
Abstract
Background:
A meta-analysis was performed for a comparison of outcomes between video-assisted thoracoscopic surgery (VATS) and thoracotomy for congenital lung malformations (CLM).
Methods:
Electronic databases, including PubMed, Scopus, Embase, and the Cochrane Library were searched systematically for literature aimed mainly at reporting the therapeutic effects for CLM administrated by VATS and thoracotomy.
Results:
A total of 40 studies meeting the inclusion criteria were included, involving 2896 subjects. VATS was associated with fewer complications [odds ratio (OR) 0.54; 95% confidence interval (CI), 0.42–0.69], less use of epidural anesthesia (OR, 0.08; 95% CI, 0.03–0.23), shorter length of hospital stay [standard mean difference (SMD) −0.98; 95% CI, −1.4 to −0.55] and chest drainage (SMD, −0.43; 95% CI, −0.7 to −0.17), as compared with thoracotomy. However, thoracotomy showed superiority in reduced operative time (SMD, 0.44; 95% CI, 0.04–0.84). Pearson analysis (Pearson r = 0.85, 95% CI, 0.28 to 0.98, p = 0.01) and linear regression (R square 0.73) confirmed a positive correlation between percentage of symptomatic cases and conversion in patients using VATS.
Conclusion:
VATS is associated with fewer complications, less use of epidural anesthesia, shorter length of stay and length of chest drainage, but longer operative time, as compared with thoracotomy. Symptomatic patients with CLM using VATS may be prone to conversion to thoracotomy.
The reviews of this paper are available via the supplemental material section.
Introduction
Congenital lung malformations (CLM) is a rare congenital disorder that accounts for 5–18% of all congenital diseases. 1 There is a wide spectrum of congenital pulmonary abnormalities, 2 including congenital pulmonary airway malformations (CPAM, formerly known as congenital cystic adenomatoid malformations), pulmonary sequestration (PS), congenital lobar emphysema (CLE), and bronchogenic cyst (BC). In recent years, prenatal ultrasonography and magnetic resonance imaging (MRI) have contributed significantly to the early diagnosis of CLM.
The presentations of CLM vary widely, from respiratory distress to entirely asymptomatic lesions. It is unquestionable that symptomatic CLM cases can benefit from surgical resection. A meta-analysis also further indicated the advantages of elective surgery in the management of asymptomatic conditions, preventing the risks of chest infection and malignancy later in life. 3 Thoracotomy is a traditional and well-known surgical approach for CLM. However, long-term complications, such as breast deformity, rib fusion, winged scapula, and scoliosis have been reported to occur in up to 30% of children with the use of thoracotomy. 4 Video-assisted thoracoscopic surgery (VATS) – a minimally invasive procedure – has been introduced for the management of CLM in experienced pediatric surgery centers in the last two decades. 5 However, the use of VATS also raises concerns regarding prolonged general anesthesia, hypercapnia, and difficulty with single-lung ventilation.
Two published meta-analyses compared VATS versus open surgery for patients with CLM6,7; however, there were some significant drawbacks in each study. The Nasr and Bass study involved a study adopting cervical incision or laparotomy for CLM, which was against their inclusive criteria. 6 The risk of bias in their included studies was not evaluated. Although this was the first meta-analysis in this field, their results were less conclusive since heterogeneity across studies was not evaluated. Adams et al. published a meta-analysis involving both single- and two-arm studies. 7 Unfortunately, they did not take into account publication bias in their meta-analysis; therefore, selection bias due to incomplete retrieval of literature might exist. Though their aim was to evaluate only asymptomatic patients, several included studies were found to have symptomatic cases. Therefore, our study aims to perform an updated meta-analysis comparing the outcomes of VATS and thoracotomy for patients with CLM, and to address the limitations of the two previous meta-analyses.
