
Abstract
Background:
Proper adjustment of arterial oxygen saturation (SaO2) during daily activities in patients with interstitial lung disease (ILD) requiring long-term oxygen therapy is challenging. Given the multifactorial nature of the limited exercise tolerance in patients with ILDs, the isolated use of oxygen therapy may not be enough. As demonstrated previously in patients with chronic obstructive pulmonary disease, the use of a noninvasive ventilation (NIV) device combined with oxygen therapy may prevent the falling of oxygen saturation during exercise, due to an improvement of the ventilation–perfusion ratio and a reduction of the respiratory work, thus enhancing exercise tolerance. We sought to assess in patients diagnosed with ILD who are in need of oxygen therapy, the effect of associating an NIV to improve oxygen parameters and the distance covered during the 6 min walking test (6MWT).
Methods:
We conducted a prospective observational study in patients with ILDs. After a clinical characterization, we performed a 6MWT in two different situations: using a portable oxygen concentrator with the regular flow used by the patient during their daily life activities and afterwards adding the additional support of a NIV. The oxygen saturation parameters were registered with a portable oximeter.
Results:
We included 16 patients with different ILDs who have oxygen therapy prescribed. The use of NIV associated with oxygen therapy in comparison with the use of oxygen therapy alone showed an increase of the average SaO2 [91% (88–93) versus 88% (86–90%); p = 0.0005] and a decrease in the percentage of time with oxygen saturation <90%: 36% (6–56%) versus 58% (36–77%); p < 0.0001. There were no changes in the 6MWT distance: 307 m (222–419 m) versus 316 m (228–425 m); p = 0.10.
Conclusions:
In our study the use of a NIV system associated with long-term oxygen therapy during exercise showed beneficial effects, especially improvement of oxygen saturation.
The reviews of this paper are available via the supplemental material section.
Introduction
Diffuse interstitial lung diseases (ILDs) are a heterogeneous group of respiratory pathologies characterized by inflammation and subsequent fibrosis of the space located between the basal membrane of the alveolar epithelium and the capillary endothelium. Their natural history entails, in most cases, a progressive clinical, radiological and functional deterioration, progressing to lung fibrosis over the subsequent years. ILD incidence is 26–32 cases/100,000 and they are associated with high morbidity and mortality. 1 Dyspnea is the most common symptom and, for most patients the most crippling one, 2 often accompanied by unproductive cough. The onset of the symptoms is slow but usually presents a progressive worsening over the years.
The presence of dyspnea of multifactorial origin is the main symptom presented by patients that limits the performance of their daily activities and involves a significant deterioration of their quality of life, affecting their social and personal environment. This is explained by a limitation on exercise, generated by an impaired arterial oxygenation. 3 The main mechanism causing pulmonary arterial hypoxemia in patients with ILDs is the imbalance in the ventilation–perfusion ratio (VA/Q) due to the interstitial space occupation and progressive destruction of alveolar units, as well as the limitation of oxygen diffusion from the alveoli into the capillaries. 4 Patients with ILDs present an excessive increase in respiratory rate during exercise, with less recruitment of tidal volume (Vt), in addition to an increased dead space/tidal volume ratio (RV/Vt). These factors explain the drop in PaO2 induced by exercise in patients with ILDs and is one of the main factors related to poor prognosis.5,6
The Royal College of Physicians recommends long-term oxygen therapy (LTOT) in patients with ILDs presenting a PaO2 < 60 mmHg at rest (FiO2 of 0.21) or those showing an oxygen saturation by pulse oximetry of <90% during the 6-min walking test (6MWT). 7 Oxygen therapy has also been recommended by the international guidelines of diagnosis and treatment for idiopathic pulmonary fibrosis (IPF) based on pathophysiological concepts and data extrapolated from patients with chronic obstructive pulmonary disease (COPD). A retrospective study of patients with different ILDs showed that home oxygen increased exercise tolerance and decreased dyspnea.8,9 Recently, a clinical trial (the AmbOx study) has demonstrated that ambulatory oxygen could improve health-related quality of life. 10
Moreover, given the multifactorial nature of the low exercise tolerance in patients with ILDs, the standard use of home supplemental oxygen therapy could not solve the whole problem. In COPD patients, multiple therapies have been described to solve this aspect. Porszasz and colleagues 11 evaluated the physiological effects of a portable noninvasive ventilator (NIV) device, designed to be used in conjunction with home oxygen therapy, in patients with COPD presenting significant falls in SaO2 during exercise. This device was designed to facilitate ambulation and activities of daily living, delivering only up to 250 ml volume. Other studies in COPD using regular NIV device in addition to oxygen therapy12,13 also showed a significant increase in arterial oxygen after performing physical effort as well as an improvement of dyspnea perception. These studies showed that the use of a NIV connected to oxygen increased exercise tolerance and significantly decreased dyspnea compared to traditional nasal prongs. The mechanism by which this device could improve respiratory parameters was related to achieving more efficient ventilation, a lower respiratory rate, reduced activation of respiratory muscles, and higher average SaO2 compared to standard devices. 11
Accordingly, we consider that the use of a noninvasive ventilator could lead to an improvement in respiratory dynamics in ILD patients due to an enhancement in ventilation–perfusion ratio and oxygenation parameters. This would imply a major advance in tolerance to physical exertion, a decrease in the patient’s sensation of dyspnea, and could possibly upgrade the effect of rehabilitation in patients with ILDs who require oxygen therapy. Our aim in this study was to assess whether the additional support provided by a NIV system could improve oxygenation parameters and exercise tolerance in patients with ILDs and home supplemental oxygen therapy.
