
Abstract
Background:
Anastomotic complications are common after lung transplantation (1.4–33% of cases) and still associated with a high morbi-mortality.
Methods:
The current study is a monocenter retrospective analysis of symptomatic anastomotic complications (SAC) occurring after lung transplantation between 2010 and 2016, using the macroscopic, diameter, and suture (M-D-S) classification from consensus of French experts in bronchoscopy. The objectives were to determine incidence from surgery, risk factors, and impact of survival of SAC. We defined SAC as M-D-S abnormalities (stenosis ⩾ 50% or dehiscence) requiring bronchoscopic or surgical interventions.
Results:
A total of 121 patients were included. SAC occurred in 26.5% of patients (n = 32), divided in symptomatic stenosis for 23.7% (n = 29), and symptomatic dehiscence in 2.5% (n = 3). In multivariate analysis, donor bacterial lung infection [HR 2.08 (1.04–4.17), p = 0.04] and age above 50 years [HR 3.26 (1.04–10.26), p = 0.04] were associated with SAC occurrence. Cystic fibrosis etiology was associated with better survival on Kaplan–Meier curve (p < 0.001). SAC [HR 2.15 (1.07–4.32), p = 0.03] was independently associated with worst survival. The 29 symptomatic patients because of stenosis required endoscopic procedure, of whom 16 patients needed bronchial stent placement. Four patients underwent surgery: three patients because of dehiscence and one because of severe bilateral stenosis (re-transplantation).
Discussion:
SAC occurred in 26.5% of patients. Donor lung infection was the only alterable identified factors. The increase rate of SAC in older patients above 50 years of age encourages in regular endoscopic monitoring.
Introduction
Despite remarkable improvement in surgical techniques and post-operative intensive care unit management, lung transplantation is still associated with significant mortality and morbidity related to infections, rejection episodes, or surgical complications. Among the latter, anastomotic complications are defined by any injuries involving bronchial anastomoses, such as ischemia or bronchial anastomotic necrosis, stenosis (stricture, malacia, or granulomas), and dehiscence. Bronchial arteries are necessarily sectioned during surgical procedure. However, 2–4 weeks are needed for revascularization and the sole retrograde circulation from the low pressure arterial pulmonary regimen allows healing of anastomoses at the initial stage. 1 Complex surgical strategies of arterial reimplantation have been proposed, but their benefit correlates with prolonged graft ischemic time, known to be deleterious. 2
Studies reporting anastomotic complications are heterogeneous with a wide variation of incidence due to the absence of consensual classification. Depending on authors, anastomotic complications occur from 1.4% to 33% of lung transplantations with a mortality ranging from 2% to 4%.3–6 Couraud et al. 7 were the first to propose a classification for anastomotic complications but they focused on bronchial anastomotic necrotic lesions. Other classifications were not precise enough regarding the localization of anastomotic complications or the description of multiple complications. 1 In 2013, a consensus of French experts in bronchoscopy established a classification for anastomotic complications, aiming to be simple, applicable, and efficient. 3 The macroscopic, diameter, and suture classification (M-D-S) describes most of the possible complications and localizations (suture, extend to lobar or beyond). In the available literature, this classification has only be used in Yserbyt et al. 6 study, whereas most of French lung transplant centers routinely use it.
Several risk factors of anastomotic complications after lung transplantation have already been identified in previous studies, such as donor conditions, initial disease, surgical technique, immunosuppressive therapy, right-sided anastomoses, infections, and comorbidities.6,8–10 Nevertheless, few preventive strategies can be proposed because most of these risk factors are not alterable. Curative therapeutic options include medical treatment (immunosuppressive change, antibiotics), bronchoscopic intervention (dilatation, bronchial stent placement), and surgical intervention.
The objectives of the study were to determine the incidence of symptomatic anastomotic complications (SACs) in lung-transplanted patients and to identify risks factors to develop each complication with the help of regular M-D-S scoring.
