
Abstract
Objectives:
The objective of this study was to determine the performance of preoperative 6-minute walk test (6MWT) for predicting postoperative pulmonary complications (PPC) in high risk patients undergoing elective surgery under general anesthesia.
Methods:
A prospective cohort study was conducted in patients scheduled to undergo elective thoracic or nonthoracic surgery and indicated for preoperative pulmonary evaluation in Songklanagarind Hospital, Songkhla, Thailand. Preoperative spirometry, 6MWT were done and 30-day PPC were recorded. The multiple regression analysis and receiver operating characteristic (ROC) curves were used to analyze the variables and to compare the performance of 6MWT and spirometry tests.
Results:
A total of 78 participants were recruited into the study. 6MWT was done completely in all cases without any complications. Among these tests, 14 cases (17.9%) had contraindications to spirometry and two cases were unable to achieve the criteria for acceptable efforts. PPC developed in 17 cases (21%) with a high mortality (17.7%). A multiple regression analysis showed elderly, poor general health status, smoking history, low level of the mean value of forced expiratory volume in 1 second (FEV1) % predicted (by spirometry) and shorter 6-minute walk distance (6MWD) were the independent factors associated with PPC. Patients developing PPC had a significantly lower preoperative 6MWD compared with patients without PPC (256.0 ± 48.0 versus 440.0 ± 117.1 meters, p < 0.001). 6MWD of ⩽325 meters was a threshold for predicting PPC with 77% sensitivity and 100% specificity, and had a good predictive value for PPC similar to that for the FEV1 %.
Conclusions:
Preoperative 6MWT is a very useful alternative test for predicting PPC in high risk patients scheduled to undergo surgery under GA.
Introduction
Postoperative pulmonary complications (PPC) are a common problem and a major cause of perioperative morbidity, mortality, longer hospital stays [Smetana et al. 2006; Smetana, 1999; Lawrence et al. 1995]. Estimated incidence of PPC varies from 2% to 40% with a mortality rate up to 10% [Canet et al. 2010; Sogame et al. 2008; Rudra and Das, 2006; Fisher et al. 2002]. The major categories of PPC include atelectasis, bronchitis, pneumonia, exacerbation of chronic lung diseases, bronchospasm, prolonged mechanical ventilation (MV) and acute respiratory failure (ARF) [Canet and Mazo, 2010; Smetana et al. 2006; Warner, 2000; Smetana, 1999].
Preoperative spirometry and cardiopulmonary exercise testing (CPET) are the standard tests for predicting PPC risk. The forced expiratory volume in 1 second (FEV1) and forced vital capacity (FVC) by spirometry of <60–70% predicted or the maximal oxygen uptake (VO2 max) by CPET below 10 ml O2/kg/min could identify a high risk of PPC [Mezzani et al. 2009; Albouaini et al. 2007; Wang, 2004]. However, these tests have their own limitations such as complexity, need for more equipment, cost, discomfort, contraindications and lack of availability of institutional and local expertise. Therefore, a simplified useful test for predicting the chance of PPC is now sought.
Since 1982, the 6-minute walk test (6MWT), which analyzes the 6-minute walk distance (6MWD), was developed as a simple, noninvasive, inexpensive test with minimal technological requirement and had broad applications for the objective valuation of submaximal functional exercise capacity. It evaluates the global and integrated responses of all the body systems involved during the exercise [Morales-Blanhir et al. 2011; American Thoracic Society, 2002; Solway et al. 2001; Butland et al. 1982]. Various studies had shown that the 6MWT was valid and reproducible, and demonstrated a high positive association between a 6MWD of <427 meters (m) and a VO2 max <11 ml O2/kg/min in patients with cardiopulmonary diseases [Casillas et al. 2013; Lee et al. 2013; Sinclair et al. 2012; Guimarães et al. 2008; Knox et al. 1998]. Therefore, the 6MWT was used for monitoring the treatment response and establishing the prognosis of cardiopulmonary diseases [Nathan et al. 2015; Miyamoto et al. 2000; Cahalin et al. 1996; Wijkstra et al. 1994].
