
Abstract
Background:
Severe asthma increases the risk of severe COVID-19 outcomes such as hospitalization and death. However, more studies are needed to understand the association between asthma and severe COVID-19.
Methods:
A cohort of 150,430 adult asthma patients were identified in the Swedish National Airway Register (SNAR) from 2013 to December 2020. Data on body mass index, smoking habits, lung function, and asthma control test (ACT) were obtained from SNAR, and uncontrolled asthma was defined as ACT ⩽19. Patients with severe COVID-19 were identified following hospitalization or in death certificates based on ICD-10 codes U07.1 and U07.2. The Swedish Prescribed Drug register was used to identify comorbidities and data from Statistics Sweden for educational level. Multivariate logistic regression analyses were used to estimate associations with severe COVID-19.
Results:
Severe COVID-19 was identified in 1067 patients (0.7%). Older age (OR = 1.04, 95% CI = 1.03–1.04), male sex (1.42, 1.25–1.61), overweight (1.56, 1.27–1.91), obesity (2.12, 1.73–2.60), high-dose inhaled corticosteroids in combination with long-acting β-agonists (1.40, 1.22–1.60), dispensed oral corticosteroids ⩾2 (1.48, 1.25–1.75), uncontrolled asthma (1.64, 1.35–2.00), cardiovascular disease (1.20, 1.03–1.40), depression (1.47, 1.28–1.68), and diabetes (1.52, 1.29–1.78) were associated with severe COVID-19, while current smoking was inversely associated (0.63, 0.47–0.85). When comparing patients who died from COVID-19 with those discharged alive from hospital until 31 December 2020, older age, male sex, and current smoking were associated with COVID-19 death.
Conclusion:
Patients with uncontrolled asthma and high disease burden, including increased asthma medication intensity, should be identified as risk patients for severe COVID-19. Furthermore, current smoking is strongly associated with COVID-19 death in asthma.
Background
At an early stage in the coronavirus disease-19 (COVID-19) pandemic, several diseases including diabetes, hypertension, and cardiovascular disease were identified as risk factors of worse COVID-19 outcome.1,2 Although a few studies have reported a prevalence of asthma up to 14% in hospitalized COVID-19 patients and asthma as risk factor for hospitalization,3,4 there is growing evidence that asthma does not increase the risk of acquiring COVID-19. 5 In Sweden, the frequency of severe COVID-19 in asthma has been relatively low, 6 and several meta-analyses show that patients with asthma are not at risk of severe COVID-19-related outcomes such as hospitalization, intensive care, or mortality.7,8 It has even been speculated that inhaled corticosteroid treatment might have a protective effect against COVID-19. 9
Despite the low risk of patients with asthma of acquiring the infection,5,6 studies are indicating that severe asthma and non-allergic asthma can increase the risk of severe COVID-19-related outcomes.10–12 Yet, there is need for further studies in larger asthma cohorts on factors associated with severe COVID-19 in asthma. These factors could be important when identifying patients at risk of COVID-19 and developing guidelines in asthma-related COVID-19 care. The current study is based on a large and well-characterized cohort of patients with physician-diagnosed asthma within the Swedish National Airway Register (SNAR).6,13,14 In this cohort, patients hospitalized or who died from COVID-19 have been identified, giving a unique opportunity to study the burden of asthma and its association with severe COVID-19.
Methods
Study population
The Swedish National Airway Register
SNAR is a national quality register launched in 2013 and includes data on patients from primary and secondary care with a physician diagnosis of asthma (children and adults) or chronic obstructive pulmonary disease (COPD).6,13,14 In this study, we included adult patients (⩾18 years) with asthma diagnoses (International Classification of Diseases, version 10; ICD-10 J45) identified in extracted data from SNAR on 1 February 2020. Patients with COPD diagnosis (ICD-10 J44) were excluded from the study population.
Severe COVID-19 detected by national registers
As cases, we identified asthma patients with severe COVID-19 by linking data extracted from SNAR with data obtained up to 31 December 2020 from the National Patient Register (NPR), the Swedish Intensive Care Registry (SIR), and the Swedish Cause of Death Register (SCDR). 15 Those registers provide data about COVID-19 based on the ICD-10 codes U07.1 (COVID-19 confirmed by laboratory testing) and U07.2 (COVID-19 clinically or epidemiologically diagnosed, but laboratory testing is inconclusive or not available). Severe COVID-19 was defined as inpatient care identified as primary discharge diagnosis in NPR or care at the intensive care unit in SIR, or COVID-19 death registered as an underlying cause of death in SCDR. The asthma patients without severe COVID-19 were defined as controls.