Material and methods
Design and population
The current study is a monocenter retrospective analysis. Patients were eligible if lung-transplanted adults followed in Nantes University Hospital, France, between January 1, 2010 and December 31, 2016. We excluded heart-lung transplantations and deaths that occurred within the first 30 days after lung transplantation and patients opposed to participation.
Outcomes
The main outcome of this study was the time between surgery and SAC occurrence. SAC were defined as M-D-S abnormalities (stenosis D2 ⩾ 33% or dehiscence ⩾ S1) requiring bronchoscopic or surgical interventions because of dyspnea, handicapping cough, forced expiratory volume in 1 s (FEV1) decline, or recurrent infection.
Secondary outcomes were as follows:
Time between surgery and patient death
To determine the incidence of severe endoscopic complications and provide the rate of worst anastomoses endoscopic scoring for each M-D-S and each bronchus (left or right) classification in the population
To investigate the risk factors associated with SAC
To describe SAC management.
Data collection
Donor
Epidemiologic data were collected: age, sex, weight, height, tobacco history, intensive care unit length of stay, and respiratory infections.
Recipient
Medical history was retrieved from hospital medical reports: age, sex, underlying disease, nutritional parameters, bacterial or fungal colonization before lung transplantation.
Graft follow-up
Surgical information, total graft ischemic time, intensive care unit length of stay, and organ dysfunctions were collected. Post-transplant complications and their treatments were collected: infections, immunosuppressive regimen, diabetes, allograft dysfunction, and anastomotic complications.
Donor infection was based on anonymous biomedicine agency file when the following criteria were present: purulent respiratory secretions associated with identified bacteria and compatible radiological findings on computed tomography (CT)-scan.
Recipient colonization was defined by bacterial or fungal identification more than two times a year (3 months apart) without active infection.
Graft infection was defined by isolation of bacteria or fungi associated with clinical (cough, secretions, fever > 38.5°C), biological (leukocytes elevation > 12 G/l), or radiological signs (alveolar infiltrates, condensations, nodes) of infection needing treatment.
M-D-S classification definition and rules of scoring
We collected bronchoscopy reports (text and pictures if available) at regular times: day 1, day 7 (±1 day), day 14 (±2 days), day 30 (±7 days), 3 months (±1 month), 6 months (±2 months), and 12 months (±3 months) after lung transplantation. Two independent physicians scored each anastomoses according to the bronchoscopy reports in M-D-S classification, routinely used in our department since 2014. 3 Score 0 corresponds to normal score (normal anastomose scored M0D0S0). The detailed classification is provided in the Supplemental Material. In case of discordant classification between the two bronchoscopists, the anastomoses were re-sorted until mutual agreement.
We chose to define severe anastomotic complications as follows, regarding usual evolution of these endoscopic aspects toward symptoms:
Severe bronchial anastomotic necrosis as M3c or M3d (named ⩾ M3c) scoring;
Stenosis D2 ⩾ 33% to exclude malacia and mild stenosis < 33%;
Dehiscence ⩾ S1 (S0 being normal).
Survival was evaluated by June 1, 2018.
Data analysis
Quantitative data are expressed as median ± interquartile range. Nonparametric two-sided tests, such as the Fisher’s exact test and the Mann–Whitney U test, were used as appropriate. A p-value less than or equal to 0.05 was considered significant.
The analyses of long-term outcomes were performed with the use of the Kaplan–Meier estimator. A first selection of covariates was performed with the log-rank test (p < 0.20). Then, a Cox model was estimated with a backward procedure performed manually variable by variable with the use of a Wald test (p < 0.05). This procedure allows the identification of possible confounding factors (variation of regression coefficients > 20%). Hazards proportionality was checked by plotting log-minus-log survival curves and by testing the scaled Schoenfeld residuals. Time-dependent coefficients were used for nonproportional covariates. In the analysis of time to death, SAC were considered as time-dependent covariates with the use of an extended Cox model.
