
Abstract
Background:
Pyogenic lung abscesses are rare and poorly described infections. This study aimed to describe their prognostic factors.
Methods:
We retrospectively included all patients hospitalized between 1 January 1998 and 1 June 2018, with an International Classification of Diseases, version 10 (IDC-10) diagnosis of pyogenic lung abscess, from the Diamm based medical records (Micro6, Nancy, France). Parasitic, fungal, or mycobacterial lung abscesses were excluded.
Results:
A total of 64 patients were included. Abscesses were associated with immunosuppression in 28 patients, including HIV infection and immunosuppressive therapy for eight and 12 patients, respectively. Bacterial identification was obtained for 36 patients. Nine patients (14%) developed lung abscesses after hematogenous dissemination. They differed from bronchogenic abscesses by their younger age (p = 0.03), the absence of smoking or emphysema (p = 0.05), Staphylococcus aureus (p = 0.001) or Streptococcus spp. (p = 0.05) isolation, and the smaller size of their abscess (p = 0.02). Overall, evolution was marked by radiological sequelae (46.9%), relapse (12.5%), and death (4.8%). Radiological sequelae occurred more frequently during the course of bronchogenic abscesses (p = 0.02), particularly when they spontaneously discharged (p = 0.04). Relapses were more frequent in patients with emphysema (p = 0.04) and when Haemophilus influenzae was isolated (p = 0.04). In multivariate analysis, poor outcomes, including death, sequelae, and relapse occurred more frequently in patients who had bronchogenic abscess (p = 0.02), and in those who received antibiotics during less than 6 weeks (p = 0.05).
Conclusion:
A duration of antibiotic treatment of less than 6 weeks and bronchogenic presentation were globally associated with poor outcome of pyogenic lung abscesses. These data should be considered when proposing guidelines for the care of pyogenic lung abscesses.
The reviews of this paper are available via the supplemental material section.
Introduction
Lung abscesses are defined as necrotic cavitary lesions containing pus in the pulmonary parenchyma, leading, after formation of bronchopulmonary fistula, to an air-fluid level inside the cavity.1–3 They are usually caused by pyogenic bacteria, particularly anaerobic bacteria, Staphylococcus aureus, and aerobic Gram-negative bacteria.4–7 In the pre-antibiotic era, mortality from lung abscesses was approximately 75% without treatment. 8 Lung abscess mortality decreased to 20–35% with percutaneous drainage 9 and less to 10% with antibiotic therapy.9–12 Antibiotic treatment, with or without drainage, is currently the standard of care, but up to now no specific guidelines define the duration of antibiotic treatment. Some studies have shown that it may require 3–20 weeks to cure a lung abscess by antibiotic treatment.13,14 Globally, the mortality rate of lung abscesses varies from 1% to 20% depending on study periods and patients’ history,4,6,9–13,15–17 and thus deserves to be better defined. Finally, there is a lack of data regarding other outcome factors, such as radiographic sequelae or relapse in adult lung abscesses.
Our objective was to assess clinical and radiological presentation, bacterial identification and prognostic factors, over the 20-year period of the study, to suggest improvements in the care of patients with lung abscesses.
Methods
Study population
We retrospectively included all patients over 18 years of age hospitalized between 1 January 1998 and 1 June 2018 in the infectious disease unit of Tenon University Hospital (Paris, France) with a diagnosis of pyogenic lung abscess. Consecutive cases of lung abscess were identified by a retrospective search of medical discharge summaries for the 20-year period with the appropriate International Classification of Diseases, version 10 (ICD-10) code.