Definitions
Clinical data
Clinical data were obtained from SNAR including the latest uploaded information about body mass index (BMI), smoking habits, Forced Expiratory Volume in 1 s as percent of predicted value (FEV1%), and Asthma Control Test (ACT). BMI was used as a continuous variable but also categorized as underweight (BMI <19), normal weight (BMI 19–25), overweight (BMI 26–30), and obese (BMI > 30). Smoking was categorized as current smokers, ex-smokers (including those who quit smoking during the last 6 months), and non-smokers. The Swedish reference values by Hedenström were used to calculate FEV1% predicted,16,17 and if post-values were missing, pre-values were used. ACT scores were used as a continuous variable (range, 5–25; poor control to complete control), and ACT ⩽19 was used to define uncontrolled asthma. 18
Data on asthma medications
Data on dispensed asthma medications between 1 January 2019 and 28 February 2020 were retrieved from the Swedish Prescribed Drug Register (SPDR) 14 using Anatomical Therapeutic Chemical (ATC) codes. Asthma medication was classified as short-acting β-agonists (SABA) (R03AC02-03), short-acting muscarinic antagonists (SAMA) (R03BB01), long-acting β-agonists (LABA) (R03AC12,13,18,19), long-acting muscarinic antagonists (LAMA) (R03BB04-07), inhaled corticosteroids (ICS) (R03BA), LABA-LAMA combinations (R03AL03-07), LABA-ICS combinations (R03AK), LABA-LAMA-ICS combinations (R03AL08,09,11,12), leukotriene antagonists (LTRA) (R03DC03), acetylcysteine (R05CB01), and oral corticosteroids (OCS) (H02AB01,02,06). OCS were classified into ⩾1 and ⩾2 dispensations. Based on the different ATC codes, and a 4-month dispensed coverage of single or combination medication, dispensed inhaled medications were further divided into groups: (1) SABA and/or SAMA only, (2) ICS only, (3) LABA-ICS, (4) LABA-LAMA-ICS, and (5) other inhaled medication, that is, LABA only, LAMA only, or LABA-LAMA. Dispensed high-dose ICS were defined according to the Global Initiative for Asthma (GINA) guidelines. 5
Data on level of education, asthma healthcare utilization, and comorbidities
Data on level of education were obtained from Statistics Sweden 19 and classified into primary school (usually 9 years), secondary school (usually 12 years), and tertiary education (longer than 12 years). Prior inpatient or secondary care due to asthma was identified from the NPR, defined as patients who had been hospitalized or had a secondary care visit in 2019 with a primary ICD-10 code for asthma (J45 or J46). Medication-treated comorbidities were identified through the SPDR with ATC codes for dispensed medication between 1 January 2019 and 28 February 2020 and classified into cardiovascular disease (C01-03, C08, C09), depression (N06), diabetes (A10A, A10B), and rhinitis (R01A).
Statistical analyses
Data analyses were conducted using SAS 9.4 for Windows (SAS Institute Inc, Cary, NC, USA). Baseline data of cases and controls were expressed as means, standard deviations (SD), and percentage of relative frequencies. For comparative analyses between the cases and controls, t-tests were used for continuous data and Chi-square tests for categorical data. All p-values <0.05 were considered statistically significant. Odds ratios (OR) and 95% confidence intervals (CI) were generated using multivariable logistic models, with severe COVID-19 as a dependent variable. Independent variables were age, sex, level of education, BMI, smoking habits, FEV1% predicted, ACT scores ⩽19, asthma medication (high-dose ICS in combination with LABA and OCS), prior asthma inpatient/secondary care, and concomitant comorbidities (cardiovascular disease, depression, diabetes, and rhinitis). Missing values were handled in two ways: missing as a separate category (Model 1) and a complete case analysis (Model 2). 20 We further explored factors associated with COVID-19-related death by comparing patients dying from COVID-19 with those discharged from hospital alive. This analysis was conducted with COVID-19 death as the dependent variable and the same covariates as described above.