The following preoperative data were considered as possible correlates of SAC or patient death: donor ages (years), donor gender, mechanical ventilation duration of donor (days), donor PaO2/FiO2 ratio before explantation, donor bacterial lung infection, recipient age (years), recipient gender, recipient transplant etiology, recipient body mass index, recipient fungal and bacterial colonization, recipient FEV1 at 1 year, recipient diabetes, tracheostomy, recipient mechanical ventilation (days), thymoglobulin induction, and recipient preoperative cardiopulmonary bypass.
Statistical analyses were performed with the use of version 4.0.3 of R software.
Results
SAC characteristics
From 2010 to 2016, 145 patients were transplanted in our institution. Death within 30 days post transplantation were excluded (no one was attributed to anastomotic complication). Overall, 121 patients (237 anastomoses) were included (Figure 1).

Flowchart of patients screened during the study period, excluded and finally included, with the repartition of patients with and without SAC.
SAC occurred 32 patients (26.5%) concerning 44/237 (18.5%) anastomoses (15 localized on the left side and 29 on the right side).
The worst endoscopic evaluation for each side is described in Table 1, associated with the complication rate of each staging. Bronchial anastomotic necrosis ⩾ M3c occurred in 46.2% of patients (56/121), of whom 53.6% (30/56) induced a symptomatic complication (stenosis of dehiscence). Stenosis occurred in 47/121 patients, and the symptomatic stenosis ⩾ D2 in 23.7% (29/121) [endoscopic stenosis ⩾ D2 in 38.0% (46/121)] and symptomatic dehiscence ⩾ S1 in 2.5% (3/121) of them [endoscopic dehiscence ⩾ S1 in 7.4% (9/121)].
Occurrence of worst endoscopic scoring of anastomoses on M-D-S classification in the study population.

NA, not applicable.
There were 116 bilateral lung transplantations and 5 single lung transplantations (4 right and 1 left single lung transplantations). M1, D1b, D1c, D2c, D3c, and S2f stages are not shown because no patient was concerned by these stages. For M-D-S classification detail, see on the “Method” section.
Patients with and without SAC are described in Table 2. The median donor age was 46 (31–55) years, with 53% males. Donors had tobacco-smoking history in 31%, with median mechanical ventilation duration of 2 (1–3) days and a PaO2/FiO2 ratio of 414 (365–467) before explantation. A lung infection was identified in 37% of donors (among the main pathogens found: 20% Streptococcus spp., 35% Staphylococcus aureus, 9% Pseudomonas aeruginosa; and 20% polymicrobial). Recipients had a median age of 38 (28–50) years, with 54.5% males. Median body mass index was 19.2 (17.6–21.9) kg/m2. Underlying respiratory disease was cystic fibrosis in 50%, lung fibrosis in 13%, chronic obstructive pulmonary disease (COPD) in 11%, alpha-1 antitrypsin deficiency in 12%, and others in 14% (bronchiectasis, pulmonary hypertension, and rare lung diseases). Immunosuppressive induction was systematic, using thymoglobulin in 63%. Surgical technique was homogeneous with continuous suture with non-absorbable material, termino-terminal anastomoses, minimizing the length of the donor bronchus. Neither tissue-covered anastomosis nor bronchial revascularization was performed. Cold ischemic time was similar in both groups [539 (428–610)].
Baseline characteristics according to groups.

AMR, antibody-mediated rejection; BMI, body mass index; CMR, cellular-mediated rejection; ECMO, extra corporal membrane oxygenation; FEV1, forced expiratory volume in 1 s; HLA, human leukocytes antigen; PGD, primary graft dysfunction; SAC, symptomatic anastomotic complication; TLC, total lung capacity.
Quantitative data are provided as median (interquartile range).
Risk factors of SAC
In multivariate analysis, donor bacterial lung infection [HR 2.08 (1.04–4.17), p = 0.04] and age above 50 years [HR 3.26 (1.04–10.26), p = 0.04] were associated with SAC occurrence (see Table 3).
Risk factors of SAC (multivariate analysis).

Hazard ratio is presented as: HR [confidence interval 95%]; p-value.