Data collection
A retrospective review of medical records of all identified cases was performed. All cases of lung pyogenic abscess with clinical and radiological evidence were included; parasitic, fungal, and mycobacterial lung abscesses were all excluded from the study. Lung abscess was defined as a necrotic lung cavitary lesion of more than 2 cm in diameter. Data were collected using a standardized form. General data collected were: patient age, gender, country of birth, HIV infection, other immunosuppressive conditions, tobacco use, alcoholism, diabetes mellitus, dental decay, aspiration risk, oro-tracheal intubation, tracheostomy, sinusitis, lung cancer, emphysema, bronchiectasis, broncho-oesophageal fistula, pulmonary embolism, and pulmonary contusion. The time between the first symptoms and the diagnosis of lung abscess was also recorded. Lung abscesses were considered as acute when the time between the first symptoms and diagnosis was less than 6 weeks and chronic when it was equal to or more than 6 weeks, as in another study. 14 Abscesses secondary to bacteremia occurring from another entry site defined hematogenous lung abscesses. Other abscesses were considered to be bronchogenic. Radiological investigations defined the number of abscesses, pulmonary lobe location, pleural disease, and the largest abscess diameter. Bacterial identification data were also recorded. Therapeutic data collected included the antibiotic molecules administered, treatment duration, percutaneous drainage, surgical management, and spontaneous discharge. Outcome data collected comprised mortality, relapse, and radiological sequelae. Relapse was defined as a new lung abscess occurring in the same location as the previous disease after the end of antibiotic treatment. Radiological sequelae were defined as cavitary lesions, bronchiectasis, or infiltrates persistent in the location of the lung abscess 2 months after treatment ended.
Statistics
The patients’ characteristics were explored using classic descriptive parameters. Univariate analysis comparing the two patient groups (bronchogenic versus hematogenous abscess) was performed using the chi 2 test for qualitative variables (or the Fisher’s test when conditions for the chi 2 test were not met). Quantitative variables were compared using the Student’s t-test (or the Mann–Whitney test when the Student’s test conditions were not met). These analyses were performed using Stata 14 software. Differences were considered statistically significant when the p-value was ⩽0.05.
For the outcome analysis, we considered the composite ‘poor outcome’ criterion defined as death, relapse and/or radiological sequelae. Univariate and multivariate analyses to identify factors associated with the outcome were performed using a logistic regression model. Variable selection for the multivariate logistic regression model was based on significance from univariate analysis as pre-screening (p < 0.25). The odds ratio (OR) along with 95% confidence interval (95% CI) were calculated. p-Values associated with the models’ variables were reported with the threshold of statistical significance set at 5%. These analyses were performed using R software. 18
Ethics
Data were recorded in a clinical database (DIAMM-G; Micro-6, Nancy, France). The National Commission on Informatics and Liberties (CNIL) approved the database used in this study. The study protocol conformed to the ethical guidelines of the 1975 Declaration of Helsinki (revised in Edinburgh in 2000), as reflected by a priori approval by the institution’s human research committee.
Results
General description of the patients
We retrospectively included a total of 64 patients hospitalized between 1 January 1998 and 1 June 2018 with at least one pyogenic lung abscess. The general characteristics are summarized in Table 1. The patients were predominantly men (n = 47; 73.4%). The median age at lung abscess diagnosis was 48 years (interquartile range (IQR) 43–58). Overall, 34 patients (53.1%) were born in France.
General characteristics, radiological presentation, and microbiological identification of patients with pyogenic lung abscesses.

LLL, left lower lobe; LUL, left upper lobe; ML, middle lobe; RLL, right lower lobe; RUL, right upper lobe; USSR, Union of Soviet Socialist Republics.
Lung abscess underlying conditions
The underlying conditions are detailed in Table 1. Immunosuppression was observed in 28 patients (43.7%), and included HIV infection (n = 8, 12.5%), diabetes mellitus (n = 7, 10.9%), and others (18.7%). Underlying conditions were smoking for 47 patients (73.4%), alcoholism for 25 (39.0%), and dental decay for 22 (34.4%); other conditions were less frequent: emphysema for 14 patients (21.9%), aspiration risks for nine (14.0%), sinusitis for five (7.9%), lung cancer for three (4.7%), and tracheostomy for three (4.7%). Bronchiectasis, pulmonary embolism, and lung contusion were each observed in one patient (1.6%).
Clinical and radiological presentations
The lung abscess symptom onsets were acute in 44 patients (68.7%). Seventeen patients (26.6%) had multiple lung abscesses. Radiographic analyses showed the right lower lobe (RLL) to be the more frequent location (n = 21, 32.8%). Multi-lobe abscesses were more frequently observed in acute presentation [eight (18.2%) versus zero (0%); p = 0.04]. Pleural effusion was more frequent in non-immunosuppressed patients [18 (50.0%) versus six (23.1%); p = 0.05]. The mean of the largest abscess diameter was 55.7 mm (±28.1). The abscess diameters appeared larger when the patient had underlying chronic sinusitis (p = 0.02).
