
Abstract
Background:
Tuberculosis (TB) is a constant threat even with a worldwide active public health campaign. Diagnosis of TB pleurisy is challenging in the case of pleural effusion of unknown origin after aspiration analysis. The study was designed to demonstrate a simple image interpretation technique to differentiate TB pleurisy from non-TB pleurisy using semi-rigid pleuroscopy.
Methods:
The study retrospectively enrolled 117 patients who underwent semi-rigid pleuroscopy from April 2016 to August 2018 in a tertiary hospital. We analyzed the possibility of TB pleurisy using three simple pleuroscopic images via semi-rigid pleuroscopy.
Results:
Among 117 patients, 28 patients (23.9%) were diagnosed with TB pleurisy. Sago-like nodules/micronodules, adhesion, and discrete distribution were noted in 20 (71.4%), 20 (71.4%), and 19 (67.9%) patients with TB pleurisy, respectively. Sago-like nodules/micronodules, adhesion, and discrete distribution were noted in six (6.7%), 37 (41.6%), and no (0.0%) patients with non-TB pleurisy, respectively. The positive and negative predictive values of any two out of three pleuroscopic patterns for TB pleurisy were 100.0% and 93.7%, respectively.
Conclusions:
A high positive predictive value for TB pleurisy was demonstrated by the presence of any two out of the three characteristic features. Absence of all three features had an excellent negative predictive value for TB pleurisy. Our diagnostic criteria reconfirm that pleuroscopic images can be used as predictors for TB pleurisy in patients with undiagnosed pleural effusion.
The reviews of this paper are available via the supplementary material section.
Introduction
Despite the aggressive public health strategy and effective treatments against tuberculosis (TB), it remains a major infectious cause of death worldwide, with 9 million new cases and nearly 2 million deaths annually. 1 Tuberculous pleural effusion is a common manifestation of extra-pulmonary TB and is the leading cause of pleural effusion in some geographical areas.2–5 The incidence of TB pleurisy as a manifestation of extrapulmonary TB is 23–66%. 6 In contrast, TB accounts for 25–44% of all cases of pleural effusion. 3
The early diagnosis of TB pleurisy is crucial for a favorable clinical outcome. A previous study reported that prognosis was worse if effective anti-TB treatment was delayed even by a duration of 2 weeks after the first visit. 7 A time-consuming diagnostic process is the major cause of delay in effective anti-TB treatment in the early stage of the disease. Conventional diagnostic tests include microscopic examination of the pleural fluid for acid-fast bacilli (AFB); mycobacterial culture of the pleural fluid, sputum, or pleural tissue; and pathological examination of the pleural tissue for granulomatous inflammation. Microscopic examination of the pleural fluid is positive for AFB in less than 5% of cases due to the paucibacillary nature of the disease,8,9 while mycobacterial culture of the pleural fluid is time-consuming and has low sensitivity (24–58%).9,10 Biopsy of the pleural tissue for combined histological examination and mycobacterial culture of the pleural fluid and tissue is the most sensitive method among currently available methods. 11 The levels of adenosine deaminase (ADA) in pleural fluid have high sensitivity and specificity in the diagnosis of TB pleurisy.12,13 However, the use of ADA may not be widely available in developing countries.
