
Abstract
Background:
Numerous studies have shown that dipeptidyl peptidase-4 inhibitors (DPP-4i) may regulate immunological pathways implicated in asthma. The association between DPP-4i use and risk of asthma development is limited, however.
Aim:
We aimed to evaluate if DPP-4i treatment in individuals with type 2 diabetes mellitus (T2DM) is associated with a lower risk and severity of asthma.
Methods:
We performed a population-based retrospective cohort study using the Longitudinal National Health Insurance Research database between 2008 and 2015. After one-to-four propensity score matching from 1,914,201 patients with defined criteria, we enrolled 3001 patients who were on DPP-4i (DPP-4i group) for a diagnosis of T2DM but without a diagnosis of asthma for further analysis. Cox proportional hazards regression analysis was performed to estimate and compare the risk of developing and severity of asthma, including no acute exacerbations event (No-AE), acute exacerbations (AEs), status asthmaticus (Status), and required endotracheal intubation (ET-tube intubated), between the two groups.
Results:
The participants had a mean age of 66.05 ± 17.23 years and the mean follow-up time was 4.96 ± 4.39 years. The risk of asthma development was significantly lower in the DPP-4i group than in the non-DPP-4i group [adjusted hazard ratio (HR) = 0.65; 95% confidence interval (CI) = 0.29–0.83; p < 0.001], with a class effect. This trend was observed for severity of asthma as No-AE (HR = 0.55; 95% CI = 0.24–0.70; p < 0.001), AE (HR = 0.57; 95% CI = 0.26–0.73; p < 0.001), and Status (HR = 0.78; 95% CI = 0.35–0.99; p = 0.047), but not in ET-tube intubated cases (HR = 0.96; 95% CI = 0.43–1.22; p = 0.258).
Conclusion:
The use of DPP-4i decreased the risk and severity of asthma with a class effect among No-AE, AE, status of asthma events, but not in ET-tube intubated events. Our report suggests that DPP-4i may play a role in attenuating the impact of asthma on incidence in the future and on more severe forms of disease exacerbation in T2DM patients.
Introduction
According to the Nutrition and Health Survey, the prevalence of diabetes mellitus (DM) was 11.6% (men = 12.9%; women = 10.5%) in Taiwan during 2013–2016. 1 Jiang et al. 2 indicated that a 25% increase in incidence rate in diabetes based on the 2000–2009 National Health Insurance (NHI) database. Asthma, a chronic inflammatory disease involving the airways of the lungs, is prevalent and poses considerable not only economical but also individual physical burdens worldwide. 3 In addition, the prevalence of physician-diagnosed adult asthma, more severe than early-onset asthma, was 2.1% in the Taiwan population. 4 By age, the prevalence of asthma is 5–9% in childhood and 3% in young adults; however, the prevalence of asthma showed a peak of 6.8–12% after the age of 50 years.5,6 Furthermore, patients with adult-onset asthma have a poor prognosis, with a faster decline in lung function, and more severe persistent airflow limitation.7–9 Moreover, individuals with diabetes are at increased risk for chronic obstructive pulmonary disease (COPD), asthma, pulmonary fibrosis, and pneumonia. 10 Brumpton et al. 11 had reported that waist circumference and hyperglycemia or DM were independent risk factors for asthma. Lee et al. 12 also indicated that abdominal obesity, a chronic inflammation status associated with insulin resistance and developing DM, was a risk factor for asthma-like symptoms. Singh et al. 13 had reported that hyperglycemia and hyperinsulinemia in the lungs might contribute to decreased lung function and a higher occurrence of asthma in individuals with diabetes.
