverse events.
Definitions and outcomes
The primary outcome was the total number of patients with no acute exacerbations during the study period. Acute exacerbation was defined as an acute worsening of respiratory symptoms that resulted in additional therapy. The secondary outcomes were change in FEV1 volume in liters before and after the study, change in FVC volume in liters before and after the study, change in SGSR score before and after the study, change in GSH level before and after the study, and adverse events. The adverse event data recorded were the risk of discontinuation due to adverse events and serious adverse events, including COPD-related adverse events, and some common events, such as diarrhea, nausea, headache, and constipation.
Quality assessment and statistical analysis
The methods of quality assessment of included studies and the statistical analysis of data are the same as previous studies. 12
Results
Characteristics of the included trials
The flow diagram in Figure 1 shows the details of the study selection process. The numbers of initial search results from PubMed, Web of Science, and the Cochrane Library were 245, 315, and 123, respectively. There were 293 duplicate studies. A total of 390 irrelevant studies were identified by reading the title and abstract. After the exclusion of duplicates and irrelevant studies, 46 potentially relevant studies remained. After full-text article review, 35 studies were excluded because they lacked results comparing the outcomes of NAC versus placebo in adults with COPD. Two studies were excluded because they were not randomized controlled trials (RCTs). Finally, nine studies were included in the meta-analysis.10,11,13–19 The main characteristics of the nine included studies are shown in Table 1. Four studies had a high risk of bias. The risk of bias assessment is presented in Figure 2.

Flow diagram of the study selection process.
Main characteristics of the included nine studies.
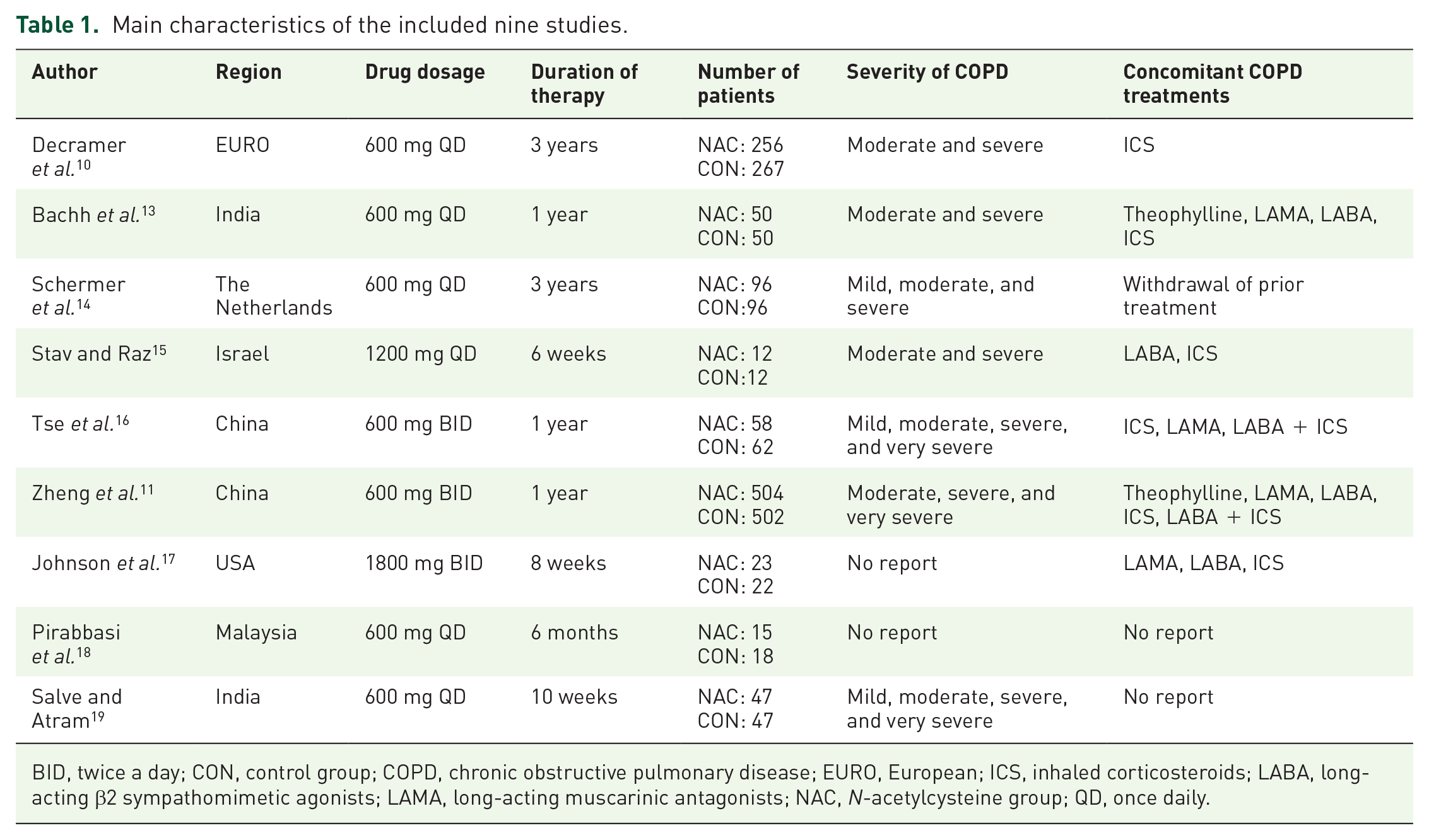
BID, twice a day; CON, control group; COPD, chronic obstructive pulmonary disease; EURO, European; ICS, inhaled corticosteroids; LABA, long-acting β2 sympathomimetic agonists; LAMA, long-acting muscarinic antagonists; NAC, N-acetylcysteine group; QD, once daily.

