
Abstract
Background:
Evidence suggests differences in ventilation efficiency and respiratory mechanics between early COVID-19 pneumonia and classical acute respiratory distress syndrome (ARDS), as measured by established ventilatory indexes, such as the ventilatory ratio (VR; a surrogate of the pulmonary dead-space fraction) or mechanical power (MP; affected, e.g., by changes in lung-thorax compliance).
Objectives:
The aim of this study was to evaluate VR and MP in the late stages of the disease when patients are ready to be liberated from the ventilator after recovering from COVID-19 pneumonia compared to respiratory failures of other etiologies.
Design:
A retrospective observational cohort study of 249 prolonged mechanically ventilated, tracheotomized patients with and without COVID-19-related respiratory failure.
Methods:
We analyzed each group’s VR and MP distributions and trajectories [repeated-measures analysis of variance (ANOVA)] during weaning. Secondary outcomes included weaning failure rates between groups and the ability of VR and MP to predict weaning outcomes (using logistic regression models).
Results:
The analysis compared 53 COVID-19 cases with a heterogeneous group of 196 non-COVID-19 subjects. VR and MP decreased across both groups during weaning. COVID-19 patients demonstrated higher values for both indexes throughout weaning: median VR 1.54 versus 1.27 (p < 0.01) and MP 26.0 versus 21.3 Joule/min (p < 0.01) at the start of weaning, and median VR 1.38 versus 1.24 (p < 0.01) and MP 24.2 versus 20.1 Joule/min (p < 0.01) at weaning completion. According to the multivariable analysis, VR was not independently associated with weaning outcomes, and the ability of MP to predict weaning failure or success varied with lung-thorax compliance, with COVID-19 patients demonstrating consistently higher dynamic compliance along with significantly fewer weaning failures (9% versus 30%, p < 0.01).
Conclusion:
COVID-19 patients differed considerably in ventilation efficiency and respiratory mechanics among prolonged ventilated individuals, demonstrating significantly higher VRs and MP. The differences in MP were linked with higher lung-thorax compliance in COVID-19 patients, possibly contributing to the lower rate of weaning failures observed.
Introduction
Before the implementation of nationwide vaccination programs and the emergence of the Omicron variant in 2021, COVID-19-related hospitalizations resulted in approximately 14% of subjects being treated in the intensive care unit due to severe respiratory failure, 1 with up to 90% ultimately receiving invasive mechanical ventilation.2,3 These patients consistently met the Berlin criteria for COVID-19-related acute respiratory distress syndrome (CARDS),2,4 which is associated with mortality rates ranging between 30% and 80% depending on distinct patient-related factors.5,6
Early reports of CARDS revealed a different profile in ventilation efficiency and respiratory mechanics compared to the classical ARDS, typically presenting increased dead-space ventilation and well-preserved lung-thorax compliance in the early stages of the COVID-19 disease.7,8 Established ventilatory indexes readily accessible at the bedside can be used to evaluate both factors, such as the ventilatory ratio (VR) 9 and the mechanical power (MP) of artificial ventilation, the amount of energy per time unit transferred to the respiratory system. 10
VRs are simple surrogates for impaired ventilation efficiency that correlate well with the pulmonary dead-space fraction (VD/VT). 9 This index compares actual minute ventilation and associated PaCO2 during mechanical ventilation with the expected values, which are computed based on the predicted body weight to adjust for individual lung dimensions. It is a unitless ratio, and a value approximating one would represent normal ventilating lungs. In patients experiencing an increase in the pulmonary dead-space fraction, higher minute ventilation is required to maintain the same PaCO2 (this makes mechanical ventilation and spontaneous breathing less ‘efficient’), which will cause the VR to increase. In contrast, the MP concept was introduced to shed further light on the mechanisms involved in ventilator-induced lung injury, as it converges all ventilatory variables (e. g. respiratory rate, tidal volume, and airway pressures) deemed responsible. 10 Respiratory subphenotypes of CARDS predicting different prognoses have been identified based on these two indexes, 11 and upward trends in parameters following intubation have also been linked with a longer duration of mechanical ventilation.11,12
In addition to predicting mortality in CARDS13,14 and ARDS,15,16 VR and MP may also be used to determine patients’ spontaneous breathing ability during weaning from mechanical ventilation.17–19 Indeed, oxygenation and decarboxylation are closely related to the ventilatory variables used in VR and MP calculations. However, there are currently no studies evaluating these variables in the later stages of CARDS, when patients have recovered from respiratory failure and are ready to be liberated from the ventilator.
The study’s primary objective was to determine the VR and MP distributions and trajectories among prolonged mechanically ventilated patients following COVID-19 pneumonia compared to a large cohort of respiratory failures of other etiologies. Secondary outcomes included weaning failure rates between these groups and the ability of the VR and MP to predict weaning failure or success.