In the context of preoperative assessment, in 1992, the 6MWT was used by Holden and colleagues as the predictor of postoperative mortality in 16 cases with resectable lung cancer. Results showed a 6MWD of <304 m had 100% sensitivity for predicting postoperative death [Holden et al. 1992]. After that, in 1997, Szekely and colleagues undertook a retrospective study in 47 patients undergoing lung volume reduction surgery and found that a 6MWD of <200 m was a better predictor of postoperative death and hospital length of stay (LOS) than FEV1 % predicted [Szekely et al. 1997].
Recently, in 2015, Awdeh and colleagues conducted a prospective study in 117 patients undergoing major surgery and showed that a preoperative 6MWD of ⩽300 m was associated with postoperative LOS and some categories of PPC (atelectasis, pneumonia and prolonged MV) [Awdeh et al. 2015]. Conversely, a study by Paisani and colleagues in 2012 found no correlation between preoperative 6MWD and risk of PPC in patients who underwent upper abdominal surgery (UAS) [Paisani et al. 2012].
As mentioned above, there have been limited and sometimes conflicting data in the usefulness and cutoff level of preoperative 6MWD for predicting PPC, especially in the high risk patient groups. Therefore, the present study was conducted to identify the value of preoperative 6MWD in predicting PPC in high risk patients who are indicated for preoperative pulmonary evaluation (PPE) before undergoing elective surgery under general anesthesia (GA).
Materials and methods
A prospective cohort study was conducted from March to August 2013 at the Songklanagarind Hospital, Songkhla, Thailand. Inclusion criteria included:
Patients 18 years of age or older admitted to the Department of Surgery and planned for either elective thoracic or nonthoracic surgery (upper abdomen or major surgical procedures lasting more than 3 hours) under GA;
Patients having at least one of these potentially PPC risk factors [age at least 60 years old; history of cardiopulmonary disease, stroke, obstructive sleep apnea, malnutrition or poor general health status as defined by American Society of Anesthesiologists (ASA); physical status class >2; cigarette use within previous 8 weeks; arterial oxygen desaturation (SO2) <95% or tension of carbon dioxide >45 mmHg; abnormal chest X-ray] that indicated PPE as the general standard of care [Vasu et al. 2012; Canet et al. 2010; Sogame et al. 2008; Rudra and Das, 2006; Smetana et al. 2006; Wang, 2004; Fisher et al. 2002; Smetana, 1999]; and
Patients undergoing the 6MWT within 3 days prior to surgery.
Patients with recent acute coronary syndrome, uncontrolled hypertension and cardiac diseases, pregnancy, a condition which impaired walking (e.g. joint muscle pain, arthritis, paresis) and incomplete 6MWT were excluded from the study.
After the history, physical examinations and laboratory tests were taken [e.g. complete blood counts, blood chemistry tests, anti-human immunodeficiency virus (HIV), chest X-ray, electrocardiography and echocardiography], patients were instructed about the PPE planning and signed informed consent forms.
Thereafter, preoperative chest physical therapy was given (deep breathing and coughing exercises); spirometry was performed and followed with the 6MWT on the same day. The third National Health and Nutrition Examination Survey (NHANES III) reference was used for interpreting spirometry results [Hankinson et al. 1999] and the 6MWT was performed indoors along a flat surface in a straight corridor 30 m long, with 180 degree turns every 30 m according to the standard protocol as per American Thoracic Society guidelines [American Thoracic Society, 2002]. The walk test was performed on room air or supplemental oxygen to maintain SO2 >90% up to a maximum of 6 minutes and monitored by trained nurses who were certified in cardiopulmonary resuscitation (CPR) and supervised by the physician. The vital signs and SO2 were monitored before and at the end of the test. Adverse events were monitored during and after finishing the test. If any of the followed symptoms occurred (chest pain, intolerable dyspnea, leg cramps, staggering, diaphoresis and ashen appearance), the walk test was terminated and interpreted as an incomplete test. The patients’ functional status and the spirometry results were used to determine operability. The decision to perform surgery was made jointly by the primary surgeon and pulmonologist, who were blinded to the 6MWT results.