Risk of bias graph: review authors’ judgments about each risk of bias item presented as percentages across all included studies.
Efficacy and safety outcomes
There were 1061 patients in the receiving NAC group and 1076 patients in the placebo group. Six studies involving 1944 patients (965 patients receiving NAC therapy, 979 control group patients) reported the number of patients with no acute exacerbations.10,11,13,14,16,17 There was no statistically significant difference in the number of patients without acute exacerbations between the two groups [odds ratio (OR) = 1.12, 95% confidence interval (CI) = 0.92–1.36, p = 0.26, I2 = 51%] (Figure 3). Subgroup analysis of the NAC dosage (⩾1200 mg per day and <1200 mg per day) was performed, and the results are shown in Figure 4. There was no statistically significant difference in the number of patients without acute exacerbations related to NAC dosage. Four studies involving 880 patients (433 patients receiving NAC therapy, 447 control group patients) reported the change in FEV1 volume in liters before and after the study.10,14,16,17 There was no statistically significant difference in the FEV1 between the two groups (mean difference = 0.00, 95% CI = −0.01 to 0.00, p = 0.29, I2 = 90%) (Figure 5). Three studies involving 357 patients (177 patients receiving NAC therapy, 180 control group patients) reported change in FVC volume in liters before and after the study.14,16,17 There was no statistically significant difference in FVC between the two groups (mean difference = 0.04, 95% CI = −0.03 to 0.11, p = 0.28, I2 = 97%) (Figure 6). Three studies involving 259 patients (128 patients receiving NAC therapy, 131 control group patients) reported change in SGRQ scores before and after the study.16,17,19 There was no statistically significant difference in the SGRQ score between the two groups (mean difference = 1.08, 95% CI = −5.04 to 7.19, p = 0.73, I2 = 94%) (Figure 7). Two studies involving 78 patients (38 patients receiving NAC therapy, 40 control group patients) reported change in GSH levels (µM) before and after the study.17,18 There was no statistically significant difference in the GSH level between the two groups (mean difference = 0.14, 95% CI = −0.13 to 0.40, p = 0.32, I2 = 0%) (Figure 8). Four studies involving 1687 patients (832 patients receiving NAC therapy, 846 control group patients) reported adverse events (including COPD-related adverse events).10,11,16,17 There was no statistically significant difference in adverse events between the two groups (OR = 1.21, 95% CI = 0.97–1.51, p = 0.10, I2 = 0%) (Figure 9). Nausea, diarrhea, COPD symptoms, dry month, muscle pain, leg edema, nausea, headache, and dizziness were commonly reported adverse events in NAC treatment patients.