Materials and methods
We conducted a retrospective observational cohort study at a national weaning center, receiving referrals from intensive care units all over Germany since the onset of the pandemic. Project approval was granted by the local institutional review board for human studies (Ethics Committee of the State Chamber of Physicians of Baden-Württemberg, Germany, File No. F-2021–158) and was conducted according to the Declaration of Helsinki principles. As the analysis was retrospective, informed consent was waived. We adhered to STROBE guidelines for reporting observational studies. 20
Ventilator weaning procedure
Established in 2006, the 12-bed weaning unit annually treats approximately 80–100 prolonged mechanically ventilated patients with tracheostomies. Patients receive ventilatory support invasively (via tracheal cannulas or endotracheal tubes) and non-invasively (using non-invasive mask ventilation or nasal high-flow cannulas). The multidisciplinary team comprises pulmonologists, respiratory therapists, physiotherapists, speech-language pathologists, and psychologists. Nursing staff and physicians work in rotating shifts of 8 h. Nurse-to-patient ratios are 1:2 during the day and 1:3 at night.
On admission, all patients were ventilated in the pressure-controlled, assist-control (A/C) mode. As described previously, a standardized method of ventilator liberation was employed as soon as the criteria for weaning readiness were met.17,18 Per protocol, ventilator weaning always starts with a 30-min spontaneous breathing trial (SBT). These weaning trials are conducted once daily, typically extending the duration by 2–3 h per day, aiming at complete autonomic breathing.
Patient selection
Evaluation of consecutive COVID-19 patients with tracheostomies referred from intensive care units across Germany to our specialized weaning unit between March 2020 and June 2021. This cohort consists of patients from the first three waves of the pandemic. Subjects were included in the study if they met the prolonged weaning criteria, 21 classified as category 3 according to Boles and colleagues (e.g. failed at least three weaning attempts or required more than 7 days of weaning after the first SBT).
The Control group comprised tracheotomized patients with respiratory failure of other etiologies than COVID-19 leading to prolonged weaning, 21 treated at our center between October 2018 and June 2021. Based on statistical considerations, we have extended the observation period in this group to allow comparisons of COVID-19 with as many non-COVID-19 subjects as possible. Moreover, separate analyses of de novo type-1 (hypoxemic) respiratory failure patients (not related to COVID-19) were conducted to account for the heterogeneity of the Control group. De novo type-1 respiratory distress refers to hypoxemic respiratory failure resulting from pulmonary infiltrates rather than cardiac causes (e.g. cardiogenic pulmonary edema).
Analyses were limited to patients who completed the ventilator liberation process (either successfully or unsuccessfully) but excluded those who died during weaning (success or failure in ventilator liberation remained uncertain) or had neuromuscular diseases.
Data collection
Electronic medical records and charting systems were used to collect data (iMedOne, Telekom Healthcare Solutions, Bonn, Germany; PDMS Metavision ICU, iMDsoft, and Tel Aviv, Israel). Patients’ baseline characteristics, including demographics, clinical features, and comorbidities, were collected. Types of respiratory failure leading to prolonged ventilation were assessed and categorized into COVID-19 pneumonia versus de novo type-1 respiratory failure (other than COVID-19) and other respiratory failures (both represent the Control group).
Multiple measurements of ventilatory variables and arterial blood gas analysis were recorded at different time points in each patient: (1) immediately before the first SBT on admission (day 0, one-time measurement), (2) 48 h after the first SBT (days 1–2), and (3) 48 h before weaning completion (pre-completion), with the median of these parameters used for the analyses. Moreover, we evaluated arterial blood gas analyses during spontaneous breathing for up to 7 days following weaning completion to determine failure or success (see Supplementary file 1: Figure S1).
Ventilatory variables of interest
Pressure-controlled, assist-control (A/C) ventilation was used on all patients to unload the respiratory pump effectively during both an assisted and controlled breath, thereby minimizing respiratory muscle activity. Ventilatory variables collected included inspired oxygen fraction, respiratory rate, tidal volume (VT), peak inspiratory airway pressure (Pmax), and positive end-expiratory pressure (PEEP), with the following parameters calculated: ∆Paw (dynamic driving pressure, defined as Pmax – PEEP in the pressure-controlled ventilation mode), dynamic lung-thorax compliance (LTCdyn, defined as VT/∆Paw), 22 VR, 9 and MP 10 using the simplified formula proposed by Becher and colleagues. 23
To account for lung dimensions on which MP acts, referred to as ‘specific MP’, we normalized total power to LTCdyn (LTCdyn-MP), a measure of mechanical ventilation stress intensity. Dynamic compliance with its temporal changes is a surrogate of actual ventilated lung volume, accounting for the force required to overcome the respiratory system’s resistance and elastance (equals the dynamic driving pressure), which is crucial during ventilator weaning.17,18 In creating the Power indexrs,17,18 isocapnia was simulated by adjusting LTCdyn-MP values for complementary PaCO2 to account for individual ventilator settings. A detailed description of the calculated variables and indexes is provided in the online supplement (see Supplementary file 1).