Methods
Literature search
Our methods were in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. 8 The protocol of this study was registered on PROSPERO (CRD42020171061, https://www.crd.york.ac.uk/prospero). A systematic search of the PubMed, EMbase, Scopus, and Cochrane Library CENTRAL for the relevant published studies comparing the outcomes of VATS versus thoracotomy for CLM cases was conducted in February 2020. VATS was not used commonly for CLM until the late 1990s; therefore, to avoid potential selection bias, year of publication was restricted from January 2000 to February 2020. The strategy used for searching was (congenital cystic adenomatous malformation OR congenital pulmonary airways malformation OR bronchogenic cyst OR pulmonary sequestration OR congenital lobar emphysema OR congenital lung lesions OR congenital lung diseases) AND [(thoracoscopy OR thoracoscopic surgery OR video-assisted thoracic surgery OR minimally invasive surgery) OR (open surgery OR conventional surgery OR thoracotomy)]. References from all included studies and other relevant literature were also reviewed manually to identify additional eligible studies. This search was restricted to articles that were published in English. We contacted the authors to obtain extra information via e-mail as necessary.
Study selection
A study was included in this systematic review when the following criteria were met: (1) single-arm case series, observational studies (cohort or case-controlled studies) or randomized controlled trials (RCTs) that presented outcomes of VATS and thoracotomy for CLM; (2) the procedure of each surgical approach was described. Briefly, thoracotomy should be performed through a conventional posterolateral thoracotomy. VATS was performed through several port incisions and under the observation of thoracoscopy.
A study was excluded in this systematic review when the following criteria were met: (1) multiple studies were based on the same data; (2) sample size of single-arm studies was less than 10 cases; (3) studies involved patients over 16 years of age. Reviews, letters, conference abstract, case reports, and animal experiments were also excluded. When several studies were based on the same sample (same database and time period), only the study with most complete set of data was included.
Data extraction and definition of variables
Data was extracted by both reviewers (X.J.H. and W.Y.H.) independently, any disagreement was resolved by consensus with the help of a third reviewer (W.C.). A standardized extraction form in an Excel spreadsheet was used. The following information was extracted: (1) baseline characteristics of included studies: first author, publication year, study area, types of study design, types of CLM, surgical approach, sample size, operative age, recommended age for elective surgery, percentage of symptomatic cases, conversion, and follow-up time; (2) outcomes of VATS and thoracotomy approaches: causes of conversion, operative time, length of hospital stay (LOS) and chest drainage time, use of epidural anesthesia, and complications after surgery.
Symptomatic patients with CLM were defined as patients who presented with respiratory symptoms or chest infection before surgery. Complications after surgery referred to wound infection, pneumonia, pleural effusion, air leaks, etc. Operative time was defined as time duration of each operation. LOS was defined as the time period from admission to discharge. Chest drainage time was defined as the time period from insertion to removal of the chest tube. Conversion was considered when thoracoscopic surgery was converted to thoracotomy due to unsatisfied exposure, bleeding, adhesion, or other reasons.
Quality assessment and risk of bias
Quality assessment and risk of bias were performed by two reviewers (W.Y.H. and X.J.H.) independently, and any disagreements on the assessed quality were resolved with a third reviewer (W.C.) by consensus. The risk of bias of non-RCTs (NRCTs) was evaluated with the ROBINS-I tool. 9 The risk of bias of single-arm case series was evaluated using the methodological index for non-randomized studies (MINORS) guidelines.
Statistical analysis
All statistical analyses were conducted using RevMan software (version 5.3; The Nordic Cochrane Centre, Copenhagen, Denmark). Odds ratio (OR) and standard mean difference (SMD) were employed for dichotomous and continuous data, respectively. The χ2-Q statistics and I2 statistics were used to assess heterogeneity, with I2 > 50% indicating heterogeneity. If the I2 statistic was >50%, a random-effect model was adopted. Subgroup analysis and sensitivity analysis were used to explore the sources of heterogeneity; otherwise, a fixed-effect model of analysis was used. Sensitivity analysis was performed using the leave-one-out method. Subgroup analysis was conducted in terms of types of CLM, operative age, conversion to thoracotomy and percentage of symptomatic cases. If only the median value and range were available in our included studies, the formulas provided by Hozo et al. were used to estimate the mean value and standard difference. 10 Publication bias was evaluated with funnel plot, Begg’s and Egger’s tests (Stata 12.0, Stata Corp, College Station, TX, USA). Pearson analysis and linear regression were performed using Graphpad (V7.0, GraphPad Software Inc., La Jolla, CA, USA). A p value <0.05 was considered statistically significant for all analyses in our study.