As the first-line treatment for type 2 DM, metformin has been reported to be associated with a lower risk of asthma exacerbation, asthma-related emergency department visits, and hospitalization. 14 Another previous study in a Taiwan population reported that among patients with concurrent asthma and diabetes, metformin users had a lower risk of asthma-related hospitalization and asthma exacerbation. 15 In addition, a meta-analysis indicated that metformin decreased the risk of asthma-related emergency room visits for patients with concurrent asthma and diabetes but was not statistically significant for decreasing asthma-related hospitalization and exacerbation. 16
The benefits of second-line with treatment agents for type 2 DM, including sulfonylureas (SUs), sodium-glucose cotransporter 2 inhibitors, glucagon-like peptide-1 receptor (GLP-1R) agonists, and dipeptidyl peptidase-4 inhibitors (DPP-4is), when treating asthma were limited and inconclusive, however.17–20
DPP-4, also known as adenosine deaminase complexing protein 2 or cluster of differentiation 26 (CD 26), is encoded by the DPP-4 gene in humans. 21 There is an emerging role of DPP-4 as a therapeutic target in chronic lung disease, including asthma, COPD, and lung cancer.22,23 Furthermore, an increasing number of studies have indicated that DPP-4 is implicated in airway inflammation and experimental asthma.24,25 Therefore, we constructed a study to assess the association between DPP-4i use and the incidence and severity of asthma based on the Taiwan National Health Insurance Research Database (NHIRD).
Materials and methods
Data source and participants
A single-payer NHI program was launched by the Taiwanese government in March 1995. We used data from the NHIRD and 1,914,201 patients included in the Longitudinal Health Insurance Database in Taiwan (2008–2015). The annual coverage rate of the NHI program has ranged from 96.1% to 99.6%, with more than 20 million Taiwanese citizens enrolled since 1997. In the NHIRD, all diseases before 2015 were coded according to the International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM). All diagnoses of T2DM were made by board-certified internists, endocrinologists, or other related specialists, and all diagnoses of asthma were made by board-certified internists, pulmonologists, or other related specialists.