Forest plots for no exacerbation patients between the N-acetylcysteine therapy group and the control group.

Forest plots for no exacerbation patients between the N-acetylcysteine (NAC) therapy group and the control group (subgroup analysis of the N-acetylcysteine dosage ⩾ 1200 mg per day and < 1200 mg per day).

Forest plots for FEV1 between the N-acetylcysteine therapy group and the control group.

Forest plots for FVC between the N-acetylcysteine therapy group and the control group.

Forest plots for SGRQ score between the N-acetylcysteine therapy group and the control group.

Forest plots for GSH level (µM) between the N-acetylcysteine therapy group and the control group.

Forest plots for adverse events between the N-acetylcysteine therapy group and the control group.
Discussion
The current meta-analysis of nine studies provides evidence that the number of patients with no acute exacerbations, change in FEV1, change in FVC, change in SGRQ score, change in GSH level, and adverse events were not significantly different between patients receiving NAC and patients receiving placebo. NAC could not reduce the risk of acute exacerbation and ameliorate the decline in lung volume in COPD patients. Six meta-analyses published before 2020 explored the efficacy of NAC on the exacerbation of COPD.20–25 All six meta-analyses concluded that long-term oral NAC could reduce the risk of exacerbation of COPD. Five meta-analyses included studies published mainly before 2000.20,21,23–25 In the meta-analysis of Cazzola et al., 22 only high-dose NAC (1200 mg/day) could prevent exacerbation of COPD, but this conclusion was cited from only two studies. Pharmacological therapy for COPD is used to reduce symptoms, reduce the frequency and severity of exacerbations, improve exercise tolerance, and decrease mortality. Pharmacological therapy for COPD may have the potential benefit of reducing the rate of decline in lung function. The mainstay of pharmacological therapy for COPD is inhaled bronchodilators, which can increase patients’ lung volume. Bronchodilator medications for COPD are most often administered as long-term regular inhalation therapy. A clinical trial showed that long-acting muscarinic antagonists (LAMA) can reduce the frequency of acute exacerbation.26,27 Long-acting dual bronchodilators have been recommended in the Global Initiative for Chronic Obstructive Lung Disease (GOLD) guide for approximately 10 years. Clinical trials have shown that dual bronchodilator therapy can increase lung function and decrease the risk of acute exacerbations compared with monotherapy.28–30 Inhaled corticosteroids (ICS) in combination with long-acting bronchodilator therapy can improve lung function and reduce exacerbation. Moreover, ICS in combination with long-acting bronchodilator therapy is more effective than either component alone.31,32 Triple inhaled therapy (dual bronchodilators and ICS), which has been recommended in the GOLD guide since 2019 for selected COPD patients, can improve lung function and reduce exacerbations compared with LAMA, dual bronchodilators, or LABA/ICS.33–37 Regular long-term inhaled therapy for COPD significantly reduces respiratory symptoms, the frequency of exacerbations, and the risk of mortality and is a well-documented therapy for COPD patients. Pharmacological inhalation therapy for COPD has greatly improved since 2000. Therefore, we included studies published after 2000 in the current meta-analysis and showed that NAC could not reduce the risk of acute exacerbation. The GOLD guidelines concluded that NAC may reduce exacerbations in COPD patients not taking ICS.22,38 Shermer et al. showed different research results. There was no statistically significant reduction in the exacerbation risk in COPD among patients receiving NAC, patients receiving placebo, and patients receiving fluticasone inhalation. 14 In the meta-analysis of Jiang et al., NAC was shown to improve the rate of acute exacerbation, improve lung function (FEV1 and FEV1/FVC), and increase glutathione sulfur transferase activity. The meta-analysis included 15 studies. 39 We read the full texts of 15 studies and found that 13 studies did not report the efficacy of NAC in the treatment of COPD patients with exacerbations.40–52 We are thus uncertain about how the meta-analysis can draw such conclusions.