Ethics
The study complies with the Declaration of Helsinki and was approved by the Swedish Ethical Review Authority (2020-02777).
Results
Up to 31 December 2020, 150,430 living adult asthma patients in SNAR were identified, of whom 1067 (0.7%) fulfilled the definition of severe COVID-19. In total, 875 patients were identified following hospitalization due to COVID-19 (n = 777 NPR and n = 98 NPR and SIR) and an additional 192 patients were identified in death certificates (SCDR) (Figure 1). A majority of cases, 1059 (99%), were confirmed by laboratory testing (ICD-10 U07.1).

Flow chart of the study population.
Basic characteristics of cases with severe COVID-19 and controls
Older age (mean 65.5 years versus 50.6 years, p < 0.001), male sex (42.5% versus 39.0%, p = 0.021), higher BMI (mean 30.9 versus 27.8, p < 0.001), lower FEV1% predicted (mean 79.0% versus 85.4%, p < 0.001), and lower ACT scores (mean 18.2 versus 19.9, p < 0.001) were more common among cases than controls. The proportion of patients with primary education was higher among cases (54.3% versus 40.1%, p < 0.001), while a lower proportion of cases were current smokers (4.5% versus 10.1%, p < 0.001) (Table 1).
Basic characteristics of asthma patients with and without severe COVID-19.

ACT, asthma control test; BMI, body mass index; FEV1, forced expiratory volume in 1 s.
Dispensed ICS-LABA (50.2% versus 37.2%, p < 0.001), ICS-LABA-LAMA (5.3% versus 2.4%, p < 0.001), and high-dose ICS in combination with LABA (32.7% versus 19.4%, p < 0.001) were more common in cases than controls, while no asthma medication at all, SABA or SAMA only, and the use of ICS only were more common among controls. In addition, cases were more often dispensed LTRA (17.7% versus 10.9%, p < 0.001) and OCS (30.8% versus 20.2%, p < 0.001), and prior asthma inpatient or secondary care in 2019 were also more common in cases (8.6% versus 4.5%, p < 0.001). Medications for comorbidities were more common in cases than controls: cardiovascular disease (59.9% versus 30.4%, p < 0.001), depression (29.1% versus 19.1%, p < 0.001), diabetes (20.4% versus 7.5%, p < 0.001), and rhinitis (25.2% versus 22.3%, p = 0.022) (Table 2).
Asthma medication, comorbidities, and asthma healthcare utilization in patients with and without severe COVID-19.

ICS, inhaled corticosteroids; LABA, long-acting beta-agonists; LAMA, long-acting muscarinic antagonists; LTRA, leukotriene receptor antagonists; NS, non-significant; OCS, oral corticosteroids; SABA, short-acting beta-agonists; SAMA, short-acting muscarinic antagonists.
LABA only, or LAMA only, or LABA-LAMA, respectively.
Associations with severe COVID-19
A multivariable logistic regression model with missing values as a separate category showed that overweight (OR = 1.56, 95% CI = 1.27–1.91), obesity (OR = 2.12, 95% CI = 1.73–2.60), uncontrolled asthma (OR = 1.64, 95% CI = 1.35–2.00), high-dose ICS in combination with LABA (OR = 1.40, 95% CI = 1.22–1.60), OCS ⩾2 (OR = 1.48, 95% CI = 1.25–1.75), prior asthma inpatient or secondary care (OR = 1.42, 95% CI = 1.13–1.79), cardiovascular disease (OR = 1.20, 95% CI = 1.03–1.40), depression (OR = 1.47, 95% CI = 1.28–1.69), and diabetes (OR = 1.52, 95% CI = 1.29–1.78) were associated with severe COVID-19, also when adjusted for older age and male sex. Current smoking was inversely associated with severe COVID-19 (OR = 0.63, 95% CI = 0.47–0.84) (Table 3, Model 1). The results were similar in a complete case analysis, although concomitant cardiovascular disease was not significant (Table 3, Model 2).
Multivariable logistic models: independent predictors of severe COVID-19 in asthma..