After surgery, all patients received once daily postoperative chest physical therapy (postural drainage, position rotation, deep breathing and coughing exercises) until discharge. The postoperative LOS and PPC occurring during the admission or house calls within 30 days after the operation were recorded by the pulmonary physician who was also blinded to the 6MWD. PPC was defined as of the following:
Atelectasis: radiological evidence of atelectasis associated with dyspnea requiring medical or bronchoscopic interventions
Bronchitis: excessive of purulent sputum with fever (body temperature >38ºC) in normal chest X-ray
Pneumonia: chest X-ray showed new and persistent of lung infiltration at least for 2 days associated with at least 2 of the following criteria (fever, purulent sputum and leukocytosis)
Exacerbation of chronic lung diseases
Prolonged MV >48 hours after the operation
ARF: evidence of either oxygenation or ventilation failure needing invasive or noninvasive MV at least 48 hours
We hypothesized that patients with a shorter preoperative 6MWD will be more likely to develop PPC. Therefore, this study aimed to determine whether the 6MWT is a useful predictor of PPC. Moreover, the performance of the three parameters (6MWD, FEV1 % predicted and FVC % of predicted) in predicting the risk of PPC were compared. The study protocol was approved by the Ethics Committee of the institution (IRB#56-180-14-4-3) and was conducted in accordance with the World Medical Association Declaration of Helsinki and good clinical practical guideline, 2013.
Statistical analysis
The samples size was calculated using the two independent means formula for unequal group sizes [Hulley et al. 2001]. A sample size of 16 cases was required in the PPC group and 62 cases in the non-PPC group, giving a total sample size of 78 cases, in order to detect a difference higher than 100 m of 6MWD between groups, expecting an incidence of PPC of 20%, standard deviation (SD) of 100 m, assuming α = 0.05 and 80% power of detection. The mean (SD) was used to describe continuous data. Proportion (%) was used to describe categorical data. Student’s t-test and the chi-squared test were used to analyze the continuous and categorical characteristics, respectively. The clinical, test variables and 6MWD were compared between the two groups using univariate and multiple regression analysis. The discrimination of PPC by spirometry and 6MWD was determined by receiver operating characteristic (ROC) curves. The outcomes of interest were analyzed with STATA version 13 software and the results were considered as statistically significant if the p value was<0.05.
Results
A total of 78 patients undergoing elective surgery under GA and indicated for PPE were recruited and all completed the 6MWT without any contraindications or adverse events. Among this, 16 cases (21%) had no the spirometry results due to contraindications in 14 cases (13 vascular aneurysms, 1 recent pneumothorax) and were unable to achieve the criteria for acceptable efforts in two cases. Of the total 78 patients, 17 cases (21.8%) developed PPC (7.7% pneumonia, 6.4% atelectasis, 3.8% ARF and 3.8% developed exacerbation of chronic lung diseases). Of the 17 PPC cases, three (17.7%) died in the hospital from pneumonia and ARF. The PPC group had significantly higher postoperative LOS (20.4 ± 3.2 versus 11.5 ± 2.6, p = 0.03) and higher mortality rate (17.7% versus 0, p = 0.02) compared with the non-PPC group. The PPC group had a statistically significant higher age (69.5 ± 7.2 versus 59.5 ± 8.4, p < 0.001) and higher percentage of ASA class >2 (76.5% versus 45.9%, p = 0.02), smoking (82.4% versus 55.7%, p = 0.04) and underlying diseases (100% versus 62.3%, p = 0.003) compared with patients in the non-PPC group (Table 1).
Baseline characteristics of patients in the PPC and non-PPC groups.

American Society of Anesthesiologists physical status classification I–V.