In clinical practice, undiagnosed pleural effusion is frequently encountered even after thoracentesis and closed tube biopsy. The possible causes for undiagnosed pleural effusion include malignancy, TB, infection and inflammation. 14 Therefore, invasive procedures for biopsy under direct visualization via pleuroscope are employed to reach the diagnosis. Recent evidence suggests that a semi-rigid pleuroscope is an effective diagnostic tool for undiagnosed pleural effusion. 14 Semi-rigid pleuroscopy is conducted by a non-surgical pulmonologist in the endoscopy suite, with patients under local anesthesia and conscious sedation. The diagnostic yield of closed tube biopsy ranges from 50% to 60%. 11 Pleuroscopy has been demonstrated to improve the diagnostic accuracy of TB pleurisy 15 in undiagnosed pleural effusion. The improved diagnostic yield of semi-rigid pleuroscopy is mostly due to examination of the pleural lesion and guides the biopsy of abnormal pleural lesions. Apart from its role in improving the diagnostic yield of TB pleural disease, abnormal pleural lesions can be observed directly under the pleuroscope. Several characteristic patterns could be observed in the pleuroscopic examination. 16 By identifying the characteristic features of TB pleurisy, precise biopsy of the targeted lesion may increase the diagnostic yield rate and reduce the duration of the procedure. In addition, tissue culture for mycobacterial detection and drug sensitivity test can be performed using this procedure. The aim of the present study was to investigate the sensitivity and sensitivity of three characteristic features observed under semi-rigid pleuroscopy for the diagnosis of TB pleural effusion.
Methods
Patients
The present study was approved by the Institutional Review Board (IRB) of Chang Gung Memorial Foundation (IRB no.: 201902075B0). We retrospectively recruited 120 patients from April 2016 to August 2018 at Linkou Chang Gung Memorial Hospital, Taiwan, which is a tertiary referral medical center. Consecutive patients who underwent semi-rigid pleuroscopy within the study period were identified from the database and their demographic characteristics were recorded. Among the 120 patients who received pleuroscopy, three patients were excluded due to failure in biopsy. The causes for failure of biopsy were severe adhesion without enough explored view (n = 1), the presence of bronchopleural fistula (n = 1), and severe cough during the pleuroscopy procedure (n = 1). Therefore, a total 117 patients were recruited for final analysis.
Diagnostic criteria of TB pleurisy
Patients with TB pleurisy were defined according to a previous study. They included patients with confirmed as well as probable TB pleurisy. 17 A patient with confirmed TB pleurisy was defined as a patient with a pleural fluid sample that was culture-positive for Mycobacterium tuberculosis and/or a histopathological finding consistent with TB on pleural biopsy. A patient with probable TB pleurisy was defined as a patient with at least one of the following characteristics: (a) sputum specimen that was culture-positive for M. tuberculosis; (b) other biological specimens that were culture-positive for M. tuberculosis; (c) raised pleural lymphocytes and protein levels; and (d) a positive response to anti-TB medication with the absence of other possible causes of pleural effusion. According to previous studies,9,10 patients with positive M. tuberculosis culture results represent a relatively small portion of all cases of TB pleurisy. The present study employed a combination of pleural M. tuberculosis culture, pleural pathological analysis, and clinical diagnosis as the reference method for diagnosing TB pleurisy. To confirm the diagnosis of TB pleurisy, two senior physicians independently reviewed each patient’s clinical and laboratory records.
Procedure and equipment
All patients underwent pleuroscopy performed by an experienced operator and two trained assistants. All patients received moderate sedation with fentanyl and midazolam with or without propofol during the procedure. Before starting the examination, chest ultrasound was performed to identify the optimal entry site with the patients in the decubitus position. After local administration of 2% lidocaine for anesthesia, a 1.0-cm skin incision was made followed by thoracotomy with an 8-mm flexible trocar (MAJ-1058, Olympus Medical Systems Corp., Japan). A semi-rigid thoracoscope (LTF-240; Olympus, Tokyo, Japan) was initially used for draining the effusion and for exploring the pleural cavity. Cryoprobe or a pair of forceps (FB-15C-1; Olympus, Tokyo, Japan) were used for biopsy through the working channel of the semi-rigid thoracoscope. A 1.9 or 2.4-mm flexible cryoprobe (Erbokryo CA, Erbe, Germany) was used to perform cryobiopsy with carbon dioxide as the cryogen. The cooling time of each cryobiopsy was approximately 3 s and the temperature of the probe tip reached approximately −70°C. At least three biopsies were considered the standard procedure in each patient. The biopsy area was restricted in parietal pleura. For histopathological analyses, all biopsy samples were transported in separate formalin containers. The biopsy samples were processed according to standard protocols for histopathological and immunohistochemical staining. After completing the biopsies, a drainage tube with a 16 Fr pigtail catheter (BT-PDS-1630-W-NK1; Bioteq, Taipei, Taiwan) was placed to monitor and drain the pleural effusion. The timing of catheter removal was decided by clinicians’ judgment based on the amount of pleural effusion (less than 50 ml) and the clinical condition.