Results
Characteristics of included studies
A total of 3747 studies were obtained initially from the electronic databases and seven papers were further identified manually on reference lists of the retained studies. After screening for duplicates and relevance in titles and abstracts, only 109 studies were available for the full-text evaluation for eligibility; 69 studies were excluded after full-text evaluation. Eventually, this review was based on 40 NRCTs,11–50 which encompassed 23 two-arm case-controlled studies,11–33 and 17 single-arm case series.34–50 A flowchart depicting the search strategy is shown in Figure 1.

Flowchart of process for literature screening for this meta-analysis according to PRISMA guidelines.
All 40 studies were retrospective NRCTs (Table 1) published between 2004 and 2020. A total of 2896 patients were involved, of which 1372 patients were in the VATS group and 1524 patients in the thoracotomy group. Over half of our included studies reported ‘hybrid’ types of CLM, and 15 studies focused on each specific type. CPAM was the main reported type of CLM. Lobectomy was the approach used most frequently for lung resection (Supplemental Table S1). Only five studies were based completely on asymptomatic cases. Rate of conversion ranged from 0% to 40.9%. The leading causes of conversion were hemorrhage, poor visualization, and intolerance to single-lung ventilation. The most frequently recommended timing for elective surgery in the management of CLM was 6–12 months of age. A total of four studies reported post-operative death in 11 patients.
Baseline characteristics of included studies.
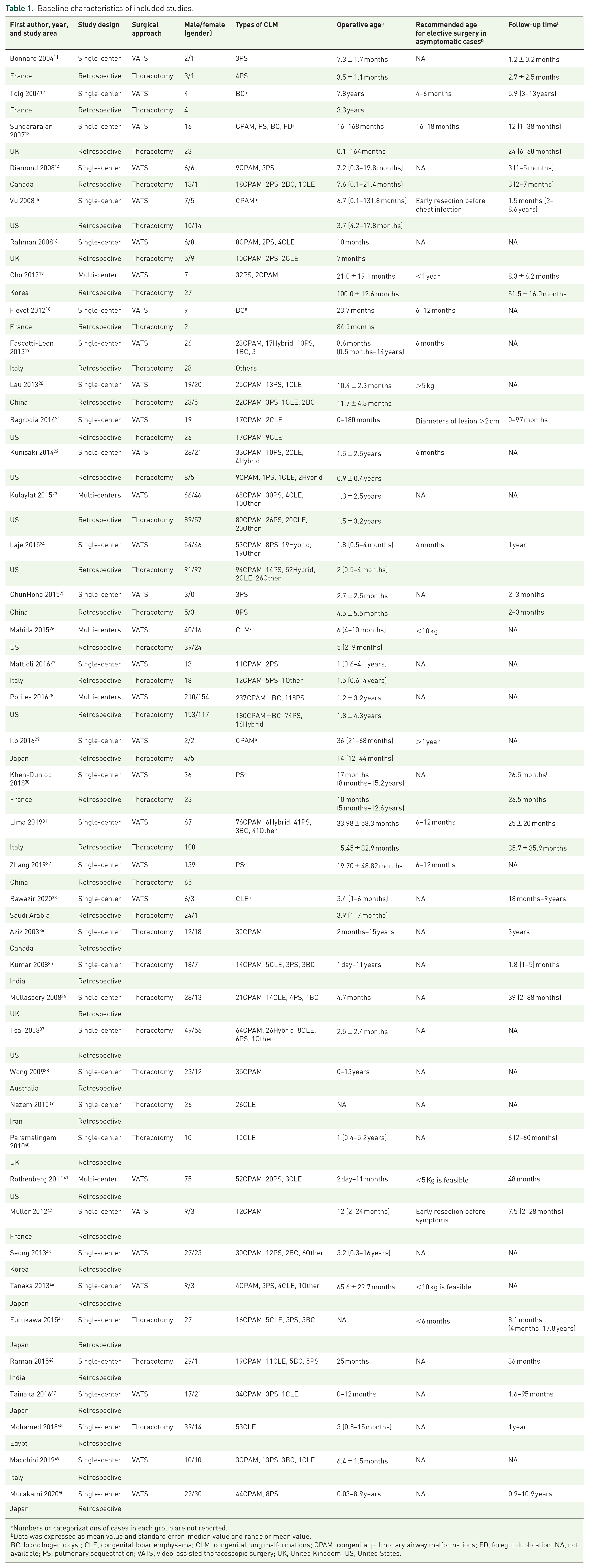
Numbers or categorizations of cases in each group are not reported.
bData was expressed as mean value and standard error, median value and range or mean value.