BMI, body mass index; PPC, postoperative pulmonary complications; SD, standard deviation; N, number; n, percent.
Results showed there was a negative correlations between the mean value of FEV1 % predicted, FVC % predicted and 6MWD with the chance of PPC. Patients developing PPC had a lower FEV1 % predicted (59.3 ± 9.4 versus 82.4 ± 11.8), FVC % predicted (76.9 ± 6.6 versus 86.3 ± 7.0) and 6MWD (256.0 ± 48.0 versus 440.0 ± 117.1, all p < 0.001) compared with subjects without developing PPC, respectively (Table 2).
Level of 6MWD, FEV1 and FVC % predicted between patients developed PPC and non-PPC groups.

6MWD, 6-minute walk distance; FEV1, forced expiratory volume in 1 second; FVC, forced vital capacity; PPC, postoperative pulmonary complications; SD, standard deviation; N, number.
Preoperative 6MWD of ⩽325 m was selected as the threshold for predicting the PPC risk, with a sensitivity of 77%, specificity of 100% and area under the ROC curve (AUC) of 0.94 (Figure 1). The study showed there was no PPC incurred in patients with a preoperative 6MWD > 325 m despite FEV1 < 60% predicted. A multiple regression analysis showed that 6MWD ⩽325 m, FEV1 <60% predicted, elderly, ASA class >2 and smoking history were strongly independent predictors for PPC, but there was no associations between FVC <60% predicted and an FEV1/FVC ratio of <70% with the PPC chance (Table 3). According to the performance of three parameters in discriminating PPC (represented by AUC), the results showed that 6MWD was a good prognostic parameter equal to FEV1 % predicted for predicting the risk of PPC (0.94 versus 0.93, p = 0.06), but significantly better than FVC % predicted by spirometry (0.94 versus 0.83, p = 0.04) (Figure 2).
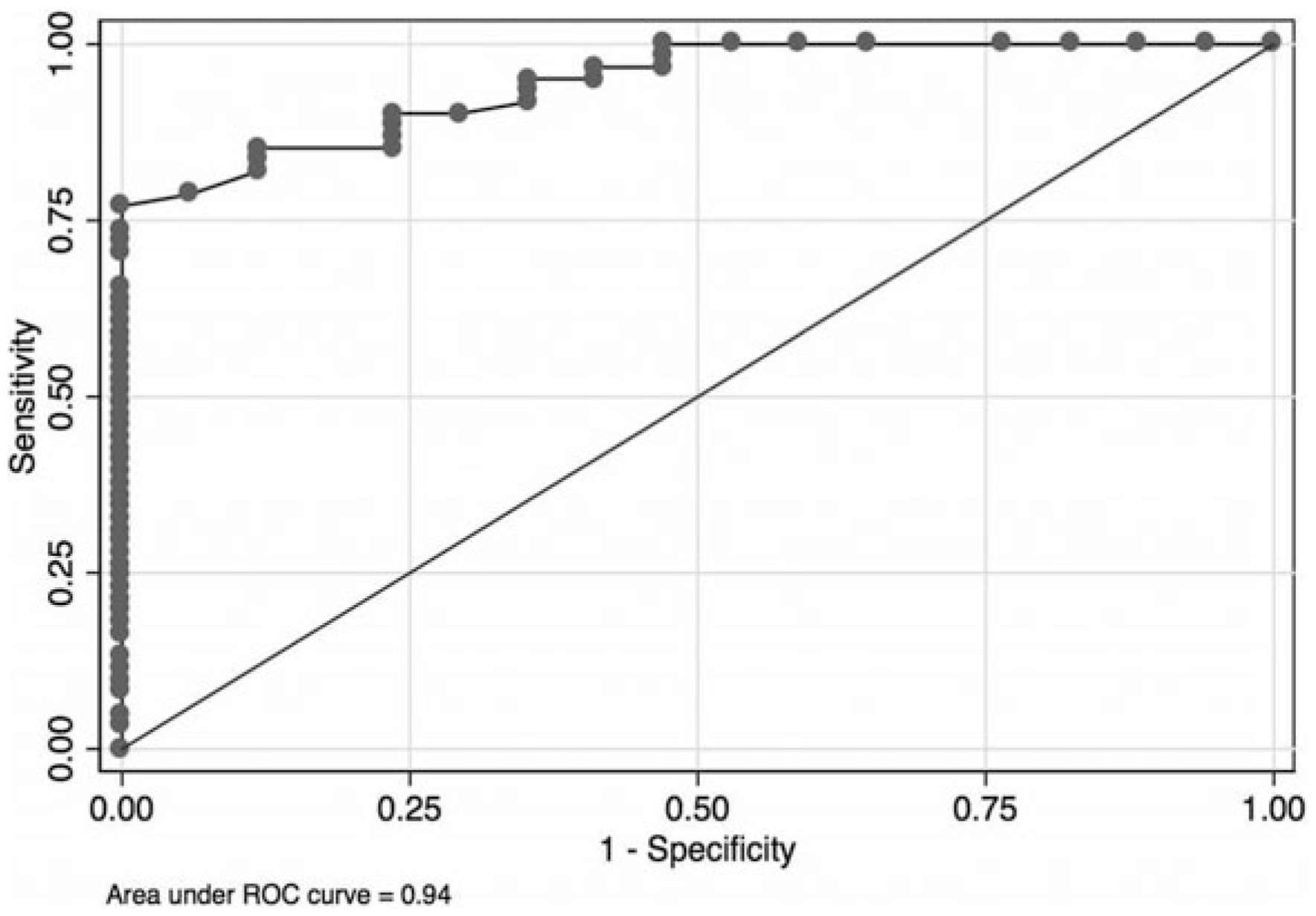
Sensitivity, specificity and area under the ROC curve of 6MWD for predicting PPC.
PPC predictive value of clinical and test variables by multiple regression analysis.

CI *American Society of Anesthesiologists physical status classification 2
6MWT, 6-minute walking test; FEV1, forced expiratory volume in 1 second; FVC, forced vital capacity; PPC, postoperative pulmonary complications; SD, standard deviation.

Area under the ROC curves for PPC risk determined by 6MWD, FEV1 and FVC % predicted.