Specimen processing
The pleural and sputum specimens were processed according to the procedure described in a previous report.
18
Briefly, pleural fluid and sputum specimens were stained with Ziehl–Neelsen stain for microscopic examination. Decontamination was performed using N-acetyl-
Image analysis
Each pleuroscopy image was evaluated for three features, namely the character of nodules, adhesion, and the distribution of the lesions. Three characteristic features were adopted for differentiating TB pleurisy from non-TB pleurisy: (a) lesions with sago-like nodules (Figure 1A) or micronodules (Figure 1B); (b) the presence or absence of adhesion (Figure 2); and (c) the distribution of the lesions (discrete or fused together) (Figure 3). To define the absence or the presence of these three features among subjects, it took 10–15 min to make a conclusion between two senior pulmonologists. They evaluated the clinical course and discussed each pleuroscopy image to arrive at a consensus.

A representative case of tuberculosis pleurisy.

A representative case of adhesion.

A representative case of discrete distribution of lesions.
Statistical analysis
Data were expressed as mean ± standard error of the mean. Student’s t-test was used for the comparison of continuous variables between patients with TB pleurisy and those with non-TB pleurisy, while the Mann–Whitney U-test was used for non-normal distributions. Categorical variables were compared with the chi-squared test or Fisher’s exact test. Univariate logistic regression analysis with odds ratios and 95% confidence intervals (CIs) were used to assess the difference in diagnostic yields between the groups. The sensitivity, specificity, positive predictive value, and negative predictive value were expressed as 95% CIs. Statistical significance was set at p < 0.05. Statistical analyses were performed using SPSS version 13.0 (SPSS Inc.; Chicago, IL, USA).
Results
Diagnoses of pleural effusion
Among 117 patients, 28 had TB pleurisy and 89 had non-TB pleurisy. The causes for non-TB pleurisy included adenocarcinoma (n = 39), squamous cell carcinoma (n = 2), metastatic carcinoma (n = 6), lymphoma (n = 1), mesothelioma (n = 1), mesothelial cell hyperplasia (n = 2), reactive mesothelial changes (n = 1), fibrinous pleuritis (n = 24), empyema (n = 5), Wegener’s granulomatosis (n = 1), and undiagnosed (n = 7) (Table 1).
Diagnosis and causes of pleural effusion in 117 patients.

Data are presented as number (percentage).
TB, Tuberculosis.
The characteristic patterns of pleuroscopy images
Sago-like nodules or micronodules (the ‘A pattern’) in the pleuroscopy images were noted in 20 patients (71.4%) with TB pleurisy and in six patients (6.7%) with non-TB pleurisy (p < 0.001) (Table 2). Adhesion (the ‘B pattern’) in the pleuroscopy image was observed in 20 patients (71.4%) with TB pleurisy and in 37 patients (41.6%) with non-TB pleurisy (p = 0.006). Discrete distribution (the ‘C pattern’) was observed in the pleuroscopy images of 19 patients (67.9%) with TB pleurisy and in none of the patients (0%) with non-TB pleurisy. The presence of sago-like nodules or micronodules was found in the non-TB group with a diagnosis of adenocarcinoma (n = 1), methothelioma (n = 0), and fibrous pleuritis (n = 3). The adhesion was noted in the non-TB group with a diagnosis of adenocarcinoma (n = 15), methothelioma (n = 0), and fibrous pleuritis (n = 13). The presence of A + B features were observed in 13 patients (46.4%), A + C features were observed in 16 patients (57.1%), and B + C features were observed in 11 patients (39.3%) with TB pleurisy. Among patients with non-TB pleurisy, no patient presented with two concomitant features. The presence of any two characteristic features (A + B, A + C, or B + C) was noted in 22 patients (78.6%) with TB pleurisy and in none of the patients with non-TB pleurisy. The presence of all three pleuroscopic features was noted in nine patients (32.1%) with TB pleurisy. The presence of all three features was observed in none of the patients with non-TB pleurisy. In contrast, the absence of all three pleuroscopic features was observed in none of the patients with TB pleurisy, but it was observed in 46 patients (51.7%) with non-TB pleurisy.