Classification of outcomes
At the end of the ventilator weaning process, patients were categorized into two groups based on spontaneous breathing abilities determining weaning failure or success. Weaning failure is defined as a transition to domiciliary ventilation (by face mask or tracheostomy tube) due to chronic ventilatory failure. Ventilatory failure describes recurrent hypercapnia during daily weaning trials (observed on at least two consecutive days), preventing the extension of spontaneous breathing, or sustained hypercapnia (on at least two successive occasions) occurring within 7 days after weaning completion (requiring reinstitution of mechanical ventilation). These patients remain mechanically ventilated at discharge. As such, the definition of successful weaning is sustained spontaneous breathing (⩾ 7 days) without concomitant signs of ventilatory failure after weaning completion (median PaCO2 ⩽ 45.0 mmHg derived from the highest measured PaCO2 on each of the 7 days), determined by the last day on which the patient was ventilated. 17 These patients remain ventilator-detached on discharge.
Statistical analysis
Descriptive and frequency statistics summarized patients’ baseline demographics, clinical characteristics, and comorbidities. A chi-square or Fisher’s exact test was used when comparing categorical variables, as appropriate. Depending on the continuous variables’ homogeneity of variance, determined by the Kolmogorov–Smirnov normality test, differences between groups were analyzed through Student’s t-test or Mann–Whitney U test. Similarly, we performed bivariate comparisons of weaning outcomes in patients with and without COVID-19.
In the first step of the analysis, we calculated each group’s VR and MP distributions at different time points, as illustrated by Box-Whiskers plots. In the following step, we conducted a (factorial) repeated-measures analysis of variance (ANOVA) to detect within-subject time effects and between-group differences in ventilatory variables’ trajectories.
Next, we performed uni- and multivariate binary logistic regression analysis to identify factors (including VR and MP) independently associated with prolonged weaning failure in the entire study population. The following pre-specified variables deemed relevant regarding ventilator weaning were included: age, gender, body mass index (BMI), APACHE-II score, Charlson comorbidity index, presence of chronic heart failure or chronic obstructive pulmonary disease (COPD), COVID-19 pneumonia, and the ventilatory parameters of interest (the median of the VR, MP, and the Power indexrs [specific MP] assessed on days 1–2). 17 We performed a forward selection of variables, with Hosmer & Lemeshow test and Nagelkerke R 2 employed to evaluate the model’s goodness-of-fit. Forest plots were used to describe the effect sizes graphically, and we reported odds ratios with 95% confidence intervals (95% CI). Finally, we plotted Kaplan–Meier survival curves for each multivariable model’s factor, compared by log-rank test. Thresholds for continuous model variables were determined through receiver operating characteristic (ROC) curve analysis, using the criterion associated with the Youden index. 24
Since there were no comparable studies on prolonged mechanically ventilated COVID-19 patients to determine sample size, we compared subjects of the first three pandemic waves to a large, heterogeneous non-COVID-19 cohort, including the subgroup of patients with de novo type-1 respiratory failure. We performed two-tailed tests; statistical significance was indicated by p < 0.05. The analyses were conducted with MedCalc version 19.2.5. (MedCalc Software Ltd, Ostend, Belgium).
Results
The study included 249 out of 256 (97%) consecutively screened patients admitted to our center from October 2018 to June 2021. Four died during weaning (caused mainly by nosocomial pneumonia and ischemic heart disease), while three had neuromuscular diseases (Figure 1).

Patient flow diagram.
Baseline clinical characteristics
We analyzed 53 patients on prolonged mechanical ventilation following an ARDS associated with laboratory-confirmed COVID-19 pneumonia (positive PCR for SARS-CoV-2 virus). They presented the following characteristics: dexamethasone was administered to 42 patients (79%) and remdesivir to 3 patients (6%). Most (87%) had non-invasive respiratory support before intubation (nasal high-flow cannula and non-invasive ventilation), 43 (81%) experienced prone positioning during invasive ventilation in intensive care, and 8 (15%) were treated with venovenous extracorporeal membrane oxygenation.