Ethical approval
This retrospective cohort study was approved by the Institutional Review Board of Tri-Service General Hospital (IRB No. B-110–47), and informed consent was waived as the database used in this study was deidentified.
Study design and sampled participants
Sitagliptin was the first marketed DPP-4i in Taiwan since 2008. We choose the time between 1 January 2008 and 31 December 2015 for a cumulative analysis of the occurrence of asthma development or exacerbation.
We recruited patients aged ⩾18 years with ICD-9-CM diagnosis codes for T2DM (ICD-9-CM: 250.XX), who had at least three outpatient visits, and used DPP-4i for >90 days (Figure 1). Treatment of patients in non-DPP-4i group included metformin, SUs, meglitinides, thiazolidinediones, sodium-glucose cotransporter 2 inhibitors, α-glucosidase inhibitors, and insulin. We excluded patients who were identified on the index date as (1) being aged 18 years or younger; (2) those previously diagnosed with asthma; (3) those with comorbid disorders (COPD, respiratory tract cancer, bronchiectasis); (4) those who were on DPP-4i before the index date; and (5) those who received GLP-1 agonist before the tracking (Figure 1).
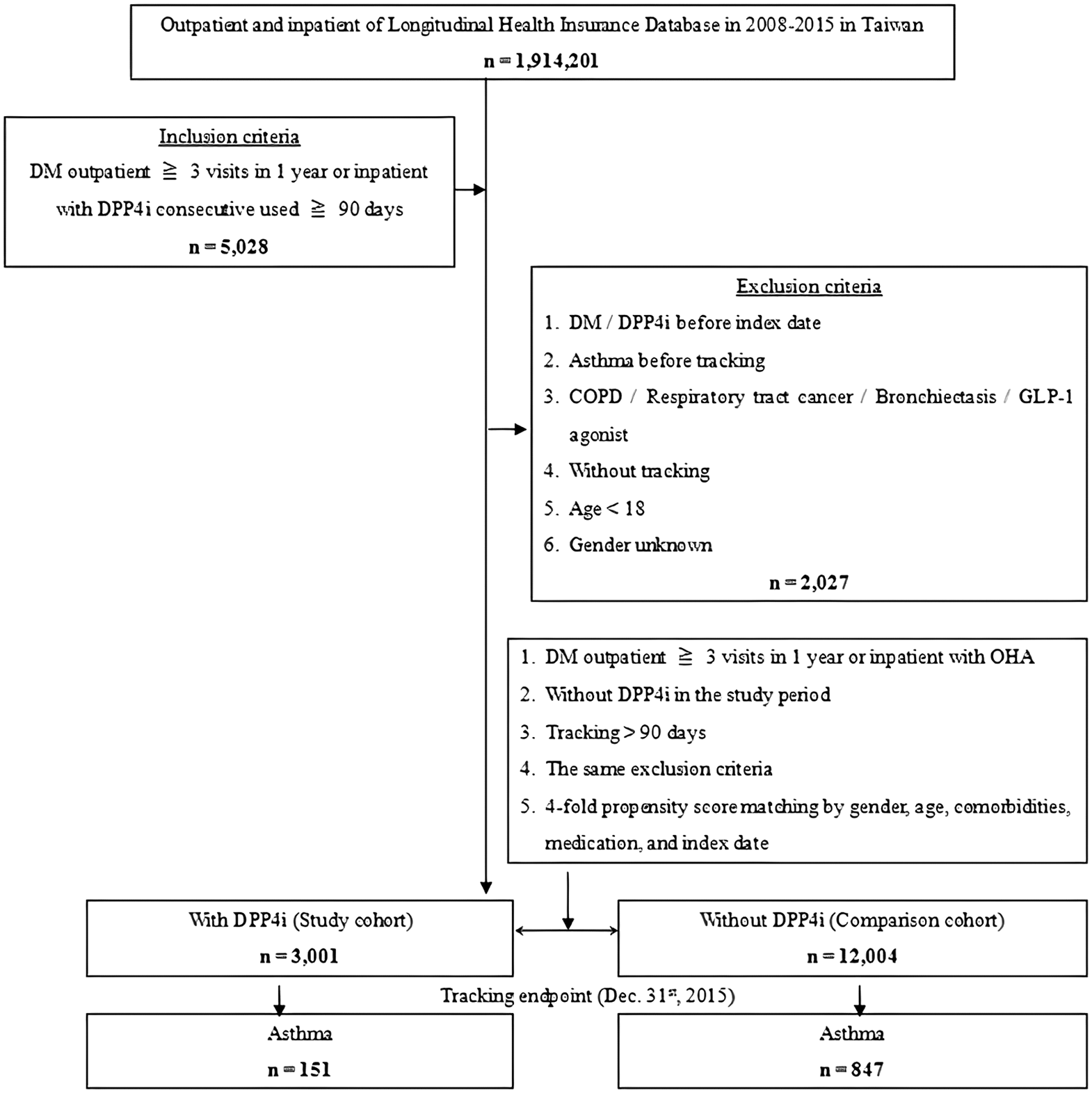
The flow chart of study sample selection.
Propensity score matched comparison cohort
To reduce demographic differences between the DPP-4i group and the non-DPP-4i group, we performed 1:4 propensity score matching by age, sex, race/ethnicity, history of smoking, medical comorbidities, complications of T2DM, and urbanization level. After 1:4 propensity score matching from 1,914,201 patients with defined criteria, we finally enrolled 3001 patients in DPP-4i group and 12,004 patients in non-DPP-4i group (Figure 1).