Prediction of tuberculosis pleurisy based on pleuroscopy image features.
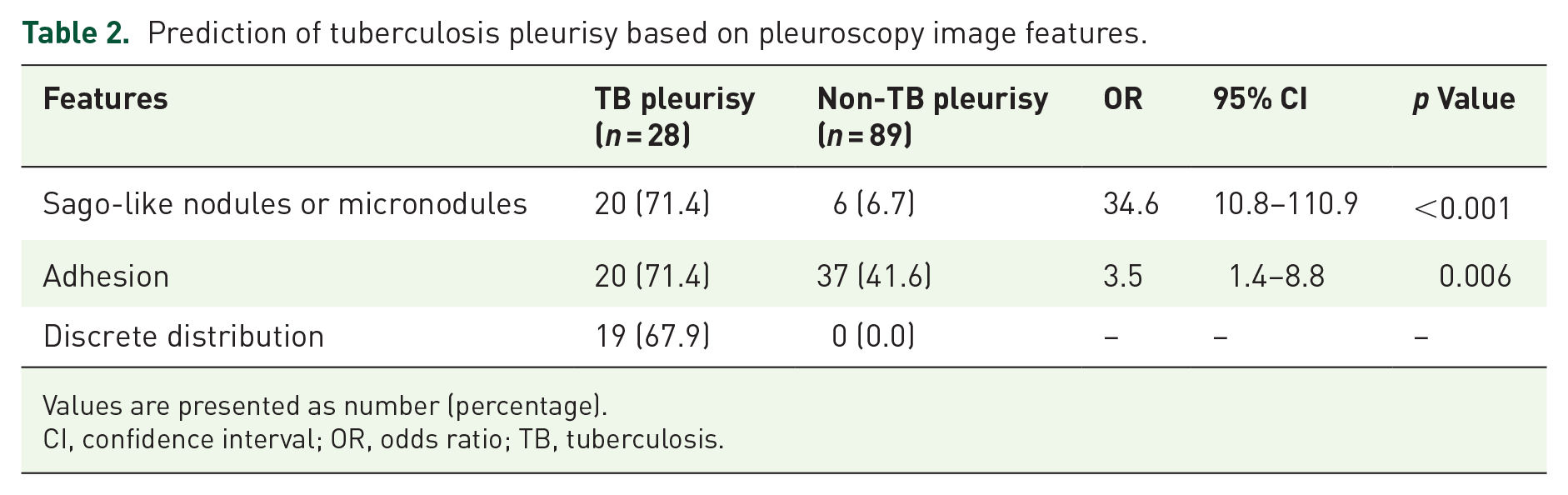
Values are presented as number (percentage).
CI, confidence interval; OR, odds ratio; TB, tuberculosis.
Predictive values of pleuroscopic features for TB pleurisy
The predictive values were initially measured based on each feature alone. Adhesion had the highest sensitivity for the diagnosis of TB pleurisy (71.4%). However, it had the lowest specificity (58.4%). In contrast, discrete distribution had the highest specificity (100.0%) and the lowest sensitivity (67.9%). The sensitivity (71.4%) of sago-like nodules/micronodules was the same as the sensitivity of adhesion. The specificity of sago-like nodules/micronodules (93.3%) was intermediate. The positive predictive value of all three pleuroscopic features for TB pleurisy was 100.0%. The negative predictive value of a lesion with none of the three pleuroscopic features for the diagnosis of TB pleurisy was 100.0%. The positive and the negative predictive values of any two out of three pleuroscopic features for TB pleurisy were 100.0% and 93.7%, respectively (Table 3).