On admission to the weaning center, patients with COVID-19 were younger and had lower APACHE-II scores and Charlson comorbidity indexes, associated with a lower proportion of patients with COPD and cardiac diseases (Table 1). By contrast, comparing COVID-19 with the de novo type-1 respiratory failure subgroup did not reveal significant differences in clinical characteristics and comorbidities (see Supplementary file 1: Table S1).
Clinical characteristics on admission to the weaning center – comparison of patients with and without COVID-19 pneumonia.
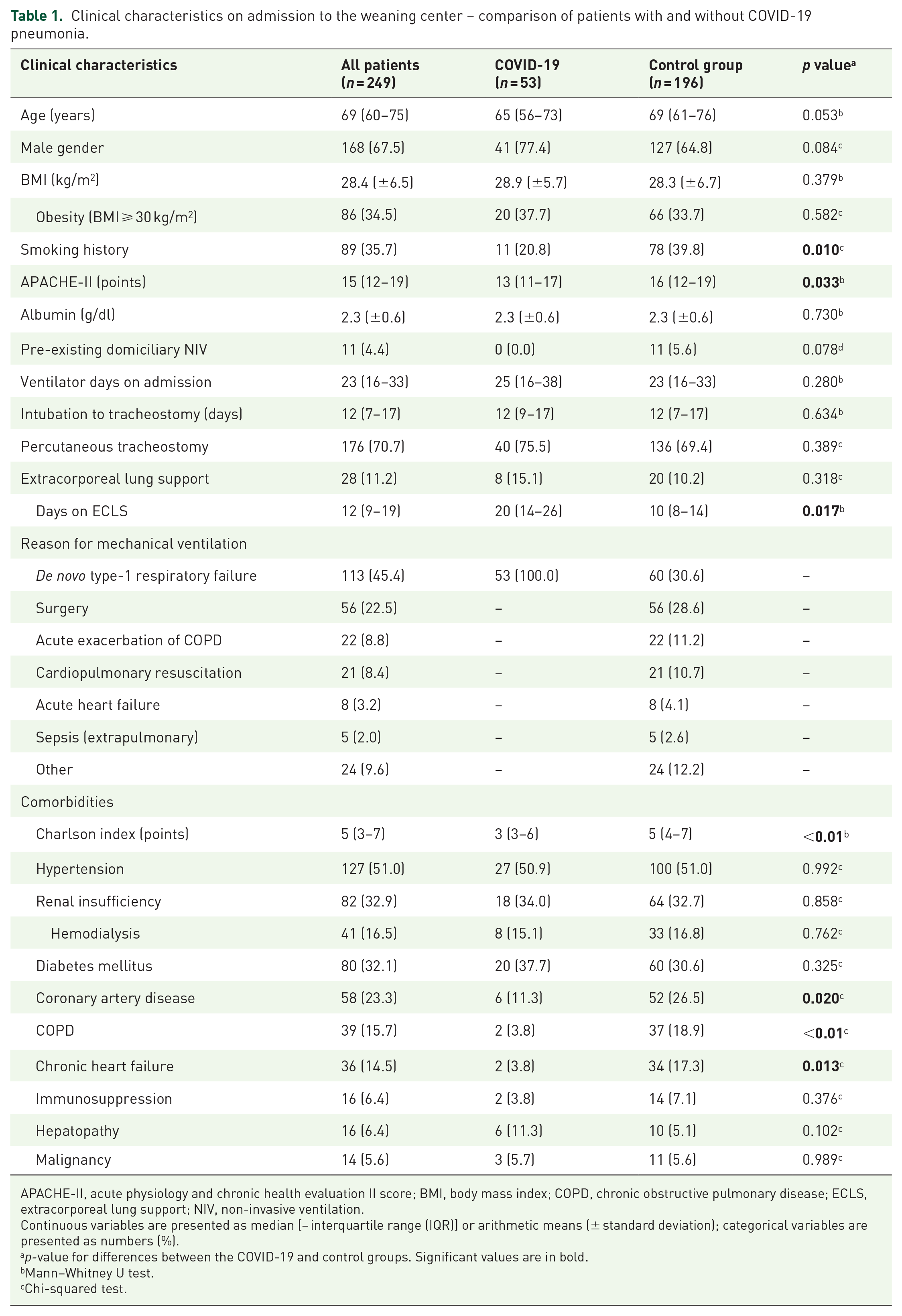
APACHE-II, acute physiology and chronic health evaluation II score; BMI, body mass index; COPD, chronic obstructive pulmonary disease; ECLS, extracorporeal lung support; NIV, non-invasive ventilation.
Continuous variables are presented as median [− interquartile range (IQR)] or arithmetic means (± standard deviation); categorical variables are presented as numbers (%).
p-value for differences between the COVID-19 and control groups. Significant values are in bold.
Mann–Whitney U test.