Survival
Cystic fibrosis etiology was associated with a better survival (Figure 2). In multivariate analysis, SAC was associated with a twofold increased risk of death [HR 2.15 (1.07–4.32), p = 0.03] (see Table 4).

Survival without SAC depending on (a) graft etiology and (b) recipient age.
Multivariate analysis for survival.
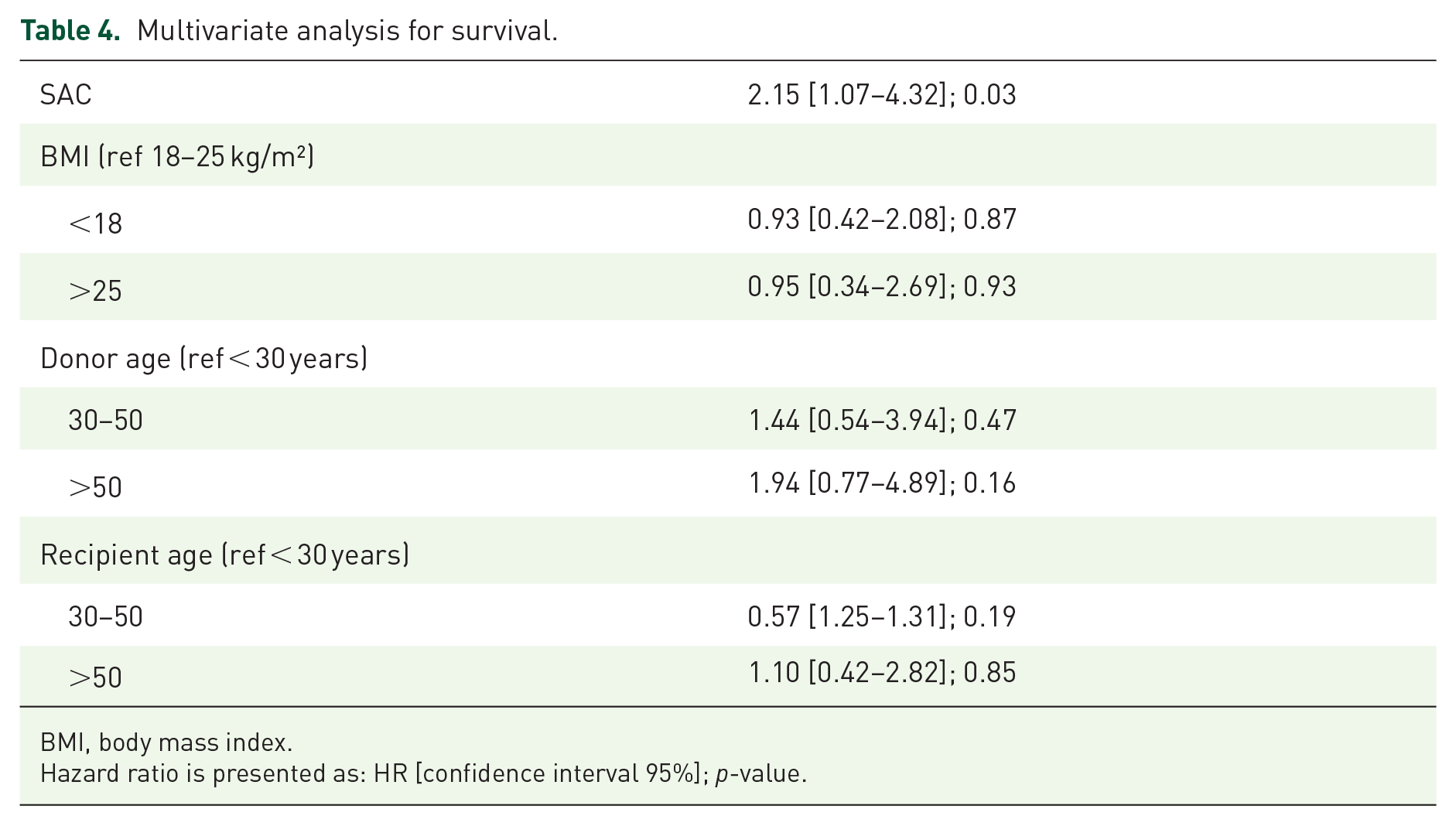
BMI, body mass index.