Discussion
This study found that the 6MWT was a safe and useful test for predicting the chance of PPC in high risk patients who were to undergo elective surgery under GA. Furthermore, the 6MWT had an equal performance in PPC prediction to FEV1 % predicted, but was significantly better than FVC % predicted by spirometry test.
PPC prolongs hospital LOS and increases perioperative mortality, especially in high risk patients who are indicated for PPE [Canet et al. 2010; Sogame et al. 2008; Rudra and Das, 2006; Smetana et al. 2006; Fisher et al. 2002; Smetana, 1999; Lawrence et al. 1995]. To date, preoperative spirometry and CPET are the standard tests for PPC risk assessment; however, both tests have many limitations as previously mentioned [Mezzani et al. 2009; Albouaini et al. 2007; Wang, 2004]. The 6MWT analyzed for 6MWD is a simple, noninvasive, safe, reproducible, inexpensive test and demonstrated a high positive association between 6MWD <427 m and the VO2 max <11 ml O2/kg/min by the CPET [Lee et al. 2013; Sinclair et al. 2012].
The 6MWT is used for treatment monitoring and predicting the prognosis of various diseases. Moreover, it has become the most widely useful tool for submaximal exercise tolerance testing and more patients accepted compared with other tests (e.g. shuttle walking, 200 m fast walk and stair climbing) [Casillas et al. 2013; Lee et al. 2013; Sinclair et al. 2012; Morales-Blanhir et al. 2011; Guimarães et al. 2008; American Thoracic Society, 2002; Solway et al. 2001; Miyamoto et al. 2000; Knox et al. 1998; Cahalin et al. 1996; Wijkstra et al. 1994; Butland et al. 1982]. However, there are differences in normal value of 6MWD among countries depending on ethnicity, gender, age and body mass index (BMI); the average of 6MWD in healthy Thai subjects is 635.0 ± 75.0 m (range 489–994 m) [Casillas et al. 2013; Papathanasiou et al. 2013; Morales-Blanhir et al. 2011; Suwanachaiy et al. 2010]. Previous studies have shown that preoperative 6MWD less than 200–304 m was a predictor of a high mortality [Szekely et al. 1997; Holden et al. 1992] and was increased in some types of PPC after undergoing thoracic or major surgery [Awdeh et al. 2015].