Chi-squared test.
VR and MP
Overall, 2106 ventilatory variables with respective arterial blood gas analyses were collected (see Supplementary l file 1: Tables S2–4). COVID-19 subjects demonstrated higher respiratory rates (with assisted ventilation in a higher percentage), tidal volumes, and mechanical ventilation PaCO2, resulting in significantly increased minute ventilation and VRs throughout the study [median VR 1.54 (IQR 1.28–1.89) versus 1.27 (IQR 1.08–1.50) at weaning onset, p < 0.01; median VR 1.38 (IQR 1.19–1.73) versus 1.24 (IQR 1.04–1.49) at weaning completion, p < 0.01]. Moreover, since the applied airway pressures (PEEP, Pmax, and the ∆Paw) did not differ at each point in time, they showed consistently higher dynamic lung-thorax compliance [median LTCdyn 37 (IQR 33–45) versus 35 (IQR 28–43) ml/cmH2O at weaning onset, p = 0.046; median LTCdyn 40 (IQR 35–48) versus 37 (IQR 30–44) ml/cmH2O at weaning completion, p < 0.01] and MP [median MP 26.0 (IQR 22.1–31.1) versus 21.3 (IQR 18.5–25.3) Joule/min at weaning onset, p < 0.01; median MP 24.2 (IQR 20.8–28.6) versus 20.1 (IQR 17.1–24.4) Joule/min at weaning completion, p < 0.01]. In contrast, although MP normalized to dynamic compliance (LTCdyn-MP and respective PaCO2-adjusted values, termed Power indexrs) was higher initially, these differences disappeared at the end of weaning (see Supplementary file 1: Tables S2–4). Comparing COVID-19 patients with the de novo type-1 respiratory failure subgroup yielded similar results.
Figure 2 illustrates the ventilatory variables of interest at different time points during weaning, stratified by group membership. According to the ANOVA, these variables declined consistently across both groups during weaning (see Supplementary file 1: Table S5), and similar to bivariate comparisons, significant differences in trajectories of variables between groups were observed regarding VR [F (1, 247) = 33.0; p < 0.01] and MP [F (1, 247) = 43.6; p < 0.01], but not for the Power indexrs2.0 [F (1, 247) = 0.30; p = 0.584] (see Supplementary file 1: Table S6).

Between-group differences in VR, MP, and the power indexrs2.0
Weaning outcomes
The COVID-19 group presented significantly lower weaning failure rates (9% versus 30%, p < 0.01). The median weaning duration did not differ between groups [13 (IQR 11–19) versus 12 (IQR 10–17) days, p = 0.166], but the total time spent on (invasive) mechanical ventilation was significantly longer among COVID-19 subjects [48 (IQR 36–64) versus 40 (IQR 31–53) days, p < 0.01] (see Supplementary file 1: Table S7).
Predictors of weaning
According to the logistic regression analysis, VR and MP were independently related to weaning failure in univariable analysis, but not in multivariable analysis. Weaning failure was independently associated with BMI [OR 1.07 * (95% CI 1.02–1.13) kg/m2], COPD [OR 16.1 (95% CI 5.74–44.9)], COVID-19 pneumonia as the cause for mechanical ventilation [OR 0.26 (95% CI 0.08–0.78)], and the Power indexrs2.0 [OR 1.36 × 10−3 (95% CI 1.18–1.57) cmH2O2/min] (Figure 3, see Additional file 1: Tables S8–9), confirmed by Kaplan–Meier survival analysis (Figure 4, see Supplementary file 1: Figure S2).