Nine patients (14.1%) developed lung abscesses after hematogenous dissemination, whereas the others developed lung abscesses after bronchogenic dissemination. The main differences between bronchogenic and hematogenous lung abscesses are reported in Table 2. Patients with hematogenous abscesses were younger [45 years (29–50) versus 48 years (44–60); p = 0.03]. Multi-lobe abscesses were more frequently observed in patients with hematogenous abscesses [five (55.5%) versus three (5.4%); p = 0.01]. Smoking and emphysema conditions appeared more frequently in patients with bronchogenic abscesses (p = 0.05). The abscess diameters were larger when they had bronchogenic origin (59.8 mm ±27.5 versus 30.4 ±16.4, p = 0.02).
Main differences between bronchogenic and hematogenous lung abscesses.
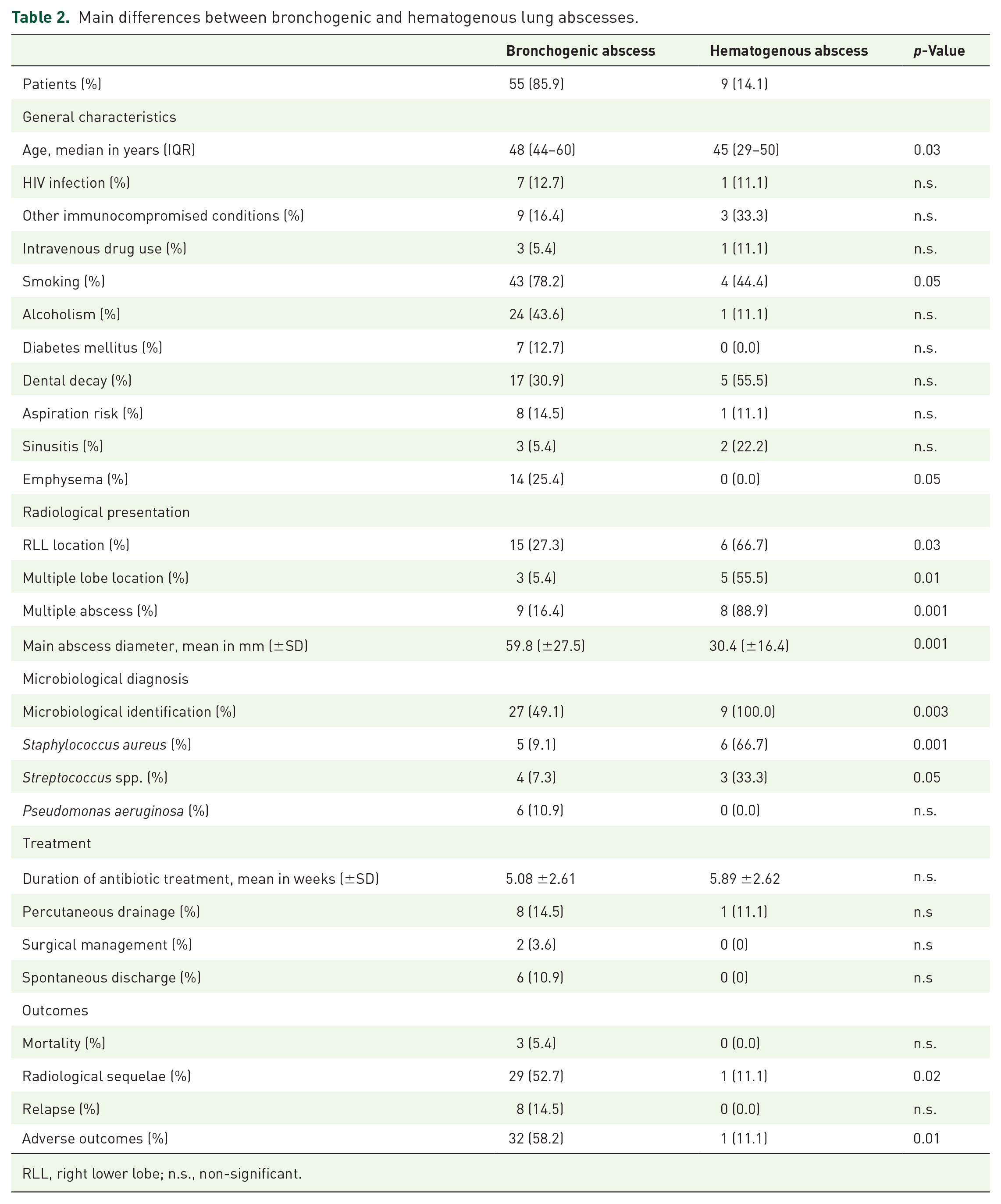
RLL, right lower lobe; n.s., non-significant.