Materials and methods
Study design and population
This was a prospective observational study carried out at the ILD Unit at Hospital Clínic, Barcelona. This study was approved by the Ethics Committee of our institution (HCB/2014/0480). Each patient was asked for written informed consent to participate in the study.
We included ILD patients who were under LTOT for at least 12 weeks prior to the onset of the study. We excluded patients for the following reasons: inability to conduct a 6MWT or a previous test with a distance achieved <150 m; pulmonary hypertension requiring specific drug treatment or systolic pulmonary artery pressure estimated by echocardiography >50 mmHg; severe cardiac disease or systemic muscle disease that may limit the effort of the patients; history of neoplastic disease treated with chemotherapy or accompanied by cachexia in the previous 2 years; concomitant diagnosis of COPD or asthma or spirometry with forced expiratory volume in 1 s (FEV1)/forced vital capacity (FVC) < 0.70; prior hospitalization for acute worsening of their lung condition in the last 12 weeks prior to the onset of the study; and respiratory infection in the 4 weeks prior to the study. All the patients were presented in our multidisciplinary discussion session. All diagnoses were established following standard guidelines.14–16
Study protocol
We scheduled an initial visit for eligible patients at the ILD unit in which we collected information about clinical and functional variables. The characteristics of the study and how the pulse oximeter worked were explained. The patient’s baseline dyspnea was assessed with the modified Medical Research Council dyspnea scale and their quality of life with the Saint George’s respiratory questionnaire test (Spanish version). 17 Subsequently two interventions were performed: (1) 6MWT with oxygen therapy (O2), using the same flow prescribed at home and (2) 6MWT with O2 and the additional support of a noninvasive ventilator (O2 + NIV). Before the second exercise, patients had a rest period of at least 1 h between the two 6MWTs and underwent an adaptation period of about 30 min with the ventilator. The Borg scale was used at the beginning and the end of the 6MWT to determine the level of dyspnea and muscle fatigue of the patients. As we wanted to avoid the effect of carrying the NIV and oxygen system by the patients on 6MWT, in both tests they were carried by an additional respiratory physician during the 6MWT.
Monitoring of arterial oxygenation was performed using a wrist pulse oximeter that comfortably allows continuous monitoring of SatO2 for the patient during daily living activities and the 6MWT (NONIN WristOx2 3150; Noning Medical). The system also has a large memory and the ability to download information from the study using the software for further analysis. Average O2 saturation (SaO2), initial and final, percentage of time with oxygen saturation <90% (CT90), and <85% (CT85) were calculated. ΔSaO2 was the difference between final and initial SaO2 in each patient.
For the second 6MWT, a noninvasive two-level positive pressure ventilator (BIPAP) model Stellar 150 ResMed® was connected to a standard oxygen tank using a T-piece located at the end of the tube closest to the ventilator (Figure 1). The oxygen flow used was the same already prescribed for each patient for the performance of their daily life activities. Expiratory pressure (EPAP) of 4 cmH2O and a variable inspiratory pressure (IPAP) were set to achieve approximately a Vt of 8–10 ml/kg, adjusted according to patient comfort. The respiratory mode was spontaneous (S) with a range of inspiratory time between 0.5 s (Tinsp minimum) and 2 s (Tinsp maximum). An oronasal mask where the leak was located was the interface used for all patients. FiO2 was not calculated in our study; its value would depend on the ventilatory pattern of the patients, tolerated inspiratory pressure and oxygen flow administered.