BC, bronchogenic cyst; CLE, congenital lobar emphysema; CLM, congenital lung malformations; CPAM, congenital pulmonary airway malformations; FD, foregut duplication; NA, not available; PS, pulmonary sequestration; VATS, video-assisted thoracoscopic surgery; UK, United Kingdom; US, United States.
Complications
A total of 22 studies compared the complications after surgery of both procedures.11–31,33 Air leaks and chest infection were the most common complications after surgery. Pectus excavutum and scoliosis, which were the long-term complications with the use of thoracotomy, were reported in only one study. 15 This meta-analysis result indicated that VATS was associated with fewer complications after surgery, as compared with thoracotomy [OR, 0.52; 95% confidence interval (CI), 0.40 to 0.67; P < 0.00001; I2 = 29%, Figure 2A]. Infectious complications, which included wound infections and respiratory infections, and bleeding were more common using thoracotomy, as shown in Supplemental Table S2.

Forest plots of complications and use of epidural anesthesia. Forest plot of OR of (A) post-operative complications and (B) use of epidural anesthesia.
A total of 10 and 7 single-arm studies reported complications from thoracotomy and VATS, respectively. Among 10 single-arm studies that reported complications of thoracotomy, the pooled estimate of complications of thoracotomy was 22% (95% CI 12–32%, I2 = 87.3%). Among seven single-arm studies that reported complications from VATS, the pooled estimate of complications was 7.1% (95% CI 0.8% to 13.3%, I2 = 53.3%) using VATS.
Use of epidural anesthesia
Four studies compared the use of epidural anesthesia after surgery.11,13,14,16 This meta-analysis indicated that VATS was associated with less use of epidural anesthesia after surgery than with thoracotomy (OR, 0.08; 95% CI, 0.03–0.23; p < 0.00001; I2 = 0%, Figure 2B).
Operative time
A total of 17 studies compared the operative time of both surgical approaches.11,12,15,17,19,20,22–27,29–33 However, in one study, Laje et al. incorrectly reported the operative time data. 24 Therefore, this meta-analysis included the remaining 16 studies. This meta-analysis indicated that VATS was associated with longer operative times than with thoracotomy (SMD, 0.44; 95% CI, 0.04–0.84; p = 0.03; I2 = 88%, Figure 3A). Due to significant heterogeneity, sensitivity analysis with the use of the leave-one-out method was adopted. I2 reduced to 72% when we removed the studies of Zhang et al. and Lima et al. in turn.31,32 This did not appreciably change the direction and magnitude of the pooled estimates (SMD, 0.65; 95% CI, 0.32–0.98; p = 0.0001).

Forest plot of operative time (min) and LOS (days). (A) Forest plot of SMD of operative time; (B) forest plot of SMD of LOS.
Length of hospital stay
A total of 17 studies compared the LOS.11,12,14,17,19,21–24,26,27,29,31–33 This meta-analysis indicated that VATS was associated with shorter LOS when compared with thoracotomy (SMD, −0.98; 95% CI, −1.4 to −0.55; p < 0.00001; I2 = 91%, Figure 3B). Sensitivity analysis was performed due to significant heterogeneity. I2 was reduced to 72% when we removed Mahida et al., Lau et al. and Mattioli et al. studies in turn.20,26,27 The direction and magnitude of the pooled estimates did not change (SMD, −0.48; 95% CI, −0.74 to −0.21; p = 0.0004).