Microbial identification
The microbial agent responsible for the lung abscess was identified for 36 (56.2%) patients. Bacteria were more frequently documented in immunosuppressed patients [11 (92.7%) versus 25 (48.1%); p = 0.006], those with underlying aspiration risks [eight (88.9%) versus 28 (50.9%); p = 0.03], and when percutaneous drainage was performed [eight (88.9%) versus 28 (50.9%); p = 0.03]. The microbial agents isolated in lung abscesses are detailed in Table 1. The four more frequently identified bacteria were Staphylococcus aureus (n = 11), Streptococcus spp. (n = 7), Pseudomonas aeruginosa (n = 6), and Haemophilus influenzae (n = 3). Streptococcus spp. were more frequently documented when pleural effusion complicated the lung abscesses [three (12.5%) versus zero (0.0%); p = 0.05], in women [five (29.4%) versus two (4.2%); p = 0.01], and in hematogenous lung abscesses [three (33.3%) versus four (7.3%); p = 0.05]. S. aureus was more frequently identified when the abscesses were multiple [seven (41.2%) versus four (0.8%); p = 0.005], multi-lobe [four (50.0%) versus seven (12.5); p = 0.02], or of hematogenous origin [six (66.7%) versus five (9.0%); p = 0.0001]. P. aeruginosa was more frequently isolated in patients with tracheostomy [two (66.7%) versus four (6.6%); p = 0.02] and those with aspiration risks [three (33.3%) versus three (5.4%); p = 0.03]. Staphylococcus spp. and Streptococcus spp. were more frequently documented in hematogenous abscesses (p = 0.001 and p = 0.05, respectively), whereas microbial documentation appeared less frequent in bronchogenic abscesses (p = 0.003) (Table 2).
Treatment and outcomes
The treatment and outcomes are detailed in Table 2. All patients received antibiotics. The mean duration of antibiotic treatment was 5.0 (+/− 2.5) weeks. In addition, 11 patients benefited from a drainage procedure. Percutaneous drainage was performed in nine patients and surgical management in two. Percutaneous drainage was more frequently performed when pleural effusion complicated the lung abscess [six (25.0%) versus three (7.5%); p = 0.05] and in documented Streptococcus spp. lung abscesses [three (42.9%) versus six (10.5%); p = 0.05]. Spontaneous discharge of the abscess occurred in four patients. Among the 64 patients treated with antibiotic treatment, 30 (46.9%) received antibiotics for less than 6 weeks and 34 (53.1%) for more than 6 weeks. The proportion of emphysema was higher in the group treated for less than 6 weeks [11 (37%) versus three (9%); p < 0.01]. Bacteria were more frequently identified in the group treated for more than 6 weeks [23 (67%) versus 13 (43%); p = 0.05].
Poor outcomes included mortality (4.8%), relapse (12.5%), and radiological sequelae (46.9%). Relapses were more frequent in patients with emphysema [four (28.6%) versus four (8%); p = 0.04] and in documented H. influenza lung abscesses [two (66.7%) versus six (9.8%); p = 0.04]. Radiographic sequelae occurred more frequently in patients with bronchogenic abscesses [29 (52.7%) versus one (11.1%); p = 0.02] (Table 2), those with spontaneous discharge [four (100%) versus 26 (43.3%); p = 0.04], and when the abscesses were limited to one lobe [29 (96.7%) versus 27 (79.4%); p = 0.04]. Globally, in univariate analysis, poor outcomes were more frequently observed in patients with underlying emphysema (p = 0.03). They were less frequently observed in hematogenous lung abscess (p = 0.03) and when the antibiotic treatment duration was over 6 weeks (p = 0.02). In multivariate analysis, the risk of poor outcomes was lower in patients who received more than 6 weeks of antibiotic treatment [OR = 0.31 (0.09–0.96); p = 0.05], and in patients suffering from hematogenous abscesses [OR = 0.07 (0.00–0.48); p = 0.02], but was not increased in patients with underlying emphysema [OR = 1.64 (0.32–9.77)] (Table 3 and Figure 1).