Hazard ratio is presented as: HR [confidence interval 95%]; p-value.
Management of SAC
Stenosis
The 29 patients developed symptomatic stenosis ⩾ D2 in median delay of 90 days (30–90). Nine patients had a single treatment: three had endoscopic desobstruction and six balloon dilatation. The remaining patients required combined therapy: 4 had endoscopic desobstruction associated with balloon dilatation, 16 had either desobstruction or balloon dilatation followed by bronchial stent placement. Endoscopy desobstruction was performed either with argon laser (eight patients), either electro cauterization (two patients) or forceps biopsy (three patients). Median time for prosthesis insertion was 6 (±4) months post lung transplantation. One patient with severe bilateral stenosis was re-transplanted 2 years after the first lung transplantation.
Dehiscence
Nine patients had dehiscences (three of them bilateral), but only three of them (2.5%) were symptomatic and primitive. Three dehiscences evolved favorably: one spontaneously (ended as a diverticulum), one with pleural drainage (accidental bronchial placement of a nasogastric tube), and one with surgery (anastomoses wrapping).
Three other dehiscences were dilatation procedure-induced leading to two fatal gaseous embolisms and one fatal hemoptysis.
The remaining three patients underwent surgery (two for anastomosis wrapping and one for anastomoses resection). Two of them had post-operative fatal hemoptysis and one had large bilateral dehiscence that would require a heart-lung transplantation that was decided against by medico-surgical staff because of altered condition.
Discussion
To our knowledge, this study is the first to use a systematic bronchoscopic evaluation to evaluate SAC incidence after lung transplantation, using the M-D-S classification. We report 26.5% of SAC (n = 32), 23.8% symptomatic stenosis ⩾ D2 requiring endoscopic procedure (n = 29), and 2.5% primitive and symptomatic dehiscence ⩾ S1 (n = 3) requiring surgery in our patients. Of note, a total of nine patients suffering from dehiscence, three experienced spontaneous resolution, three were secondary to stenosis dilatation procedure, and three were the primitive and symptomatic described above. All anastomotic complications leading to death were attributed to dehiscences.
There is still a wide variation of these rates in the literature, mainly due to the absence of consensus. Awori Hayanga et al. 4 reported a low rate of 1.4%, but they did not precisely define anastomotic complications and their data were extracted from a national register (potentially reporting the most severe complications only). In a study conducted between 2005 and 2013, that is, before the publication of the M-D-S, Yserbyt et al. 6 described 11% of anastomotic complications, but no clear definition was provided. Olland et al. 11 reported 20% of anastomotic complications after lung transplantation and Cho et al. 5 reported 28% of early and 16% of delayed anastomotic complications in their cohorts.