Covariates and outcome measurements
All covariates were measured during the pre-index period. They were age, sex, race/ethnicity, history of smoking, hypertension (HTN), hyperlipidemia, obesity, macrovascular or microvascular complications of T2DM, chronic kidney disease, obstructive sleep apnea syndrome, and urbanization level. The urbanization level of residence was defined according to the population and various indicators of the level of development. Level 1 was defined as a population >1,250,000, and a specific designation as political, economic, cultural, and metropolitan development. Level 2 was defined as a population between 500,000 and 1,249,999, and as playing an important role in the political system, economy, and culture. Urbanization Levels 3 and 4 were defined as a population between 149,999 and 499,999, and <149,999, respectively. 26 The medical comorbidities and T2DM vascular complications were selected by corresponding ICD-9-CM codes in outpatient medical claims previous to the index date including HTN (ICD-9-CM: 401.1, 401.9, 402.10, 402.90, 404.10, 404.90, 405.1, 405.9), hyperlipidemia (ICD-9-CM: 272), obesity (ICD-9-CM: 278), heart failure (ICD-9-CM: 428), obstructive sleep apnea (ICD-9-CM: 780.51, 780.53, 780.57), microvascular complications of T2DM (ICD-9-CM: 250.52, 362.0 for retinopathy; 250.6, 357.2 for neuropathy; 250.4, 250.42 for nephropathy), and macrovascular complications of T2DM (ICD-9-CM: 430-438 for stroke; 440.2–440.3, 440.8–440.9, 443, 444.22, 444.8, 447.8–447.9 for peripheral arterial disease; 410-41 for coronary artery disease). We adjusted the variables in relation to the Charlson comorbidity index scores to better control the confounding effect from comorbidity. The primary outcomes in this study were events of asthma development but no acute exacerbations event (No-AE), acute exacerbation of asthma (AE), status asthmaticus (Status), and requiring endotracheal intubation (ET-tube intubated). No-AE was defined as a patient who was diagnosed with asthma and received asthma therapy without an asthma exacerbation event (ICD-9-CM: 493.00, 493.10, 493.20, 493.90). AE was defined as a patient who used a systemic corticosteroid plus an emergency room visit during the follow-up period (ICD-9-CM: 493.02, 493.12, 493.22, 493.92). Status was defined as severe asthma unresponsive to repeated courses of systemic corticosteroid or beta-agonist therapy in an emergency room visit (ICD-9-CM: 493.01, 493.11, 493.21, 493.91). ET-tube intubated was as defined as AE or Status and ET-tube intubated (AE/Status with ICD-9-CM: OP96.04).
Statistical analysis
Statistical analysis was performed using the Statistical Product and Service Solutions, version 22 (SPSS Inc., Chicago, IL, USA). Demographic characteristics were compared using the t-test for continuous variables and the Chi-square test for discrete variables. We used multivariate Cox proportional hazard models to obtain the hazard ratios (HRs) with 95% confidence intervals (CIs) of the risk of asthma. Kaplan–Meier plots and the log-rank test were performed to evaluate differences in the risk of asthma between the DPP-4i and non-DPP-4i groups. A p value (two-sided) <0.05 was considered to indicate statistical significance.
Results
Study sample characteristics
The baseline characteristics of the study sample are presented in Table 1. There were 3001 patients in the DPP-4i group and 12,004 patients in the non-DPP-4i group after fourfold propensity score matching. The participants had a mean age of 66.05 ± 17.23 years. The prevalence of comorbidities, listed in Table 1, showed no significant differences (all p value > 0.05). The mean follow-up times for the DPP-4i group and the non-DPP-4i group were 5.22 ± 4.48 versus 4.90 ± 4.37 years, respectively. The mean time to asthma exacerbation for the DPP-4i group and the non-DPP-4i group were 4.49 ± 4.11 versus 3.97 ± 3.76 years, respectively (p = 0.35 > 0.05).
Characteristics of study in the baseline.

CCI_R, Charlson comorbidity index without dementia; DM, diabetes mellitus.
Categorical variables were compared using the Chi-square or Fisher’s exact test and expressed as N (%).
Continuous variables were compared using Student’s t test.
Table 2 shows that asthma developed in 151 (5.03%) patients in the DPP-4i group and 847 (7.06%) patients in the matched controls (p value < 0.001). Figure 2 demonstrates the Kaplan–Meier curve for the cumulative risk of asthma in the DPP-4i group and the non-DPP-4i group. A significant difference was observed between the two groups once 2 years of DPP-4i exposure had been reached (p = 0.037 by the log-rank test).
Characteristics of study in the endpoint.

CCI_R, Charlson comorbidity index without dementia; DM, diabetes mellitus.
Categorical variables were compared using the Chi-square or Fisher’s exact test and expressed as N (%).
Continuous variables were compared using Student’s t test.

Kaplan–Meier for cumulative risk of asthma among DM patients aged 18 years and over stratified by DPP-4i with the log-rank test.
Table 3 shows the Cox regression analysis of the association between DPP-4i use and the risk of developing asthma. The HR of overall asthma was 0.57 (95% CI = 0.27–0.79; p < 0.001) and remained significant after adjusting for confounding variables (adjusted HR = 0.65; 95% CI = 0.29–0.83; p < 0.001).