Multivariate logistic regression model of factors impacting outcomes in 64 patients hospitalized with pyogenic lung abscess.
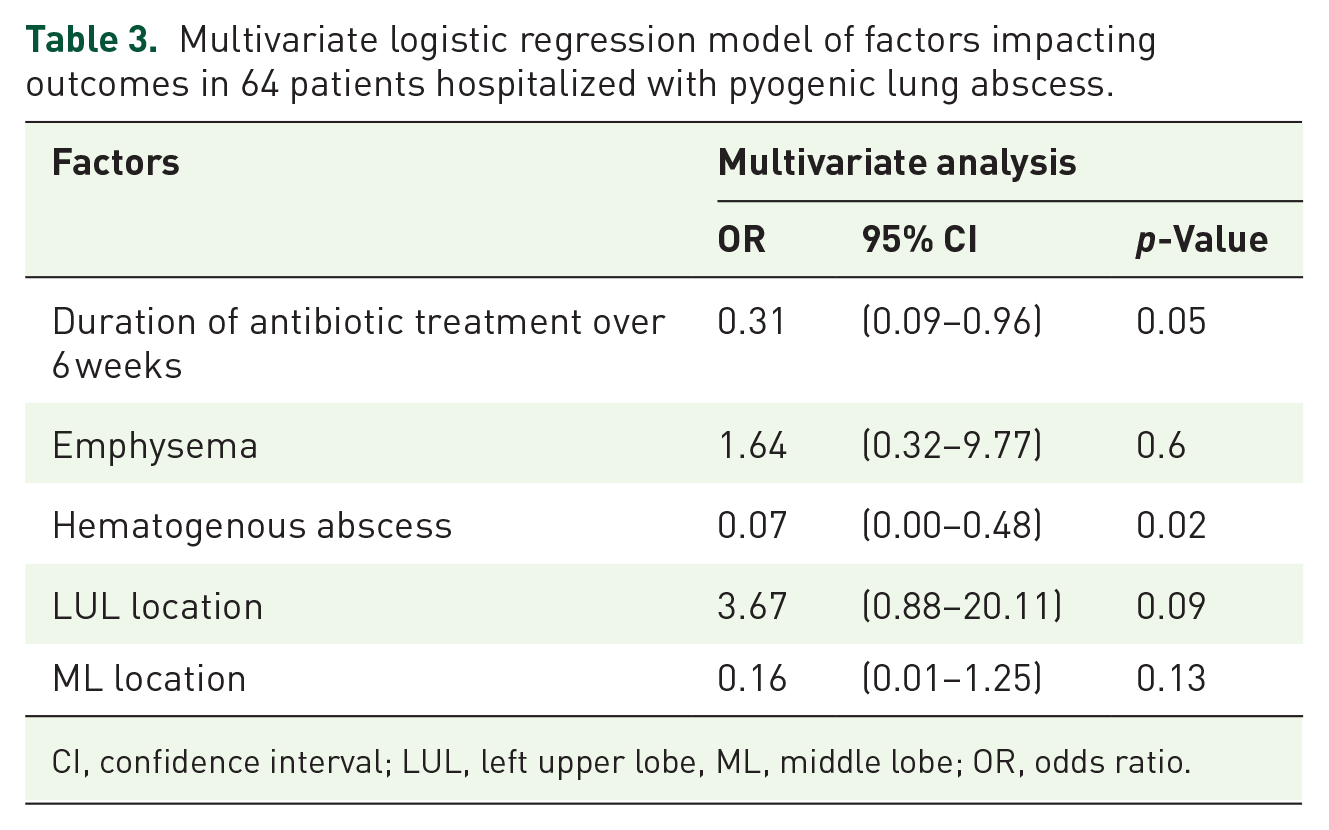
CI, confidence interval; LUL, left upper lobe, ML, middle lobe; OR, odds ratio.

Main factors which impact significantly on pyogenic lung abscess outcomes.