Photograph of the noninvasive ventilation system used in the study with an orofacial mask connected to an oxygen tank by a T-piece adapter at the proximal end of the tubing.
Statistical analysis
The primary endpoint of our study was oxygen saturation parameters (average SatO2 and CT90) while performing the 6MWT. Assuming that with NIV, it would be possible to reduce 20 ± 26% of CT90 in patients with ILD, at least 16 patients would be necessary. A significance level of 5% and a power of 80% were assumed.
Categorical variables were summarized with counts and percentages. For continuous variables, the median (25–75th percentile) were presented. Wilcoxon nonparametric tests were used for paired comparisons. The level of significance was set in all tests at 0.05 (all two-tailed). The graphs and the statistical analyses were performed using Prism 8 for MacOS (version 8.3.0, 1994–2019, GraphPad Software, LLC).
Results
A total of 16 patients with different ILDs were included in the study, IPF being the most frequent (31%). In addition, six patients also presented with connective tissue disease (CTD). From these patients, three patients were classified as CTD-ILD [nonspecific interstitial pneumonia (NSIP) associated with systemic sclerosis, NSIP associated with anti-synthetase syndrome and usual interstitial pneumonia (UIP) associated with rheumatoid arthritis]. All patients were functionally limited and needed LTOT for daily activities. Baseline characteristics of all patients are shown in Table 1.
Baseline characteristics of patients (n = 16).

Baseline characteristics of patients including pathological background, ILD diagnosis, functional parameters, current treatment and hours of oxygen therapy.
CHP, chronic hypersensitivity pneumonitis; COP, chronic organizing pneumonia; CTD, connective tissue disease; DIP, desquamative interstitial pneumonia; DLCO, lung diffusion capacity for carbon monoxide, FVC, forced vital capacity; FEV1, forced expiratory volume in 1 s, IPF, idiopathic pulmonary fibrosis; IS, immunosuppressant; mMRC, modified Medical Research Council dyspnea scale; NSIP, nonspecific interstitial pneumonia; PFT, pulmonary function test; SGRQ, Saint George’s respiratory questionnaire; TLC, total lung capacity.
Plus/minus values represent means and standard deviation.
The majority of patients developed similar physical exercise in both 6MWT independently if they were using the NIV on top of the LTOT, as suggested by the similar distance walked [O2: 316 m (228–425 m), O2+NIV: 307 m (222–419 m); p = 0.10; Figure 2] and the similar changes in physiological parameters in both tests (Figure 3). However, it is remarkable that there was an improvement in all the parameters associated with oxygen saturation: (1) a decrease in CT90 [O2: 58% (36–77%), O2+NIV: 36% (6–56%); p < 0.0001] and CT85 [O2: 25% (2–65%), O2+NIV: 20% (0–3%9); p = 0.0007] after the use of NIV; (2) a lower fall of SaO2 [ΔSaO2 = O2: −12% (−20 to 8%), O2+NIV: −7% (−18 to 3%); p = 0.0009] from the basal condition previous the onset of the 6MWT [96% (94,25–96,75%)]; and (3) an increase of average SaO2 [O2: 88% (86–90%), O2+NIV: 91% (88–93%); p = 0.0005; Figure 2]. As both tests were performed using the same oxygen flow, these data suggest that NIV could provide an optimization of the oxygen therapy effect on oxygen saturation.

Comparison of oxygen saturation parameters and total meters covered during the 6MWT, between oxygen therapy alone and with additional support of a noninvasive ventilator. There were no significant changes in the total distance covered during the performance of the 6MWT. However we observed a remarkable improvement of oxygen saturation parameters with the additional use of a noninvasive ventilator: a decrease of CT90 and CT85 as well as a lower fall of the SaO2 and an increase of mean oxygen saturation.