Predictive values pleuroscopic features for tuberculosis pleurisy.

A, Sago-like nodules or micronodules; B, adhesion; C, discrete distribution.
Discussion
The present study showed that with three simplified image features, namely sago-like nodules or micronodules, adhesion, and discrete distribution, pleuroscopy might be a useful tool for differentiating TB pleurisy from non-TB lesions. The presence of any single feature yields a positive predictive value of 39.4% for malignancy. The likelihood of TB pleurisy rises to 100% when the lesion exhibits any two of the specific features. A lesion with all three features is almost certain to indicate TB pleurisy. In contrast, the absence of any of these features is extremely likely to exclude the diagnosis of TB pleurisy.
Conventional diagnostic tests for TB pleurisy include microscopic examination of the pleural fluid for AFB; mycobacterial culture of the pleural fluid, sputum, or pleural tissue; and pathological examination of the pleural tissue for granulomatous inflammation. 8 Mycobacterial culture is a time-consuming process. Hence, sputum AFB smear, pleural effusion AFB smear, and pleural biopsy can provide clinical evidence for the early diagnosis of TB pleurisy. Due to the low prevalence of pleural effusion AFB smear positivity, pleural biopsy is the major contributor to the rapid diagnosis of TB pleurisy. Rapid diagnosis and treatment have long been considered a crucial factor for better outcome in TB patients. 7 Pleural biopsy via pleuroscopy has been widely used due to the higher diagnostic yield when compared with conventional closed tube biopsy. In addition, pleuroscopy could provide larger sized specimens for pathological examination and tissue culture for M. tuberculosis. Cultures of pleural biopsies were positive in 63% of cases, while the positive culture rate of pleural fluid was 5–15%. 15 Drug resistance is a common problem in developing countries. 19 With drug sensitivity results from the culture, aggressive treatment may be administered to improve the outcome while avoiding drug resistance. If any two out of the three characteristic features could be observed in pleuroscopy, the operator should obtain specimens from multiple sites for tissue culture as well as for pathological examination.
Rupture of the sub-pleural caseous focus in the lungs into the pleural space is considered the initial event in the pathogenesis of primary TB pleural effusion. The release of mycobacterial antigens into the pleural space is followed by a delayed hypersensitivity reaction. 20 After cell injury, granulomatous inflammation, which is a histological pattern of tissue reaction, may result from M. tuberculosis infection. It usually consists of necrotizing granulomas. These granulomatous lesions may grossly present as sago-like lesions in the pleura. A recent study demonstrated that a sago-like nodule is the most common gross pleuroscopic finding in TB pleural effusion. 21 Our results were consistent with this finding and showed that a sago-like nodule was observed in more than 70% of the patients with TB pleurisy.
Fibrous tissue formation and adhesions between two different tissues are important reactions during the healing process, especially after inflammation. Adhesion of the pleural cavity may be due to chronic inflammation caused by TB pleurisy. Fibrin is abundant in exudative pleural effusion and may form concentrated deposits. Fibrin might give rise to pleural adhesions, fibrotic septa, and even chronic loculation. In addition, some of the patients with TB pleurisy who have undergone thoracentesis for drainage have more potential for coagulation and adhesion formation. Over two-thirds of the cases with TB pleurisy showed adhesions on thoracoscopy in previous reports.16,22 We also observed that the most common appearance of a pleural lesion in TB pleurisy was adhesion with fibrotic septa on pleuroscopic examination.