Based on our data, we identified several risk factors of anastomotic complications after lung transplantation. Among them, donor bacterial lung infection [HR 2.08 (1.04–4.17), p = 0.04] is an interesting risk factor since being the only alterable one. To manage that, ex vivo lung perfusion could help physicians to better identify atelectasis versus pneumonia in donor when CT-scan is confusing and could save time needed for bacteriological bronchoscopic results. We started to use this procedure in 2018 in our center, that is, after the end of this study. In case of confirmed pneumonia, physicians could decide to stop procedure if pneumonia gets worse during the ex vivo lung perfusion. Of note, no study ever reported this risk factor. 1 We can hypothesize that donor lung infection induces local inflammation that alters and delays healing of bronchial mucosa and worsens ischemia. Older recipient age (>50 versus <30 years) [HR 3.26 (1.04–10.26), p = 0.04] and non-cystic fibrosis etiology (Kaplan–Meier survival curves without SAC, p < 0.001) were two other factors associated with a higher risk of SAC. Despite of numerous comorbidities (nutritional status, bacterial and fungal colonization), 12 cystic fibrosis was not a risk factors of SAC, probably because of the younger age of patients and their better vascularization which probably play a key role in anastomosis healing. Non-cystic fibrosis group includes several etiologies, mostly COPD, emphysema, and pulmonary fibrosis, which have already been identified as an ‘at-risk’ group: they are older with altered vascularization, especially in previous smokers patients. 11
In our study, surgical technique was homogeneous, using termino-terminal anastomosis without recovery strategy or bronchial reimplantation, as recommended. 13 We used non-absorbable material, as opposed to Weder et al., 14 who observed no significant dehiscence in a cohort of 441 anastomosis. Cold ischemic time was not associated with a higher risk of SAC, as previously described.1,4,6
Few studies reported the impact of SAC on survival. Our study found that SAC occurrence was independently (adjusted on BMI, donor and recipient ages) associated with a twofold increased risk of death [HR 2.15 (1.07–4.32)]. In a retrospective analysis of 94 anastomotic complication in 48 patients, Murthy et al. reported an equivalent early survival in patients with treated complication compared with patient without anastomotic complication (80 versus 82%, p = 0.9) but worse late survival at 4 years (27 versus 60%, p = 0.03). To the opposite, patients with an untreated complication had a worse early survival (662 versus 82%, p = 0.004) without difference in late survival. 15 We can hypothesize dehiscence provided early mortality and stenosis delayed survival impact.
In our study, all SAC were treated, whereas Yserbyt et al. 6 reported that only 25% of their anastomotic complications were actively treated. Among untreated anastomotic complications, they observed only 7% of secondary degradation and 7% of altered functional respiratory test. From our point of view, mechanical complications, such as lung infections, dyspnea because of the reduced bronchial diameter, and atelectasis, justify early intensive treatment to prevent side effects of chronic infections, such as bronchiectasis.
Our study is limited by its retrospective nature, leading to missing data. Another limitation is its reproducibility because of a high proportion of cystic fibrosis patients and the frequent thymoglobulin induction that was used in our center even without prior immunization. For bronchoscopy classification, twofold independent reading was performed, with an examination of non-conformity and new readings for agreement. The International Society for Heart and Lung Transplantation (ISHLT) classification was published during our study. 1 Because our team, as with all French ones, was familiar with the M-D-S classification for years, we refrained from using a new classification that could have induced incorrect a posteriori coding in our inexperienced group. We precisely defined anastomotic complications with M-D-S classification and distinguished the symptomatic ones, which is often missing in most studies. Each parameter was well described and analyzed to give an overview of anastomotic complications.
Conclusion
SAC still occurred in 26.5% (n = 32) of patients after lung transplantation. We report twofold increased risk of death in patients with SAC. Donor bacterial lung infection, non-cystic fibrosis etiology, and older recipient age were associated with an increased risk of SAC. Based on these findings, careful evaluation of potential donor lung infection and endoscopic monitoring, especially in older recipient, are needed.
Survival presented as Kaplan–Meier curve, p < 0.001.
Supplemental Material
sj-docx-1-tar-10.1177_17534666221110354 – Supplemental material for Incidence and risk factors of anastomotic complications after lung transplantation
Supplemental material, sj-docx-1-tar-10.1177_17534666221110354 for Incidence and risk factors of anastomotic complications after lung transplantation by Agathe Delbove, Thomas Senage, Pierre Gazengel, Adrien Tissot, Philippe Lacoste, Laurent Cellerin, Christian Perigaud, Isabelle Danner-Boucher, Arnaud Cavailles, Thierry Lepoivre, Antoine Mugniot, Johanna Nicolet, Delphine Horeau-Langlard, Nicolas Groleau, Yannick Fedun, Bertrand Rozec, Antoine Magnan, Jean-Christian Roussel and François-Xavier Blanc in Therapeutic Advances in Respiratory Disease
Footnotes
Acknowledgements
The authors thank Mrs Aurore Foureau (Lung O2 cluster for research, Nantes) for helping in designing and writing the study protocol and Mrs Alison Mc Lean, Medical Librarian at Vannes hospital, for proofreading the English version.
Declarations
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.