Length of chest drainage
A total of 13 studies compared the length of chest drainage (Figure 4A).11,12,14,17,19,21–24,26,27,29,31–33 This meta-analysis indicated that VATS was associated with shorter length of chest drainage than with thoracotomy (SMD, −0.43; 95% CI, −0.7 to −0.17; p = 0.001; I2 = 65%). Sensitivity analysis was also performed to explore the origin of heterogeneity. I2 reduced to 44% when we removed Laje et al. and Kunisaki et al. studies in turn.22,24 The direction and magnitude of the pooled estimates did not change (SMD, −0.58; 95% CI, −0.83 to −0.33; P < 0.00001).

Forest plot of length of chest drainage (days) and publication bias analysis by funnel plot. (A) Forest plot of SMD of length of chest drainage; (B) publication bias analysis by funnel plot.
Subgroup analysis
In the subgroup analysis of operative time, when studies were stratified by the mean operative age, thoracotomy was associated with a shorter operative time in 0–6 months and 6–12 months groups. Similarly, thoracotomy was associated with shorter operative times in groups with no conversion (Supplemental Table S3). In the subgroup analysis of LOS, shorter LOS was observed in PS group using VATS. In the subgroup analysis of complications, when studies were stratified by the types of CLM, fewer complications were observed in CPAM and mixed type groups using VATS. Fewer complications were also observed in the group where patients were over 1 year of age. Similar results were found in studies without conversion and with low percentage of symptomatic cases. In the subgroup analysis of length of chest drainage, VATS was superior in PS and mixed type groups. It also showed superiority in patients over 6 months of age. VATS entailed shorter length of chest drainage in studies without conversion and with low percentage of symptomatic cases.
Risk of bias
To evaluate the publication bias, we conducted the funnel plot of complications (Figure 4B); no significant publication bias was found (Begg’s test p = 0.96, Egger’s test p = 0.17). ROBINS-I toll was used for bias assessment of comparatives studies; 14 studies were found to be at moderate risk of bias (Supplemental Table S4), and 9 studies were deemed to be at serious risk of bias. MINORS scores of nine single-arm studies were higher than 10 points and with high qualities.34–36,40,42,45,46,48,50
Correlation between symptomatic percentage and conversion using VATS
A total of 11 studies were involved for Pearson analysis, which was used to evaluate the correlation between percentage of symptomatic cases and conversion in patients who underwent VATS. It turned out that the Pearson correlation coefficient was 0.92 (95% CI, 0.71–0.98, P < 0.0001) and R square was 0.84 (Figure 5A).

Pearson analysis and linear regression. (A) Correlation between percentage of symptomatic cases and conversion using the VATS; (B) correlation between percentage of symptomatic cases and lobectomy.
Correlation between percentage of symptomatic cases and lobectomy
A total of 15 studies were used to evaluate the correlation between percentage of symptomatic cases and lobectomy. Pearson correlation coefficient was 0.24 (95% CI, −0.32 to 0.67, p = 0.39) and R square was 0.24 (Figure 5B).
Discussion
VATS has emerged as the standard procedure for many conditions in pediatric patients. 51 So far, no definitive consensus that thoracoscopic resection yields better outcomes in the treatment of CLM has been established though two meta-analyses,6,7 which compared VATS with thoracotomy for CLM. Nasr and Bass found no differences between thoracotomy versus VATS for CLM with respect to complications and operative time. 6 Adams et al. further confirmed the superiority of VATS when comparing for complications. 7 Since these two reports, there have been a large number of high-volume case-controlled studies. Therefore, we updated this study to further explore the comparison between use of VATS and thoracotomy. Our meta-analyses indicated that VATS was associated with fewer complications, less use of epidural anesthesia, and shorter LOS and length of chest drainage when compared with thoracotomy. However, thoracotomy showed superiority in reduced operative time. Pearson analysis and linear regression confirmed a positive correlation between percentage of symptomatic cases and conversion in patients using VATS. However, the correlation between percentage of symptomatic cases and lobectomy was not significant (p = 0.39). Therefore, we concluded that VATS prompts a faster recovery with less pain and trauma in children with CLM. Use of VATS in symptomatic patients was more prone to be converted to thoracotomy. This was due to adhesion and difficulty in dissection in patients with previous chest infections.