In our present study, we performed preoperative 6MWT in 78 participants with clinically high risk of developing PPC after receiving elective thoracic or nonthoracic surgery under GA. The study showed elderly patients, those with ASA class >2, smoking history, low level of 6MWD and FEV1 % predicted but not the ratio of FEV1/FVC were the independent factors associated with PPC. The AUC, which quantifies the overall ability of the three parameters to discriminate between those individuals with PPC and those without PPC showed that 6MWD had a very good performance for PPC prediction, which was similar to that for FEV1 % predicted but significantly better than FVC % predicted. Therefore, the 6MWT is a good alternative choice for using as the PPE test in high risk patient groups and should be considered when spirometry testing is unavailable or there are contraindications to it. Furthermore, we found that preoperative 6MWD ⩽325 m could predict the high PPC risk with a sensitivity of 77% and specificity of 100%. This means that three-quarters of patients who develop PPC had a preoperative 6MWD ⩽325 m; therefore, a decision to postpone the surgery and/or various of preoperative risk reduction strategies to reduce PPC should be offered to these patients [Canet and Mazo, 2010; Rudra and Das, 2006; Smetana, 1999]. However, there was a very low PPC risk for those patients who had a preoperative 6MWD >325 m and thus patients scheduled for surgery would be continued.
The present study had a similar trend of 6MWD for PPC prediction as the study by Awdeh and colleagues [Awdeh et al. 2015], but with a different cutoff level that might be due to the different definitions of primary outcome of interest and different ethnic group. In contrast, Paisani and colleagues found no association between preoperative 6MWD and the PPC risk in patients who underwent UAS [Paisani et al. 2012]. There are a few possible explanations for these apparently opposite results. Firstly, our study recruited not only UAS, but also included participants undergoing thoracic surgery (who were likely to have some degree of preoperative pulmonary function impairment) and thus the 6MWT could be a more useful test for PPC prediction in this patient group. Secondly, the present study population was confined to the potentially high risk PPC patients with indication for PPE, and lastly, there were a few specific differences between the studies in the definitions and results of PPC. Therefore, directly comparison of the results of these two studies is not meaningful.
The strength of our study includes: (1) only clinically high risk PPC patients who needed PPE were evaluated (real-life practice); and (2) the performance of the 6MWT was compared with the current standard test for PPE (spirometry test) and the high sensitivity and specificity cutoff level of 6MWD for PPC prediction was also shown. However, our study has some limitations. Firstly, there is no comparison data between the 6MWT with other preoperative submaximal exercise tolerance tests. Secondly, there were no patients with contraindications to the 6MWT and no participants with baseline oxygen desaturation in the recruitment period; therefore, there are no data on the limitations of the 6MWT in our study. Thirdly, our study population was confined to Thai patients and lastly, there are no comparative data with 6MWT versus CPET due to the low availability of CPET in Thailand. Therefore, further studies are needed to define the suitable 6MWD cutoff level for other racial groups and to compare the predictive value between the 6MWT and CPET.
Conclusion
The preoperative 6MWT is a simple and safe test which has a high performance for PPC prediction comparable with that of spirometry in clinically high risk patients undergoing elective surgery under GA.
Footnotes
Acknowledgements
The authors would like to acknowledge The Royal College of Physician of Thailand (RCPT) for giving us a Clinical Research Award in 2014.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors
Conflict of interest statement
The authors declare no conflicts of interest in preparing this article.