ACT, asthma control test; BMI, body mass index; CI, confidence intervals; FEV1, forced expiratory volume in 1 s; ICS, inhaled corticosteroids; LABA, long-acting beta-agonists; NA, not applicable due to few cases; OCS, oral corticosteroids; OR, odds ratios.
In Model 1, missing was handled in separate categories (n = 150,430), while Model 2 was conducted as a complete case analysis (n = 52,135).
Entered as a continuous variable.
Associations with COVID-19 death
In a multivariable logistic regression model, comparing those who died from COVID-19 (n = 192) with those discharged alive from hospital (n = 875), older age (OR = 1.12, 95% CI = 1.09–1.13), male sex (OR = 1.89 95% CI = 1.24–2.78), and current smoking (OR = 5.35 95% CI = 2.29–12.48) were associated with COVID-19 death when adjusted for covariates (Figure 2).
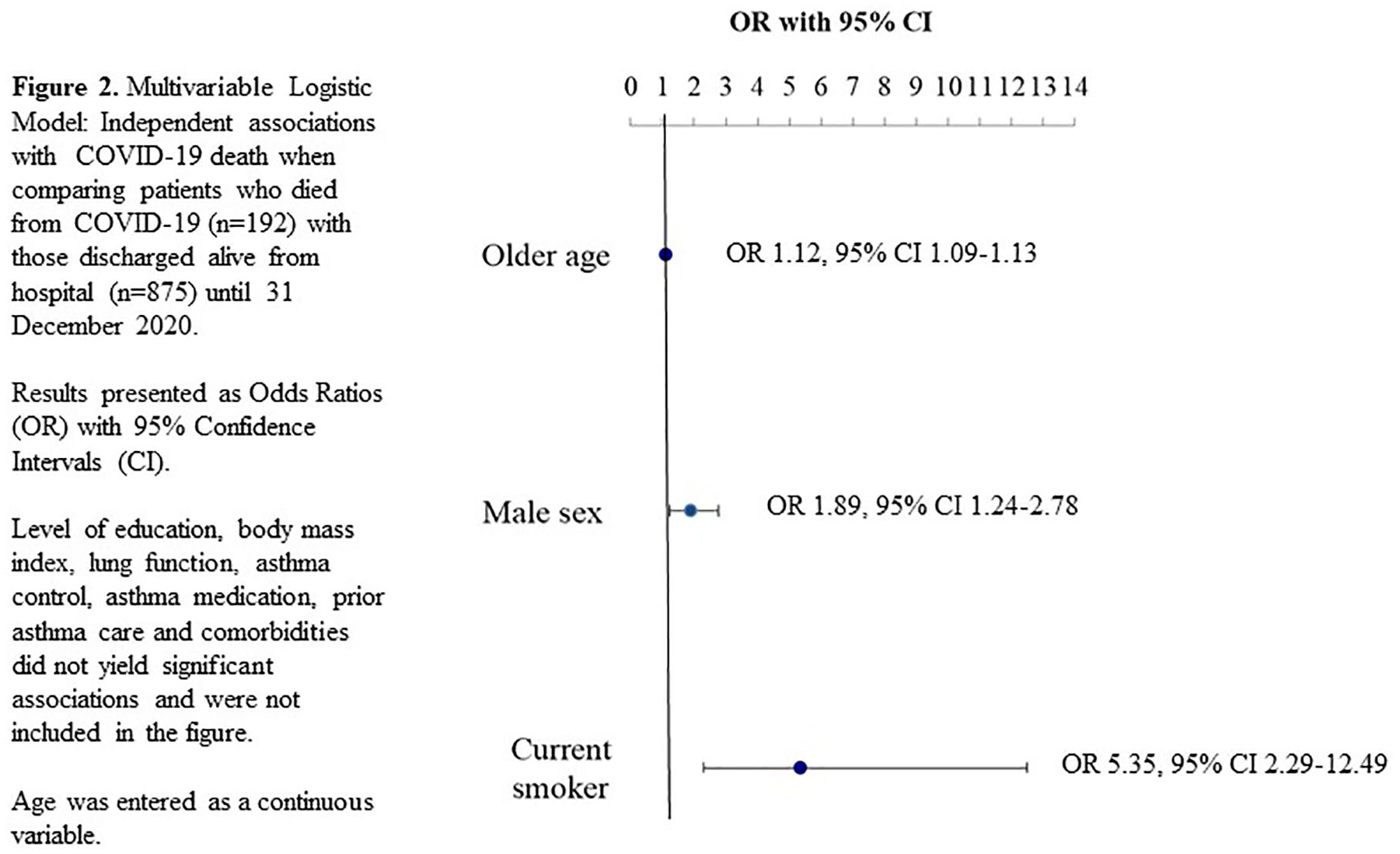
Multivariable logistic model.