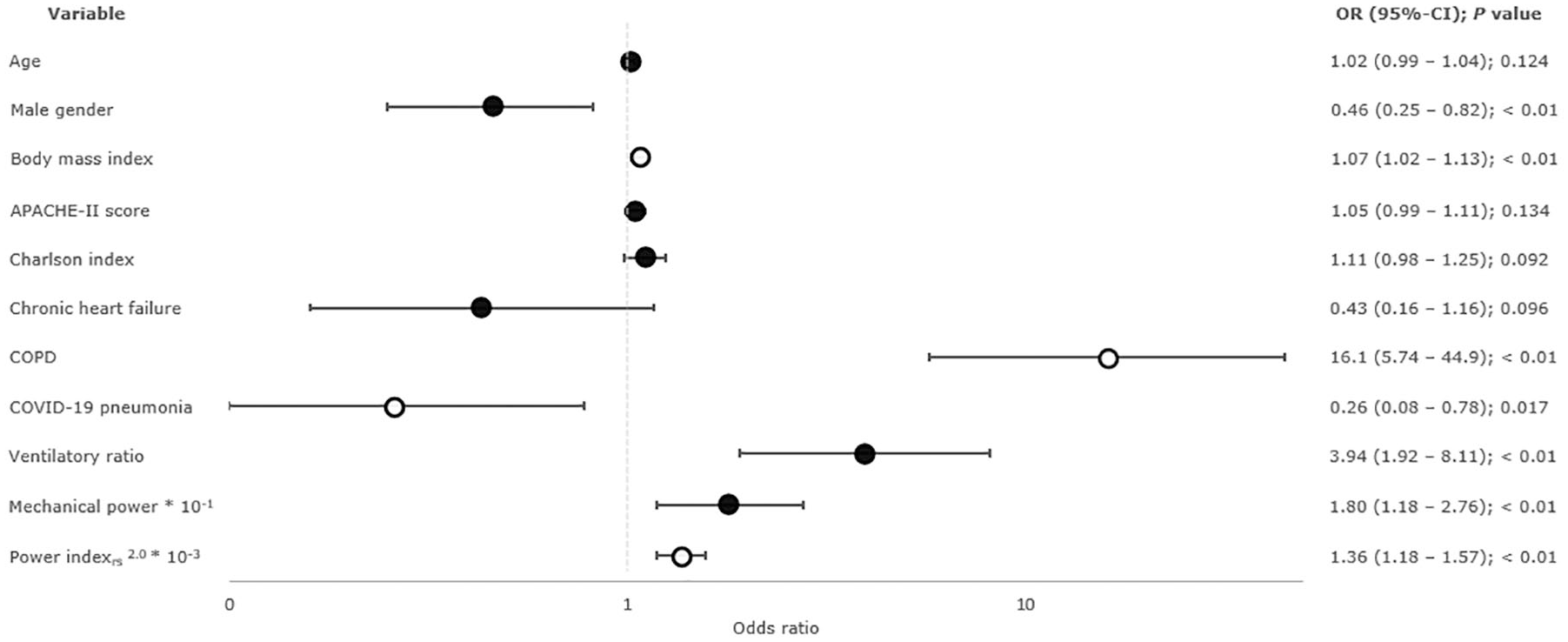
Results of binary logistic regression analysis – forest plot of variables independently associated with weaning failure.
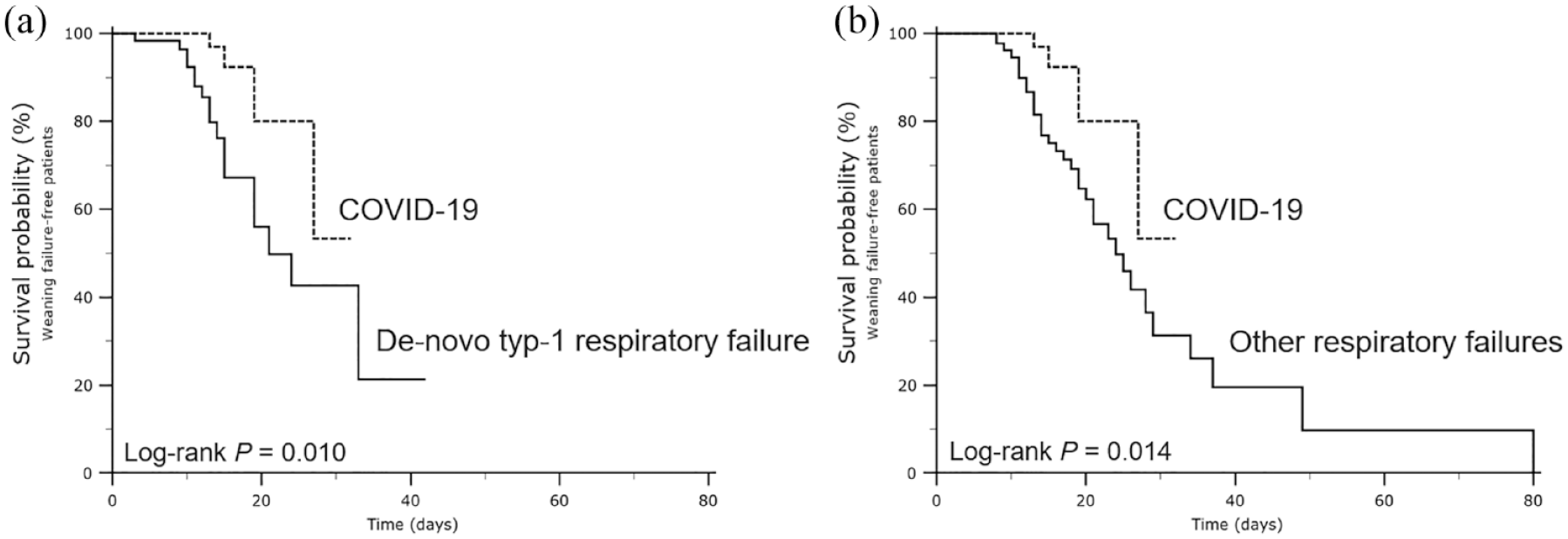
Kaplan–Meier curves comparing patients with and without COVID-19 regarding weaning failure. Comparison of COVID-19 patients with subgroups: (a) de novo type-1 respiratory failure and (b) other respiratory failures.