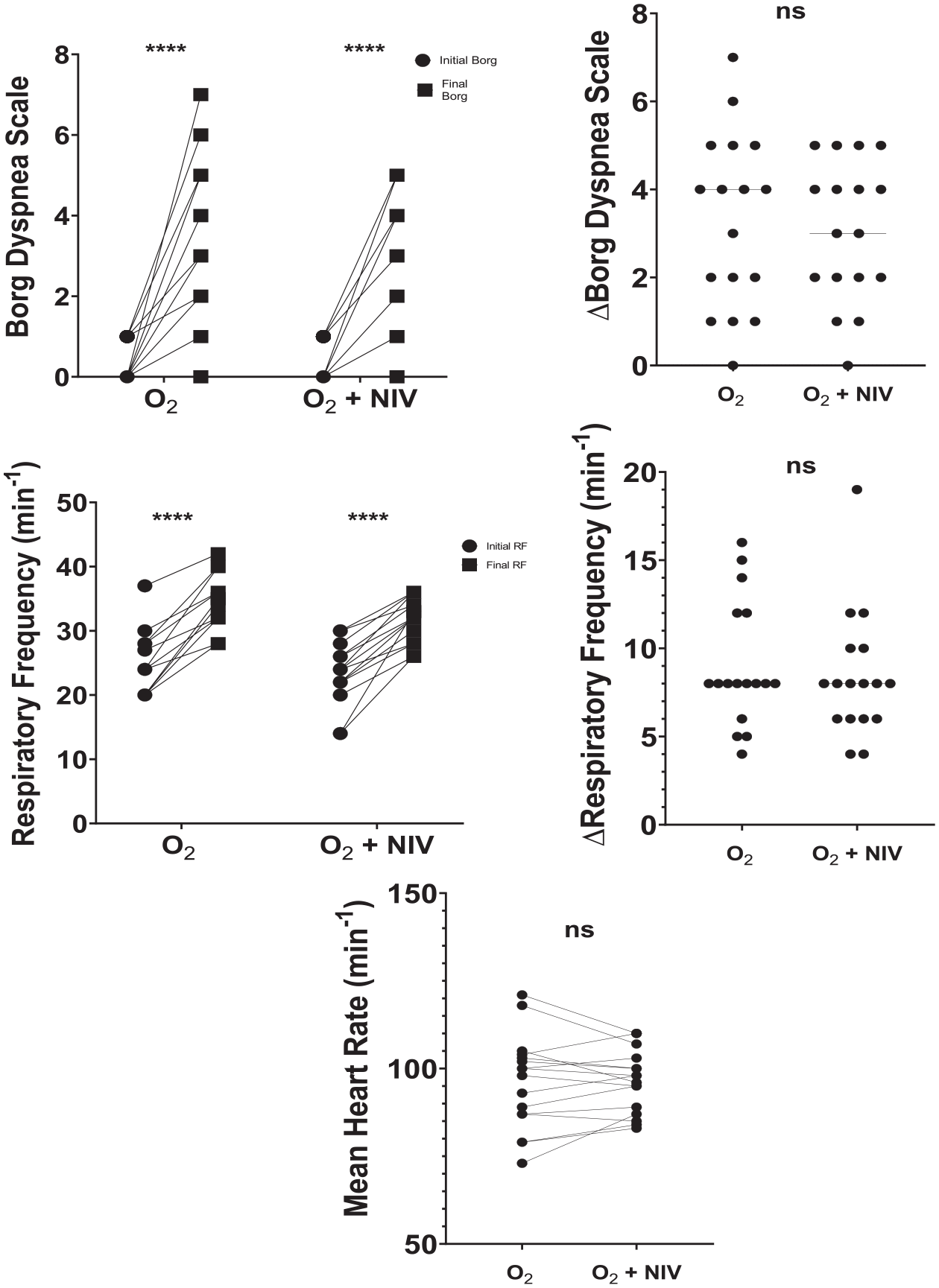
Comparison of physiological parameters (heart and respiratory rate) and dyspnea level assessed with Borg scale in patients with ILD with oxygen therapy alone and with additional support of a noninvasive ventilator.
Dyspnea measured with Borg scale were similar in both tests [Figure 3; 4 (2–4, 75), p < 0.0001] with O2+NIV compared with the O2 test [4 (2–5), p < 0.0001]; [ΔBorg = O2: 4 (1.5–5), O2+NIV: 3 (2–4.5); p = 0.43].