Discussion
There are no specific guidelines for the care of patients with lung abscesses, few and short series of such patients are reported in the literature.6,12,13,17 Patients who develop lung abscesses make up a very heterogonous population. In the present study, we distinguished pragmatically two main groups of patients with a specific presentation, microbial identification, and prognosis. The first one consists of the youngest patients, who developed lung abscesses associated with hematological dissemination, that is, positive blood cultures from another entry site. Their radiological presentations consisted of multiple abscesses in multiple lobe locations of smaller size than bronchogenic abscesses. The main bacteria associated with these presentations were Gram-positive cocci, particularly S. aureus and Streptococcus spp. These bacteria had recently showed a particular affinity to invade the pleural space and induce pleural effusion complicating lung abscess by pleural infection. 19 Thus, we recommend that empiric antibiotic treatment should consist of bactericidal molecules against Streptococcus and Staphylococcus spp. as soon as hematogenous presentation is suspected. Empiric treatment should cover methicillin-resistant Staphylococcus aureus (MRSA) when severe pulmonary infection requires admission in the intensive care unit, and should consider the potential risk of MRSA in specific situations such as nosocomial context or intravenous drug use. We suggest empiric treatment with amoxicillin and clavulanic acid,20,21 and vancomycin if MRSA had to be covered. 22 The second group is composed of the oldest patients and corresponds to those developing lung abscesses with a bronchogenic presentation. Their abscesses were more frequently unique, limited to one lobe, and larger than those observed in the hematogenous presentation. Patients who developed bronchogenic lung abscesses appeared to have a history of smoking and previous emphysematous lung disease. Globally, patients with bronchogenic lung abscesses had a worse prognosis than those with hematogenous lung abscesses in our study. Among patients with a bronchogenic presentation, P. aeruginosa was more frequently isolated in patients with aspiration risks and, more particularly, tracheostomy. Therefore, we recommend including Pseudomonas spp. in the spectrum of empiric antibiotic treatment proposed for patients with aspiration risk and suggest empiric treatment with piperacillin and tazobactam to maintain anti-anaerobic activity. 23
The median age of the patients (48 years) and large proportion of smoking history (73%), as well as the frequency of alcoholism (39%), dental decay (34%), HIV infection (12%), diabetes mellitus (11%), and aspiration risks (14%) of our studied population are similar to those reported in previous work.6,12,13,17 Nevertheless, we observed a smaller proportion of lung cancer (5%), and bronchiectasis (2%) than in the other studies.6,12,13,17 Just under half of the patients were immunosuppressed. Immunocompetent patients developed lung abscesses, which were more frequently complicated by pleural effusion. These data support the previous results of Mansharamani et al., 6 who reported more pleuritic chest pain in immunocompetent patients hospitalized with a lung abscess. In our study, the RLL was the most frequently affected lung segment (in 33% of patients), contrary to what Mansharamani et al. 6 observed. This difference can be explained by the exclusion of mycobacterial infections from our study, which clearly mainly affect apical segments of the lung. 24 Moreover, the large proportion of alcoholism (40%) and other aspiration risks (14%) in our study, led to the aspiration of oral secretion when unconscious, and concerned particularly the RLL because anatomically the right bronchus is straighter than the left.
Our microbiological data show that S. aureus and P. aeruginosa were the two main bacteria isolated in lung abscesses, as in the study by Mansharamani et al. 6 Streptococcus spp. appeared as the principal bacteria identified in community-acquired lung abscesses 13 and was the third most frequent in our study, which combines nosocomial and community-acquired lung abscesses. Early reports identified multiple species of anaerobic bacteria in lung abscesses on regular basis,7,25–28 whereas recent studies such as ours found anaerobes in a substantially lower proportion in favour of aerobes.14,29–31 The increasing wide-spectrum empiric antibiotic treatment before bacteriological study in daily practice, impacting particularly anaerobic bacteria, could explain this difference. 32
The mortality rate of lung abscess patients can vary widely, from 1% to 20%, depending on the study.4,6,9–13,15–17 We have shown that larger abscesses correlate with a poorer prognosis as described in previous studies.15,17 In our study, outcomes were assessed not only by mortality, but also relapse and radiological sequelae rates. The relapse rate was higher in patients with emphysema, which may be induced by the shorter antibiotic treatment duration we observed in these patients as worse outcome was not confirmed in our multivariate analysis. We observed radiological sequelae in 47% of patients. This high rate is close to that (49%) recently published in children. 33 Radiological sequelae were more frequently observed in patients with bronchogenic abscesses and when spontaneous discharge occurred. This finding may also be explained by the persistence of aspiration risk factors (e.g. tracheostomy) in these patients. In addition to antibiotic treatment, percutaneous drainage and/or surgery may be necessary to cure certain patients. The use of these techniques varies widely depending on the study, as percutaneous drainage and surgery were performed in 1–94% and 2–41% of patients, respectively.6,12,13 In our study, percutaneous drainage was performed in 14% of patients and surgery in 3%, without a significant impact on outcomes. Percutaneous drainage provided bacterial identification and was preferentially performed when pleural effusion complicated the lung abscess. There is no consensus on the duration of antibiotic treatment and it depends on the clinical and radiological response of the patient. Treatment should obviously be administered until at least fever, putrid sputum, and abscess fluid have resolved. According to expert opinions, the rate of therapeutic failure including relapse, is low if antibiotic therapy is pursued until radiography changes to a normal range. 34 This may require a total duration of 28–48 days, as suggested in a previous study. 13 Expert opinions recommend a prolonged antibiotic therapy over 6 weeks to prevent therapeutic failure; 35 our study is the only to confirm poor outcomes in patients treated for less than 6 weeks.