Discussion
In this large register-based Swedish asthma cohort, asthma-related factors such as uncontrolled asthma increased asthma medication intensity, and prior asthma healthcare utilization was associated with severe COVID-19. In addition, known risk factors in the general population such as male sex, older age, obesity, cardiovascular disease, and diabetes were associated with severe COVID-19. Surprisingly, current smoking was inversely associated with severe COVID-19 but was identified as a predictor for COVID-19 death together with male sex and older age.
While severe COVID-19 was more common among patients with decreased lung function and lower level of education, these factors were not associated with severe COVID-19 in the adjusted models. However, it has been reported that patients with uncontrolled asthma have an increased risk of more severe viral exacerbations. 21 In the light of our results, it is now evident that uncontrolled asthma, defined as an ACT score of ⩽19, and a high disease burden are associated with severe COVID-19. We used dispensed asthma medication, prior asthma inpatient or secondary care, and the use of OCS to determine a high disease burden. Our result is consistent with previously reported associations between COVID-19 and a severe asthma.10,11,22–24 Zein et al. 11 showed that severe asthma, based on GINA treatment steps 3 and 4, influenced the association with COVID-19-related outcomes such as hospitalization and admission to the intensive care unit (ICU). Also reported from the United States is an increased risk of severe COVID-19-related outcomes in asthma patients who required clinical asthma care during the last year before the COVID-19 diagnosis. 22 In a study from the United Kingdom, an increased risk of COVID-19 related hospital death in asthma patients who recently had been prescribed OCS was observed, 23 and worse COVID-19 outcome (death, ICU care, or need for ventilation) in patients with severe asthma was found in Italy. 24 All these factors are relevant aspects to consider when identifying patients at risk of severe COVID-19.
During the pandemic, the GINA guidance has recommended that patients should maintain their controller medication, both ICS alone and ICS in combination with LABA. If necessary, OCS should also be prescribed to achieve good asthma control. 5 The issue whether ICS can modify the risk of severe COVID-19 in asthma patients has been of major concern ever since the first wave of the pandemic, 9 and an association with ICS use and increased risk of upper respiratory infections has been previously reported. 25 Yet, early pandemic reports indicated a low prevalence of asthma among severely affected COVID-19 patients, arising the question whether ICS indeed could have a protective effect. 9 However, over time, several studies have reported a lack of association between ICS use and the risk of severe COVID-19-related outcomes.26,27 Similar to our study, others have shown an increased risk of death in asthma patients on high-dose ICS compared with SABA only. 28 Importantly, these results might reflect patients with severe asthma in need of higher doses of ICS and need for increased asthma medication intensity, rather than an ICS-mediated effect.
In the general population as well in asthma patients, obesity is a known risk factor for severe COVID-19.4,29 In our study, it was clear that overweight patients with asthma had an increased risk of contracting severe COVID-19. Importantly, BMI is a factor that affects the level of asthma control, 30 and several possible mechanisms link a higher BMI to uncontrolled asthma. First, it may be due to systemic inflammation in obese, the overweight influencing lung mechanics and metabolic factors. 31 Second, it has been reported that obese patients with asthma are less responsive to corticosteroid therapy and are exposed to a more disease-related severe outcome. 32 Higher BMI in asthma is often linked to the non-allergic phenotype, 32 and studies from the UK biobank and South Korea have investigated asthma phenotypes and COVID-19 outcomes.12,33 In both studies, patients with non-allergic asthma had worse clinical outcomes, whereas there was no association between severe COVID-19 and allergic asthma. This supports the lack of association between dispensed medication for rhinitis and severe COVID-19 in our study. However, there is still limited research about different asthma phenotypes and COVID-19, which needs to be further studied.