Exploratory analyses
To investigate the mechanisms explaining the high weaning success rates observed in COVID-19 patients, we conducted post hoc logistic regression analyses. The first step was to incorporate LTCdyn into the original multivariable model, a parameter significantly higher in this study and associated with prolonged ventilation in these patients, which resulted in the exclusion of COVID-19 pneumonia from the model. Next, these input variables were applied only to the control group, excluding LTCdyn again (see Supplementary file 1: Table S10, exploratory multivariable models 1 and 2). Moreover, ROC curve analysis determined an LTCdyn threshold of ⩽ 35.2 ml/cmH2O to best predict weaning failure in the entire study population (at the end of weaning), which was met by 42% of non-COVID-19 subjects and 21% of COVID-19 individuals (p < 0.01), respectively.
Discussion
The study results can be summarized as follows: In a heterogeneous cohort of tracheotomized patients undergoing prolonged weaning, COVID-19 subjects showed significant differences in ventilation efficiency and respiratory mechanics, exhibiting higher VRs and MP. The differences in MP were linked with higher lung-thorax compliance in COVID-19 patients, which may account for the lower weaning failure rate observed. There was an independent association between weaning failure and specific MP, but not with VR or MP.
At the pandemic’s beginning, clinical observations indicated that respiratory mechanics in COVID-19 pneumonia exhibited marked differences compared to the classical ARDS. 5 In the early stages of the disease, patients often present with profound hypoxemia in conjunction with well-preserved lung-thorax compliance, which is contrary to the behavior of other forms of ARDS. 7 However, subsequent studies involving larger sample sizes failed to replicate these findings,25,26 demonstrating a high degree of inter-individual variability in respiratory mechanics. 8 In this analysis, both study groups showed decreasing VR and MP throughout weaning, most likely due to improvements in respiratory mechanics and pulmonary gas exchange from medical intervention or spontaneous resolution of the underlying conditions (e. g. pulmonary infiltrates). COVID-19 patients displayed consistently higher indexes, best explained by corresponding ventilatory variables and blood gas analyses, showing higher minute ventilation and mechanical ventilation PaCO2 at each time point (indicating impaired ventilation efficiency). In contrast, higher specific MP (stress intensity) in the COVID-19 cohort at the beginning of weaning disappeared at completion as preserved lung-thorax compliance offset the higher respiratory rates.
Unsuccessful ventilator liberation occurred in 9% of COVID-19 subjects, which is low given that prior studies on prolonged mechanically ventilated non-COVID-19 patients determined failure rates of up to 75%. 27 However, this finding agrees with recent reports demonstrating high weaning success rates ranging between 71% and 93% in COVID-19 patients with tracheostomies,28–31 though not explicitly explained yet. The present analysis of ventilatory variables trajectories and between-group differences may help clarify this issue. COVID-19 subjects indicated a less severe impairment in respiratory mechanics compared to respiratory failures of other etiologies leading to prolonged mechanical ventilation. Although these differences (e.g. in lung-thorax compliance) were minor on average, they may have significantly impacted patients’ spontaneous breathing abilities. Previous studies have shown that weaning failure is strongly related to the level of stress intensity imposed on respiratory muscles (e.g. expressed as a pressure-time product or tension-time index of the diaphragm).32,33 However, in identifying the MP normalized to lung-thorax compliance (specific MP, which is a measure of stress intensity) to predict prolonged ventilation weaning failure accurately, recent research suggests a quadratic relationship between pressure and stress intensity. 17 When applied to spontaneous breathing conditions, even a slight increase in compliance may exponentially reduce respiratory muscle stress, facilitating successful liberation from the ventilator. This hypothesis is supported by the high weaning success rates and higher lung-thorax compliance in the present COVID-19 cohort and the exploratory logistic regression analysis results. In line with these findings, decreased static respiratory system compliance (< 40 ml/cmH2O) following intubation of COVID-19 respiratory failure patients has been associated with prolonged mechanical ventilation. 34
Apart from the diffuse alveolar damage typical of ARDS, COVID-19 pneumonia is characterized by widespread endothelial injury and extensive vascular thrombosis with obstruction of alveolar capillaries. 35 Moreover, mechanically ventilated COVID-19 patients are at increased risk of thromboembolic events, contributing to impaired pulmonary perfusion. 36 Both factors may increase pulmonary dead-space ventilation. The VR is a simple surrogate for impaired ventilation efficiency that can be easily calculated at the bedside, correlating well with the pulmonary dead-space fraction (VD/VT). 9 Developed and validated to predict mortality in ARDS, 15 this index may also help evaluate spontaneous breathing abilities in ventilated patients, with lower ratios indicating successful ventilator weaning.17,19 Furthermore, evidence suggests a respiratory subphenotype in COVID-19-related ARDS, characterized by an upward trend in VR and increased risk of prolonged ventilation.11,12 In the present COVID-19 cohort, weaning failure was less common despite higher VRs, which seems paradoxical at first glance. In addition, higher ratios were independently related to weaning failure in the univariable regression analysis. These findings may be rationalized by the multivariable analysis results, which indicate that specific MP (stress intensity) along with preserved lung-thorax compliance are the primary determinants of prolonged weaning failure, suggesting that spontaneous breathing abilities remain unaffected as long as intact respiratory mechanics compensate for impaired ventilation efficiency.