According to the results of our study, we recommend the use of VATS in asymptomatic patients to reduce complications, LOS, use of epidural anesthesia, and length of chest drainage. The magnification provided by thoracoscopy improves discrimination between normal and diseased lung tissue and offers better visualization of fissures and vascular structures. 1 However, in symptomatic cases, surgeons should evaluate each individual cautiously to determine whether VATS is feasible, since it is more prone to conversion due to adhesion. In experienced centers, VATS is feasible in neonates or young infants, although thoracoscopic technique and single-lung ventilation can be challenging. Surgeons must be cautious regarding CO2 insufflation on the operative side, and prolonged general anesthesia can lead to hypoxia, hypercapnia, and hemodynamic changes, especially in young infants, which potentially influences the selection of operative approach.
Sensitivity analyses were used to explore the sources of heterogeneity in our study. The sensitivity analysis of operative times suggested a significant reduction in heterogeneity when we removed the studies of Zhang et al. and Lima et al. in turn,31,32 and the pooled estimate remained statistically significant, which indicated a confirmed and robust result. In these two studies, the operative time for VATS was significantly shorter than that of thoracotomy. Their low rate of conversion and advanced thoracoscopic technique may have contributed to these differences. In the sensitivity analysis of LOS, heterogeneity was significantly reduced when we removed the studies of Mahida et al., Lau et al. and Mattioli et al.20,26,27 In their studies,20,26,27 higher symptomatic percentages and more severe complications (i.e., re-intubation and hemorrhage) in patients who underwent thoracotomy yielded much slower recovery. However, the heterogeneity was still significant (I2 = 72%) when we performed leave-one-out sensitivity analyses; therefore, the results with regard to operative times and LOS should be interpreted cautiously. In the sensitivity analysis of length of chest drainage, heterogeneity was also reduced when we removed the studies of Laje et al. and Kunisaki et al.22,24 Heterogeneity was attributed to prolonged air leaks and hemorrhage in these two studies, which contributed to much longer length of chest drainage in the thoracotomy group.
Subgroup analysis was also performed in our current study. In the subgroup analysis of operative times, we observed that, compared with VATS, thoracotomy was associated with shorter operative times in patients younger than 1 year of age. Therefore, to reduce anesthetic and surgical times, thoracotomy might be considered in patients with very young age and critical illness. Besides, in patients with pulmonary sequestration, VATS was found to reduce the LOS in the subgroup analysis. Furthermore, in cohorts with low percentage of symptomatic cases, shorter LOS was also observed using VATS. In patients with CPAM, in patients over 1 year of age, in patients who underwent VATS without conversion, and in patients with low percentage of symptomatic cases, VATS was associated with fewer complications after surgery.
Limitations
Some limitations of our study are acknowledged here. First, all included studies were retrospective and observational; hence our meta-analysis is of low quality. Second, only nine studies had follow-up data in excess of 1 year, so long-term complications remain unknown. Last, since most of our included studies reported different types of CLM and lung resection, heterogeneity across all 23 comparative studies was significant. Therefore, conclusions from this study may not be appropriate to apply to all CLM conditions.
Conclusion
In conclusion, as compared with thoracotomy, VATS is associated with fewer complications, less use of epidural anesthesia, shorter LOS and length of chest drainage, but longer operative times. Symptomatic patients with CLM using VATS may be more prone to conversion to open surgery. However, our study is based on retrospective studies, and our results may not be applied conclusively to all CLM conditions. Larger sample size RCTs should be designed to explore the differences in clinical outcomes between VATS and thoracotomy.