Regarding lung volume, only two previous meta-analyses explored the issue and showed that COPD patients taking NAC did not have altered lung volume.20,22 NAC is not a bronchodilator and therefore should not improve lung function or ameliorate the decline in lung volume in COPD patients. Regarding the SGRQ score, NAC cannot reduce the risk of exacerbations and improve lung function. COPD patients cannot achieve significant improvement in clinical symptoms and signs. Therefore, an increased SGRQ score cannot be achieved. Regarding GSH levels, there was no statistically significant increase in GSH levels after regular oral NAC treatment of COPD patients in the current meta-analysis. However, we cited only two studies in the current meta-analysis, and there was little evidence.17,19
The study by Buha et al. 53 evaluated the efficacy of propolis and NAC in exacerbations of COPD. In vitro studies show that propolis has anti-inflammatory, immunomodulatory, antioxidative, anti-infectious, and antiproliferative properties.54,55 The study population consisted of only 46 patients, and it was found that the oral combination of natural propolis with NAC significantly reduced the AECOPD incidence rate. The results need to be confirmed by large RCT trials. 53 The prospective observational study of Ansari et al. explored the role of oral NAC in the management of AECOPD. The study included only 40 patients, and the results revealed that there was a significant improvement in the mean partial pressures of oxygen and carbon dioxide on day 7 in the NAC group compared with the placebo group. The author concluded that regular oral 600 mg twice daily of NAC for AECOPD may have beneficial outcomes (not a reduced frequency of AECOPD). 56 Were these beneficial outcomes related to mucolytic effects or antioxidant effects? The study by Zhang et al. explored the efficacy of NAC for COPD and chronic bronchitis. The study concluded that there was no significant difference in SGQR scores between the placebo and NAC groups. 57 The results were compatible with the result of the current meta-analysis.
The current meta-analysis showed that regular oral NAC was an adjuvant therapy for COPD. The main effect of oral NAC in COPD therapy is mucolysis. NAC could not reduce the risk of acute exacerbation or ameliorate the decline in lung volume in COPD patients.
Limitations
Few RCTs have explored this issue since 2000. Four of the included studies had a high risk of bias in the current meta-analysis. The number of included studies and the population sizes were small, which is another limitation of this meta-analysis. The nine studies in the current meta-analysis had heterogeneous study designs, including NAC treatment dose, duration of therapy, and concomitant COPD treatment. In addition, there are several types of reports about exacerbations, such as exacerbation frequency, exacerbation rate, number of exacerbations per year, number of patients with at least one exacerbation, and number of patients with no exacerbations. Is there a synergistic effect for COPD patients between regular oral high-dose NAC (⩾1200 mg/day) and inhaled therapy with long-acting bronchodilators to prevent disease exacerbations? Medical experts need to perform further RCTs to confirm the issue.
Conclusion
The current meta-analysis provided evidence that the number of patients with no acute exacerbations, change in FEV1, change in FVC, change in SGRQ score, and change in GSH level were not significantly different between patients receiving NAC and patients receiving placebo. NAC could not reduce the risk of acute exacerbation and ameliorate the decline in lung volume in COPD patients. Regular long-term inhaled therapy with long-acting bronchodilators significantly reduces respiratory symptoms, the frequency of exacerbations, and the risk of mortality in COPD patients.