The limitations of this study included its retrospective nature, its being a single-center study, and the small number of patients. Moreover, the 20-year period of the study may have complicated the interpretation of the results, given the considerable improvements in both diagnosis and treatment of lung abscesses from 1998 to 2018. Moreover, the poorer prognosis observed in patients with bronchogenic abscess may be due to their general and pulmonary comorbidities and only a fraction of them was considered in our multivariate analysis.
This study indicates that the clinical and radiological presentations of lung abscesses are the main parameters which determine bacterial identification, and outcomes. We suggest that this presentation should guide empirical antibiotic treatment. The prognosis of patients was globally unfavourable when the presentations were bronchogenic and the treatment duration less than 6 weeks. These data should be considered when proposing guidelines for the care of patients with lung abscesses.
Supplemental Material
sj-pdf-1-tar-10.1177_17534666211003012 – Supplemental material for Pyogenic lung abscess in an infectious disease unit: a 20-year retrospective study
Supplemental material, sj-pdf-1-tar-10.1177_17534666211003012 for Pyogenic lung abscess in an infectious disease unit: a 20-year retrospective study by Thomas Maitre, Vichita Ok, Ruxandra Calin, Ludovic Lassel, Ana Canestri, Michel Denis, Mohammed Hamidi, Sebastian Tavolaro, Charlotte Verdet, Antoine Parrot, Jacques Cadranel and Gilles Pialoux in Therapeutic Advances in Respiratory Disease
Supplemental Material
sj-pdf-2-tar-10.1177_17534666211003012 – Supplemental material for Pyogenic lung abscess in an infectious disease unit: a 20-year retrospective study
Supplemental material, sj-pdf-2-tar-10.1177_17534666211003012 for Pyogenic lung abscess in an infectious disease unit: a 20-year retrospective study by Thomas Maitre, Vichita Ok, Ruxandra Calin, Ludovic Lassel, Ana Canestri, Michel Denis, Mohammed Hamidi, Sebastian Tavolaro, Charlotte Verdet, Antoine Parrot, Jacques Cadranel and Gilles Pialoux in Therapeutic Advances in Respiratory Disease
Supplemental Material
sj-pdf-3-tar-10.1177_17534666211003012 – Supplemental material for Pyogenic lung abscess in an infectious disease unit: a 20-year retrospective study
Supplemental material, sj-pdf-3-tar-10.1177_17534666211003012 for Pyogenic lung abscess in an infectious disease unit: a 20-year retrospective study by Thomas Maitre, Vichita Ok, Ruxandra Calin, Ludovic Lassel, Ana Canestri, Michel Denis, Mohammed Hamidi, Sebastian Tavolaro, Charlotte Verdet, Antoine Parrot, Jacques Cadranel and Gilles Pialoux in Therapeutic Advances in Respiratory Disease
Footnotes
Author contributions
Study conceptualization and design: TM, LL and GP; data collection: TM and MH; statistical analysis: VO, MH and TM; interpretation of results: TM, JC and GP; manuscript preparation: TM, GP, JC and VO; approval for final version of the manuscript: all authors.
Conflict of interest statement
The authors declare that there is no conflict of interest.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.