Factors of asthma using the Cox regression.

CCI_R, Charlson comorbidity index without dementia; CI, confidence interval; DM, diabetes mellitus; HR, hazard ratio.
Adjustment for age, sex, race/ethnicity, ever smoking, HTN, hyperlipidemia, obesity, macrovascular or microvascular complications of DM, chronic kidney disease, obstructive sleep apnea syndrome, the Charlson comorbidity index score, and urbanization level.
Table 4 reveals that compared with the non-DPP-4i group, the HRs of the DPP-4i group for severity of asthma as No-AE, AE, Status, and ET-tube intubated were 0.55 (95% CI = 0.24–0.70; p < 0.001), 0.57 (95% CI = 0.26–0.73; p < 0.001), 0.78 (95% CI = 0.35–0.996; p = 0.047), and 0.96 (95% CI = 0.43–1.22; p = 0.258), respectively. The events of the DPP-4i group for severity of asthma as (No-AE, AE, Status, and ET-tube intubated) were (45, 42, 36, and 28) and the events of the non DPP-4i group were (301, 270, 169, and 107), respectively.
HRs of asthma severity categorized by with or without DPP-4i.

AE, acute exacerbation; CI, confidence interval; ET-tube intubated, required endotracheal intubation; HR, hazard ratio; No-AE, no acute exacerbations event; PYs, person-years; Status, Status asthmaticus.
Without DPP-4i as reference group.
Status asthmaticus does not respond to standard treatments of bronchodilators and corticosteroids.
In adjusted Hazard ratio, HR was adjusted according to the variables listed in the baseline characteristics.
Table 5 shows the comparison of the risk of asthma among different DPP-4i types. All types of DPP-4i had significant protective effects against asthma development when the duration of therapy was greater than 1 year (all p values < 0.001).
Comparison of the risk for asthma according to the use of DPP-4i.
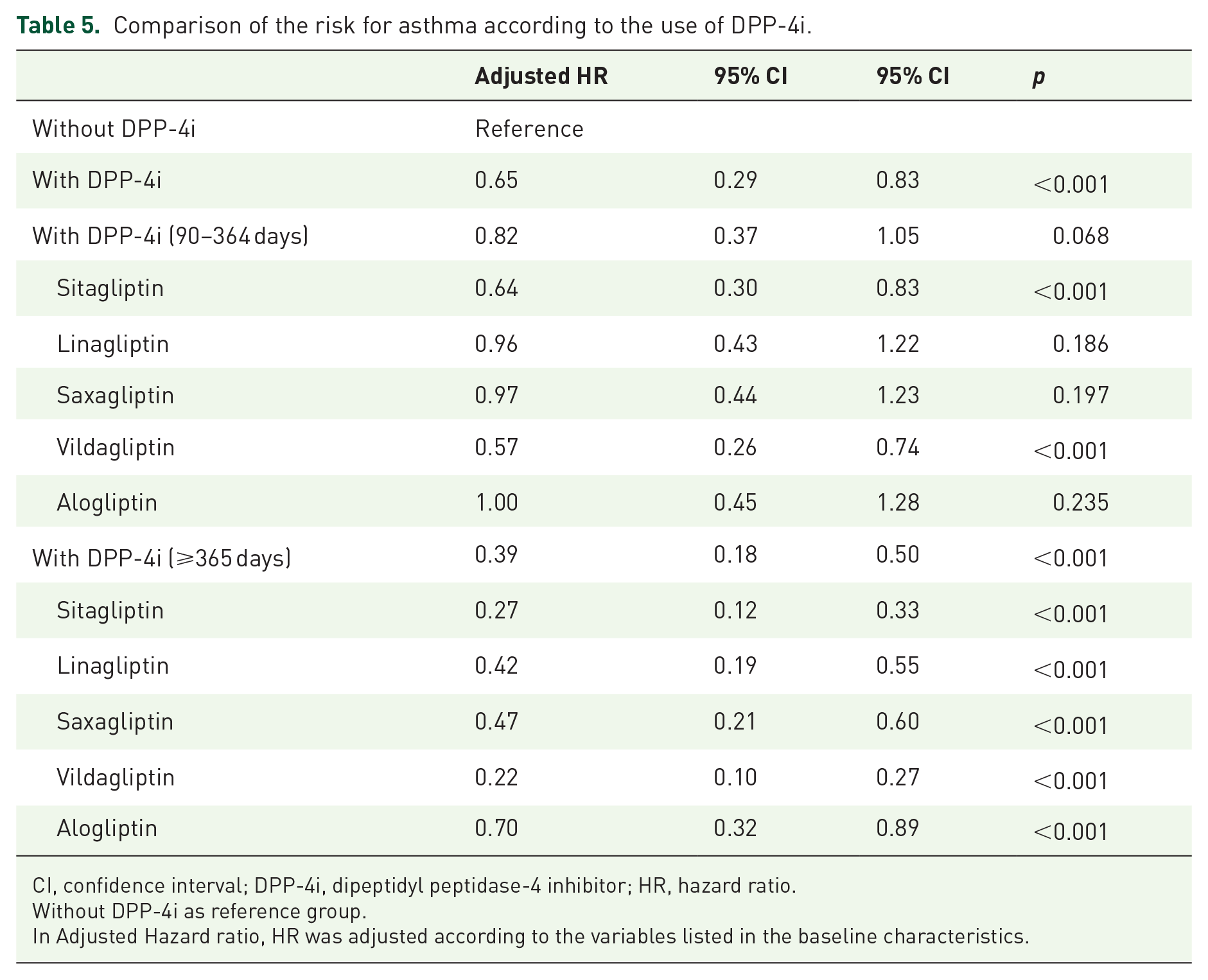
CI, confidence interval; DPP-4i, dipeptidyl peptidase-4 inhibitor; HR, hazard ratio.
Without DPP-4i as reference group.
In Adjusted Hazard ratio, HR was adjusted according to the variables listed in the baseline characteristics.
Discussion