In contrast to the discrete distribution pattern of a benign disease, malignant pleural lesions were likely to appear as fused and bulging nodules of various sizes on pleuroscopic examination. 23 The rapid growth of cancer cells and central necrosis pattern may result in the appearance of these lesions. Considering the pathophysiology of TB pleurisy with rupture of antigens into the pleural cavity causing diffuse hypersensitivity reaction, discrete distribution of lesions is a reasonable presentation for TB pleurisy. Therefore, our study suggested that discrete and non-bulging lesions might be the characteristic features for TB pleurisy. The present study showed that 67.9% of the patients with TB pleurisy presented with discrete distribution of lesions. The study by Kong et al. also reported that 64.5% of the TB pleurisy cases showed diffuse miliary lesions on medical pleuroscopic examination. 16
The principal limitation of the present study is its retrospective nature, which might have resulted in an underestimation of the incidence of TB pleurisy and bias in patient selection. Moreover, the sample size of the study was small. Therefore, the results of the present study should be interpreted with caution. Prospective studies with a larger sample size are warranted to confirm the application of these specific features in pleuroscopic examination of undiagnosed pleural effusion. Finally, the study did not measure ADA in pleural fluid. Given the high sensitivity and specificity of ADA,12,13 it is widely used in the diagnosis of TB pleurisy. Nonetheless, the use of ADA measurement in pleural fluid may be limited in terms of availability in developing countries. Due to the requirement for an invasive procedure for pleuroscopy to look for features in patients suspected of TB versus non-TB pleurisy, the results of the study may only be applied in certain countries and hospitals.
Conclusion
In conclusion, a simple classification of pleuroscopic images may prove to be a useful tool for differentiating TB pleurisy from other pleural lesions. A high positive predictive value for TB pleurisy was demonstrated by the presence of any two out of the three characteristic features. The absence of all three features had an excellent negative predictive value for TB pleurisy. Our diagnostic criteria reconfirm that pleuroscopic images can be used as predictors for TB pleurisy in patients with undiagnosed pleural effusion.
Supplemental Material
sj-pdf-1-tar-10.1177_1753466621989532 – Supplemental material for Diagnosis of tuberculosis pleurisy with three endoscopic features via pleuroscopy
Supplemental material, sj-pdf-1-tar-10.1177_1753466621989532 for Diagnosis of tuberculosis pleurisy with three endoscopic features via pleuroscopy by Chung-Shu Lee, Shih-Hong Li, Chih-Hao Chang, Fu-Tsai Chung, Li-Chung Chiu, Chu-Liang Chou, Chih-Wei Wang and Shu-Min Lin in Therapeutic Advances in Respiratory Disease
Supplemental Material
sj-pdf-2-tar-10.1177_1753466621989532 – Supplemental material for Diagnosis of tuberculosis pleurisy with three endoscopic features via pleuroscopy
Supplemental material, sj-pdf-2-tar-10.1177_1753466621989532 for Diagnosis of tuberculosis pleurisy with three endoscopic features via pleuroscopy by Chung-Shu Lee, Shih-Hong Li, Chih-Hao Chang, Fu-Tsai Chung, Li-Chung Chiu, Chu-Liang Chou, Chih-Wei Wang and Shu-Min Lin in Therapeutic Advances in Respiratory Disease
Supplemental Material
sj-pdf-3-tar-10.1177_1753466621989532 – Supplemental material for Diagnosis of tuberculosis pleurisy with three endoscopic features via pleuroscopy
Supplemental material, sj-pdf-3-tar-10.1177_1753466621989532 for Diagnosis of tuberculosis pleurisy with three endoscopic features via pleuroscopy by Chung-Shu Lee, Shih-Hong Li, Chih-Hao Chang, Fu-Tsai Chung, Li-Chung Chiu, Chu-Liang Chou, Chih-Wei Wang and Shu-Min Lin in Therapeutic Advances in Respiratory Disease
Footnotes
Author contribution(s)
Conflict of interest
The authors declare that there is no conflict of interest.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by Chang Gung Medical Research Projects (CIRPG3H0051 to Shu-Min Lin).
Supplemental material
The reviews of this paper are available via the supplemental material section.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.