Supplemental Material
sj-pdf-1-tar-10.1177_1753466620980267 – Supplemental material for Is thoracoscopy superior to thoracotomy in the treatment of congenital lung malformations? An updated meta-analysis
Supplemental material, sj-pdf-1-tar-10.1177_1753466620980267 for Is thoracoscopy superior to thoracotomy in the treatment of congenital lung malformations? An updated meta-analysis by Junhua Xie, Yuhao Wu and Chun Wu in Therapeutic Advances in Respiratory Disease
Supplemental Material
sj-pdf-2-tar-10.1177_1753466620980267 – Supplemental material for Is thoracoscopy superior to thoracotomy in the treatment of congenital lung malformations? An updated meta-analysis
Supplemental material, sj-pdf-2-tar-10.1177_1753466620980267 for Is thoracoscopy superior to thoracotomy in the treatment of congenital lung malformations? An updated meta-analysis by Junhua Xie, Yuhao Wu and Chun Wu in Therapeutic Advances in Respiratory Disease
Supplemental Material
sj-pdf-3-tar-10.1177_1753466620980267 – Supplemental material for Is thoracoscopy superior to thoracotomy in the treatment of congenital lung malformations? An updated meta-analysis
Supplemental material, sj-pdf-3-tar-10.1177_1753466620980267 for Is thoracoscopy superior to thoracotomy in the treatment of congenital lung malformations? An updated meta-analysis by Junhua Xie, Yuhao Wu and Chun Wu in Therapeutic Advances in Respiratory Disease
Supplemental Material
sj-pdf-4-tar-10.1177_1753466620980267 – Supplemental material for Is thoracoscopy superior to thoracotomy in the treatment of congenital lung malformations? An updated meta-analysis
Supplemental material, sj-pdf-4-tar-10.1177_1753466620980267 for Is thoracoscopy superior to thoracotomy in the treatment of congenital lung malformations? An updated meta-analysis by Junhua Xie, Yuhao Wu and Chun Wu in Therapeutic Advances in Respiratory Disease
Supplemental Material
sj-pdf-5-tar-10.1177_1753466620980267 – Supplemental material for Is thoracoscopy superior to thoracotomy in the treatment of congenital lung malformations? An updated meta-analysis
Supplemental material, sj-pdf-5-tar-10.1177_1753466620980267 for Is thoracoscopy superior to thoracotomy in the treatment of congenital lung malformations? An updated meta-analysis by Junhua Xie, Yuhao Wu and Chun Wu in Therapeutic Advances in Respiratory Disease
Supplemental Material
sj-pdf-6-tar-10.1177_1753466620980267 – Supplemental material for Is thoracoscopy superior to thoracotomy in the treatment of congenital lung malformations? An updated meta-analysis
Supplemental material, sj-pdf-6-tar-10.1177_1753466620980267 for Is thoracoscopy superior to thoracotomy in the treatment of congenital lung malformations? An updated meta-analysis by Junhua Xie, Yuhao Wu and Chun Wu in Therapeutic Advances in Respiratory Disease
Supplemental Material
sj-pdf-7-tar-10.1177_1753466620980267 – Supplemental material for Is thoracoscopy superior to thoracotomy in the treatment of congenital lung malformations? An updated meta-analysis
Supplemental material, sj-pdf-7-tar-10.1177_1753466620980267 for Is thoracoscopy superior to thoracotomy in the treatment of congenital lung malformations? An updated meta-analysis by Junhua Xie, Yuhao Wu and Chun Wu in Therapeutic Advances in Respiratory Disease
Supplemental Material
sj-pdf-8-tar-10.1177_1753466620980267 – Supplemental material for Is thoracoscopy superior to thoracotomy in the treatment of congenital lung malformations? An updated meta-analysis
Supplemental material, sj-pdf-8-tar-10.1177_1753466620980267 for Is thoracoscopy superior to thoracotomy in the treatment of congenital lung malformations? An updated meta-analysis by Junhua Xie, Yuhao Wu and Chun Wu in Therapeutic Advances in Respiratory Disease
Footnotes
Acknowledgements
We would like to thank Carli Yip (Bellevue College, WA, USA) for grammar and spelling revision.
Author contributions
The literature search was conducted by authors X.J.H. and W.Y.H.; variable selection was performed by X.J.H. and W.Y.H.; data extraction was conducted by X.J.H. and W.Y.H.; various phases of study conceptualization, data analysis, and results interpretation were led by X.J.H., W.Y.H., and W.C. All authors contributed to the preparation, review, and final approval of the manuscript for publication.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Conflict of interest statement
The authors declare that there is no conflict of interest.
Research involving human participants and/or animals
For retrospective studies, ethical approval is waived by Institutional Review Board of Children’s Hospital of Chongqing Medical University. This article does not contain any studies with human participants performed by any of the authors.
Supplemental material
The reviews of this paper are available via the supplemental material section.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.