The average IPAP used under NIV in our study was 12 (10–16) cmH2O. In all patients, an improvement in respiratory parameters was observed with an increase in median tidal volume [from 654 ml (500–770 ml) to 870.5 ml (729–1076 ml), p < 0.0001] and minute volume [from 14.03 l/min (12.07–17.83 l/min) to 26.96 l/min (24.41–35.38 l/min), p < 0.0001] with the support of the NIV compared with basal conditions at rest before the onset of the exercise.
Discussion
The result obtained in our study seems to demonstrate the favorable effect of associating a NIV with oxygen therapy to improve the oxygen saturation parameters during 6MWT without increasing the oxygen flow.
Current home supplemental oxygen devices have specific limitations, especially in patients with ILDs that characteristically develop a significant fall of SaO2 during exercise and need higher flows of oxygen to maintain an adequate level of SaO2. 3 The flow administered by portable oxygen devices are limited and sometimes do not satisfy patients’ needs.18,19
We hypothesized the improvement of oxygen saturation parameters to the additional effect of positive pressure in the airway, similarly to the studies of Porszasz and colleagues in COPD. 11 In their study, 15 patients diagnosed with COPD (FEV1: 32±12%) performed an exercise test using a cycloergometer with a progressive increase in exercise intensity up to 80% of the peak load in several situations: ambient air, with oxygen therapy support, NIV with ambient air and NIV combined with oxygen therapy. The results showed a significant improvement of the average oxygen saturation in the group of NIV associated with oxygen therapy in comparison with oxygen therapy alone (97.4±1.8 versus 91.2±4.2), as well as a greater tolerance to exercise assessed by a sustained physical activity over a longer period of time (17.6±5.7 min versus 11.4±6.8 min). Other studies in patients with COPD showed similar results. Dreher et al. performed two studies: in the first study 12 a total of 20 patients with COPD reporting dyspnea during mild exertion underwent two 6MWTs with supplemental oxygen therapy in a randomized cross-over design: with and without pressure-limited NIV. The results showed a significant increase in the arterial oxygen after performing a walking test with NIV as well as an improvement of dyspnea assessed by the Borg scale and total walking distance. In the second study, 13 11 patients diagnosed with severe COPD (FEV1 of 26±9%) underwent three 12-min walking tests in a randomized cross-over design on three consecutive days, comparing the usual and double dosages of oxygen versus NIV plus the usual dosage of oxygen. The use of NIV showed improvement of PaO2 compared with the usual dosage of oxygen. Changes in FEV1, Vt and inspiratory impedance were in favor of NIV-aided exercise; however, dyspnea and walking distance were not improved due to the burden of carrying the heavy ventilatory equipment in a backpack.
In patients with ILDs the main pathophysiological mechanisms of desaturation are both an imbalance in the ventilation–perfusion ratio due to progressive destruction of alveolar units and a limitation of oxygen diffusion caused by inflammation and occupation of interstitial space. Our hypothesis is that the use of a NIV could enhance the recruitment of Vt as well as improve respiratory parameters, achieving a better VA/Q-matching in our patients, leading to an increased oxygenation, especially during exercise. This hypothesis needs further validation in new studies.
In our case, with a similar walking distance in both tests, patients showed an improvement in oxygen saturation parameters with the combination of oxygen therapy and NIV. To our knowledge, no previous studies have assessed the relevance of CT90 in ILDs, but in COPD, CT90 is a useful parameter to monitor oxygen saturation during exercise. 20 As 6MWT is the current method to titrate oxygen flow for daily activities, the potential use of NIV to optimize flow titration in exercise could be relevant as a future application.
Several limitations should be addressed. Firstly, due to the characteristics and the physical exercise needed to perform the 6MWT, we excluded those patients with physical limitations derived from their lung disease as well as severe cardiac conditions or muscle involvement. This may lead to a selection bias as the most severely affected patients could not be included. However, we hypothesized that the results obtained might also apply to them. In the future we plan to include patients with a more severe stage of pulmonary involvement to research the potential beneficial effect of the noninvasive ventilation. Secondly, we monitored oxygen flow and positive pressure administered during the performance of the 6MWT with the NIV as well as the oxygen saturation variations along the exercise but delivered FiO2 was not determined. Thirdly, this is a pilot study to assess the potential use of NIV with ambulatory oxygen during 6MWT. However, these results should be confirmed during ambulatory daily activities with a NIV+O2 system that could be easily and routinely used by patients.