This study indicated that the DPP-4i group was associated with a 34% lower risk of asthma development compared with that of the non-DPP-4i group. In addition, compared with the non-DPP-4i group, the DPP-4i group showed associated decreased risks for developing asthma, including Non-AE, AE, and status of asthma but excluding ET-tube intubated. Endotracheal intubation may be required when a patient presented with respiratory distress. This study, however, defined ET-tube intubated as AE or Status and ET-tube intubated (AE/Status with ICD-9-CM: OP96.04). There are many reasons affect the results such as conservative physicians or conservative family members will choose bilevel positive airway pressure machine for respiratory failure patients instead of ET-tube intubation. This study also demonstrated that all types of DPP-4i may decrease the incidence of asthma in the future in T2DM patients when the duration of therapy was greater than 1 year. It seems that DPP-4i use has cumulative effect against asthma development.
Shiobara et al. 24 indicated that interleukin (IL)-13 induces DPP-4 expression in bronchial epithelial cells and leads to eosinophilic airway inflammation in humans. 27 Meyerholz et al. 28 also confirmed DPP-4 overexpression in alveolar type II cells, type I cells, and alveolar macrophages in chronic lung disease patients. In addition, Van der Velden et al. 29 concluded that increased expression of aminopeptidase N and DPP-4 can be found in the bronchial epithelium of allergic asthmatics. Furthermore, Nader 30 indicated that sitagliptin-like dexamethasone may play a beneficial role in reducing airway inflammation and remodeling in a murine model of chronic asthma. Helal et al. also demonstrated that saxagliptin had a marked antiasthmatic effect in allergic asthma through the modulation of toll-like receptor 4 (TLR4) and nuclear factor-kappa B (NF-kB) signaling in a murine model. This group concluded that saxagliptin might represent a promising therapeutic agent for acute allergic asthma. 31 Moreover, Klemann et al. 32 reported the role of DPP-4i in maintaining lymphocyte composition and function, T cell activation and costimulation, memory T cell generation, and thymic emigration patterns during immune-senescence. Collectively, these previous studies suggested a role for DPP-4i in chronic eosinophilic airway inflammation disease, and this hypothesis was confirmed in a murine model. There are no clinical studies to support this established evidence, however. Our data support previous results and suggest that DPP-4i may play a role in attenuating the impact of asthma on incidence in the future and on more severe forms of disease exacerbation in T2DM patients.