Smoking is a well-known risk factor of respiratory complications, and meta-analyses have shown that current smokers have an increased risk of worse COVID-19 prognosis than never smokers. 34 On the contrary, in a large Swedish population–based study, no association was found between current smoking and COVID-19 hospitalization or death. 35 Surprisingly in our study, current smoking was an inverse predictor of severe COVID-19, and the same trend has been shown in a cohort of patients with COPD. 36 We can speculate that our results could be related to protective strategies, that is, current smokers with asthma might have followed basic infection-control measures such as social distancing, especially during the first months of the pandemic, thereby reducing the risk of the infection. However, in our analysis of fatal outcomes, current smoking was a strong predictor for death, also shown by others. 37 This highlights the importance of smoking cessation support among current smokers with asthma.
In our study, we identified cardiovascular disease and diabetes as comorbidities associated with severe COVID-19. These are the same risk factors of severe COVID-19 previously reported in the general population1,2 and in asthma patients.29,38 An interesting finding was the association between depression and severe COVID-19, which might be related to the close relationship between depression and poor asthma control.39,40
Strengths and limitations
A major strength of our study is the large database of SNAR with well-characterized physician-diagnosed asthma patients and that patients with a concomitant COPD diagnosis were excluded. Furthermore, the possibility to link SNAR with other national registers allows studying severe COVID-19 among asthma patients in Sweden. In a registry study, we can reduce the risk of collider bias compared with hospital-based observational studies on COVID-19. 41 An important limitation, in relation to the use of register-based studies with clinical data from healthcare, is the variable amount of missing data. The associations between severe COVID-19 and missing data on BMI, lung function, and ACT scores indicate selection bias. A further limitation was lack of data on pack-years, since others have shown a dose–response association between pack-years and adverse COVID-19 outcomes. 42 To handle missing data, we conducted different multivariable models to validate our result. Furthermore, data on asthma medication are based on dispensed medications from Swedish Prescribed Drug Register, which have some limitations: (1) Patients with severe asthma cannot be identified when linking data. Thus, we used the term ‘a high symptom burden’ as a proxy for severe or difficult-to-treat asthma. (2) We also lack data on adherence, and therefore the ICS dose can be under- or overestimated. (3) Dispensed OCS and dispensed medication for rhinitis could be related to other conditions than asthma exacerbations or allergic rhinitis. (4) Data do not cover all comorbidities and therapies that could affect the risk of COVID-19.
Conclusion
Apart from known risk factors in the general population such as older age, male sex, obesity, cardiovascular disease, and diabetes, we identified uncontrolled asthma and a high disease burden including increased asthma medication intensity to be associated with severe COVID-19. Current smoking was an inverse predictor for severe COVID-19, but an analysis on fatal outcomes showed that current smoking was associated with COVID-19 death. Our results highlight the importance of identifying and optimizing treatment for patients with uncontrolled asthma. Equally important, for the asthma patient in general, is to maintain good symptom control and thereby reduce the risk of severe COVID-19. Furthermore, smoking cession support is essential also in relation to the risk of COVID-19 death.
Footnotes
Acknowledgements
Special thanks to Caddie Zhou for statistical analyses. Further acknowledgements are given to all the patients and healthcare professionals who contributed to registrations in SNAR and to the steering committee and register coordinators. Thanks also to the Centre of Registers Västra Götaland for infrastructure and data management support.
Author contributions
Conflict of interest statement
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: CS has served in an advisory board and/or participated in education arranged by AstraZeneca, Boehringer-Ingelheim, and Novartis. LV has received grants and personal fees from AstraZeneca and personal fees from GSK, Novartis, Boehringer-Ingelheim, Menarini, Resmed, Chiesi, AGA Linde, and Pulmonx. TS has received personal fees from ALK Abello for lectures at sponsored meetings. AL has received personal fees from AstraZeneca, Novartis, Boehringer-Ingelheim, and GlaxoSmithKline for advisory boards and/or lectures at sponsored meetings. AT has received personal fees from AstraZeneca, Novartis, Boehringer-Ingelheim, and GlaxoSmithKline for advisory boards and/or lectures at sponsored meetings. FN was an employee of AstraZeneca until 2019 and holds some AstraZeneca shares. JRK, SAF, CP, YS, JS, AEJ, and JKS have no conflicts of interest.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Swedish Heart-Lung Foundation under Grant 20200308 and The Asthma and Allergy Association.