In conclusion, our study seems to indicate that the additional use of a NIV device associated with oxygen therapy during the performance of the 6MWT may have a potential benefit in oxygen saturation parameters. However, given the current limitations discussed above, we believe additional studies should be carried out in order to properly assess its beneficial effect in daily activities.
Supplemental Material
Author_Response_1 – Supplemental material for Improving home oxygen therapy in patients with interstitial lung diseases: application of a noninvasive ventilation device
Supplemental material, Author_Response_1 for Improving home oxygen therapy in patients with interstitial lung diseases: application of a noninvasive ventilation device by Sandra Cuerpo, Maria Palomo, Fernanda Hernández-González, Joel Francesqui, Nuria Albacar, Carmen Hernández, Isabel Blanco, Cristina Embid and Jacobo Sellares in Therapeutic Advances in Respiratory Disease
Supplemental Material
Author_Response_2 – Supplemental material for Improving home oxygen therapy in patients with interstitial lung diseases: application of a noninvasive ventilation device
Supplemental material, Author_Response_2 for Improving home oxygen therapy in patients with interstitial lung diseases: application of a noninvasive ventilation device by Sandra Cuerpo, Maria Palomo, Fernanda Hernández-González, Joel Francesqui, Nuria Albacar, Carmen Hernández, Isabel Blanco, Cristina Embid and Jacobo Sellares in Therapeutic Advances in Respiratory Disease
Supplemental Material
Reviewer_1_v.1 – Supplemental material for Improving home oxygen therapy in patients with interstitial lung diseases: application of a noninvasive ventilation device
Supplemental material, Reviewer_1_v.1 for Improving home oxygen therapy in patients with interstitial lung diseases: application of a noninvasive ventilation device by Sandra Cuerpo, Maria Palomo, Fernanda Hernández-González, Joel Francesqui, Nuria Albacar, Carmen Hernández, Isabel Blanco, Cristina Embid and Jacobo Sellares in Therapeutic Advances in Respiratory Disease
Supplemental Material
Reviewer_2_v.1 – Supplemental material for Improving home oxygen therapy in patients with interstitial lung diseases: application of a noninvasive ventilation device
Supplemental material, Reviewer_2_v.1 for Improving home oxygen therapy in patients with interstitial lung diseases: application of a noninvasive ventilation device by Sandra Cuerpo, Maria Palomo, Fernanda Hernández-González, Joel Francesqui, Nuria Albacar, Carmen Hernández, Isabel Blanco, Cristina Embid and Jacobo Sellares in Therapeutic Advances in Respiratory Disease
Supplemental Material
Reviewer_2_v.2 – Supplemental material for Improving home oxygen therapy in patients with interstitial lung diseases: application of a noninvasive ventilation device
Supplemental material, Reviewer_2_v.2 for Improving home oxygen therapy in patients with interstitial lung diseases: application of a noninvasive ventilation device by Sandra Cuerpo, Maria Palomo, Fernanda Hernández-González, Joel Francesqui, Nuria Albacar, Carmen Hernández, Isabel Blanco, Cristina Embid and Jacobo Sellares in Therapeutic Advances in Respiratory Disease
Footnotes
Acknowledgements
We dedicate this manuscript to the memory and the contribution of our co-author and friend Antoni Xaubet. We also thank the respiratory therapy and nursing staff, and the physicians attending the respiratory department, for their cooperation in this study. We thank Dr. Josep Roca and Dr. Alvar Agustí for helping the investigators to initiate the study.
Author contribution(s)
Availability of data and materials
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Conflict of interest statement
The authors declare that there is no conflict of interest.
Ethics approval and consent to participate
This study was approved by the Ethics Committee of our institution (HCB/2014/0480). Each patient was asked for written informed consent to participate in the study.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work has been financed with the grant SLT008/18/00176 and the support of the Department of Health of the Generalitat de Catalunya, in the call for grants 2019–2021, under a competitive regime, for the financing of different programs and instrumental actions included in the Strategic Research and Innovation Plan in Health 2016–2020. It has also been financed by FEDER Funds (PI19/01152), SEPAR, SOCAP, FUCAP and with the PhD4MD Programme of the Institute for Research in Biomedicine Barcelona, Hospital Clínic of Barcelona and the Institut d’Investigacions Biomèdiques August Pi i Sunyer (IDIBAPS).
Supplemental material
The reviews of this paper are available via the supplemental material section.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.