Wu et al. 33 have suggested that metformin may be beneficial for the Asthma–COPD overlap group, highlighting the potential relevance of metabolic pathways in these patients. In addition, Li et al. 15 have reported that, in patients with concurrent asthma and diabetes, metformin users had a lower risk of asthma-related hospitalization and asthma exacerbation. These benefits were attributed to metformin effects. First, metformin inhibits airway smooth muscle proliferation through AMP-activated protein kinase (AMPK)-mediated inhibition of transforming growth factor-β1 signaling. 34 In addition, metformin treatment was associated with an increase in regulatory T-lymphocytes, which have been shown in a separate study to reduce airway inflammation and hyperresponsiveness. 35 These previous studies suggested that attenuating the impact of asthma on exacerbations was not only the blood sugar lowering effect but also the reduced inflammation and hyperresponsiveness effects. In the same way, the benefits of DPP-4i for asthma may be attributed to its lowering of blood sugar, T cell activation, memory T cell generation, and reduction of inflammation of airway through the modulation of TLR4 and NF-kB.
Furthermore, our data show that microvascular complications of T2DM and CCI_R are better in the non-DPP-4i group. In clinical practice (during AD 2008–2015), the first choice of oral antidiabetic drugs (OADs) after metformin were SU or thiazolidinediones (TZDs) because of the more powerful lowering HbA1c ability.36,37Optimize glucose control can reduce the risk or slow the progression of microvascular complications of DM. Moreover, there is an emerging role of SGLT2i in reducing the risk of kidney disease progression and preventing worsening of albuminuria.38,39 Thus, if the treatment strategy for DM including SGLT2i, the microvascular complications of DM will decrease in the future. The Taiwan NHI benefits only offer one drug between DPP-4i and SGLT2i, however. This might be the reason for why microvascular complications of DM, and CCI_R are better in the non-DPP-4i group.
Contrary to this study results, Colice G. et al. 14 reported no associations between DPP-4i use and asthma control based on a retrospective, matched cohort study. Participants in Colice G.’s study were concurrent asthma and T2DM patients newly initiating DPP-4i treatment for T2DM. Thus, the asthma medication strategy and participants’ medical compliance had impacted the study asthma events. This study investigated T2DM patients without asthma and analyzed whether asthma events developed after participants were included.
Strengths of this study include the very large sample size and T2DM, and asthma diagnoses were confirmed by a trained physician. In addition, this study included patients who were diagnosed with T2DM but without asthma and were recruited for cumulative analysis of occurrences of asthma development or exacerbation. Based on this study design, we could minimize the impact of patients with poorly controlled asthma before they were recruited.
Limitations
There were still some limitations to this study, however. First, patients with asthma or T2DM could be identified using insurance claims data. Furthermore, data on the severity and duration of T2DM and impact on diabetes control, such as HbA1c levels and body mass index (BMI) were not available. In addition, it was inability to classify endotypes (T2 high/T2 low) and phenotypes (such as atopic, late onset, smoke-related, and obesity-related) of asthma based on our database. Besides, we could only estimate treatment durations of each DPP-4i by dividing the cumulative doses of individual medications by defined daily doses. Moreover, there was no patient had used the biological therapies, including anti-immunoglobulin E (IgE): omalizumab; anti-IL-5: mepolizumab, reslizumab, and benralizumab, and anti-IL-4R: dupilumab during this study (2008–2015). Finally, a population-based study cannot clarify the actual mechanism of the association between DPP-4i use and asthma in patients with T2DM, and further efforts in this direction are required.
Conclusion
In conclusion, DPP-4i use was associated with a 34% lower risk of asthma development in a Taiwanese population with T2DM compared with that in the non-DPP-4i use group. In addition, DPP-4i use has also associated with protected against the development of asthma of different severities with a class effect among No-AE, AE, status of asthma events, but not in ET-tube intubated events. In brief, our report suggests that DPP-4i may play a role in attenuating the impact of asthma on incidence in the future and on more severe forms of disease exacerbation in T2DM patients.