MP is a concept introduced to clarify the mechanisms involved in ventilator-induced lung injury since it encompasses all ventilatory variables considered responsible. 10 High MP was independently linked with increased mortality in ARDS patients, but its impact on lung injury remains debated. 16 Moreover, COVID-19 patients with increasing MP over the first 4 days following intubation had longer durations of mechanical ventilation and fewer ventilator-free days on day 28. 11 As with the results for the VR, the present COVID-19 cohort demonstrated lower weaning failure rates despite consistently higher MP throughout weaning, which contradicts prior research. 17 Once again, these findings may be explained by the results of the multivariable analysis. Since specific MP (the Power indexrs) was retained in the final model, the association between MP and weaning failure or success varied with lung-thorax compliance. In other words, iso-MP (pressure times volume per unit of time) may predict weaning failure if generated by high pressures and low tidal volumes, while it may indicate weaning success when caused by low pressures along with high tidal volumes (synonymous with high compliance).
This is the first study using longitudinal data to compare prolonged ventilated COVID-19 patients with a heterogeneous group of non-COVID-19 subjects based on respiratory physiology, offering information on mechanisms that might explain differences in weaning outcomes. However, the results need to be interpreted in light of several limitations. First, external validity remains undetermined since it is based on a monocentric approach. Second, despite including all patients from the first three waves of the pandemic treated at our center, the COVID-19 cohort had a low sample size, in part due to the fact that Germany was largely spared from the first pandemic wave. Third, in the absence of information about intubation practices of most referring ICUs (e.g. advocacy for ‘early intubation’ in COVID-19 patients soon after the beginning of the pandemic), we might have overlooked this critical covariate concerning weaning outcomes when analyzing the data. Fourth, ventilatory variables used to calculate the VR and MP are typically measured in controlled ventilation modes. Despite applying A/C ventilation to unload respiratory muscles effectively, diaphragm activation for ventilator triggering may have distorted tidal volumes and, consequently, calculation of dynamic lung-thorax compliance and MP. However, an assisted breath does not necessarily indicate a high level of spontaneous activity with this mode. When the ventilator is triggered with minimal effort, it delivers a breath similar to controlled ventilation (passive insufflation occurs).37,38 Moreover, spontaneous activity was common in both groups, and using the median of ventilatory variables more than 48 h (including controlled breaths) may have balanced such effects and reduced bias to a certain extent. In this respect, the study may be considered proof of concept, although further research to confirm the results will be required.
Conclusion
COVID-19 patients demonstrated marked differences in ventilation efficiency and respiratory mechanics among prolonged mechanically ventilated individuals with tracheostomies, resulting in higher VRs and MP throughout weaning. The differences in MP were linked with higher lung-thorax compliance in COVID-19 patients, which may account for the lower weaning failure rate observed. There was an independent relationship between weaning failure and specific MP, but not with VR or MP.
Supplemental Material
sj-pdf-1-tar-10.1177_17534666231155744 – Supplemental material for Ventilatory ratio and mechanical power in prolonged mechanically ventilated COVID-19 patients versus respiratory failures of other etiologies
Supplemental material, sj-pdf-1-tar-10.1177_17534666231155744 for Ventilatory ratio and mechanical power in prolonged mechanically ventilated COVID-19 patients versus respiratory failures of other etiologies by Alessandro Ghiani, Konstantinos Tsitouras, Joanna Paderewska, Kathrin Kahnert, Swenja Walcher, Lukas Gernhold, Claus Neurohr and Nikolaus Kneidinger in Therapeutic Advances in Respiratory Disease
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.