
Abstract
Background:
Nonasthmatic eosinophilic bronchitis (NAEB) responds well to inhaled corticosteroids (ICS), while recurrence is common after discontinuing treatment. There are no data available to show whether treatment duration of ICS in patients with NAEB is related to recurrence. We aim to evaluate the effect of different duration of treatment with ICS on relapse of NAEB.
Methods:
A total of 101 patients with NAEB were recruited to the open label, randomized, parallel-group trial. Patients were randomized to receive 1-month, 2-month, or 4-month treatment with inhaled budesonide (200 μg, twice daily). Sputum induction, cough visual analogue scale (VAS), and cough symptom score (CSS) were conducted at baseline and after completion of treatment. The patients were followed up for 1 year after treatment. The primary outcome was the relapse rate of NAEB in 1 year.
Results:
ICS significantly decreased cough VAS, CSS, and sputum eosinophilia among these groups. There were no statistically significant between-group differences in cough VAS, CSS scores, and sputum eosinophil counts at the end of treatment, and no significant between-group differences in those changes from baseline to post-treatment. Significantly, more participants in the 1-month treatment group experienced a recurring episode of NAEB than those in the 3-month treatment group (41.9% versus 12.0%, p = 0.0137) at 1-year follow-up. The 2-month treatment group showed a lower tendency, with a relapse rate of 20.0% (p = 0.0644).
Conclusions:
Our results suggest that inhaled corticosteroids should be administrated for at least 2 months to reduce the relapse of NAEB.
Clinical trial registration:
The study was registered on ClinicalTrials.gov (NCT02002715).
The reviews of this paper are available via the supplemental material section.
Introduction
Nonasthmatic eosinophilic bronchitis (NAEB), characterized by irritable dry cough, sputum eosinophilia, being responsive to corticosteroids, and without the abnormalities of airway function that characterize asthma, was originally described by Gibson and colleagues, 1 and has subsequently been reported as one of the most common causes of chronic cough, accounting for about 7–33% of cases.2–4 Anti-inflammatory treatment with inhaled corticosteroids (ICS), or avoidance strategies, if the eosinophilic inflammation was caused by occupational exposures or inhaled allergen, have been the cardinal therapies for the treatment of NAEB. 5 After steroid treatment, cough improves, sputum eosinophil count decreases significantly or even returns to normal level, and no significant progressive decline is found in lung function despite the decrease in small airway function in some NAEB patients over time. 6 However, NAEB seems to be a continuing disease, and recurrence is common.7,8 Our previous study also showed that up to 59.6% patients with NAEB relapsed after 4-weeks of ICS treatment. 6 For asthma, with similar airway eosinophilic inflammation, long-term treatment with ICS is the cornerstone of successful treatment and prevention of exacerbation of the condition.9–11 We postulated that insufficient ICS treatment, in particular, short duration of treatment with ICS, may lead to relapse of NAEB. However, no data currently available show whether duration of ICS is related to relapse of NAEB. Hence, we conducted this open label, randomized, parallel group comparison trial to test whether duration of treatment with ICS could affect the relapse rate of NAEB.
Methods
Study design and subjects
The study was a trial of open label, randomized, parallel group comparison of 1-month, 2-month, and 4-month treatment with ICS in an outpatient population with NAEB.
We recruited adults with protracted cough (>3 weeks) attending a specialist cough clinic in the First Affiliated Hospital of Guangzhou Medical University (between March 2008 and May 2018). All patients had undergone investigations and treatment to determine causes of cough, as stated in ‘the Chinese national guidelines on diagnosis and management of cough’. 12 We included steroid-naïve patients with NAEB using the following criteria: prolonged or protracted cough lasting more than 3 weeks; no abnormality in chest radiograph; normal pulmonary ventilation function, and a lack of airway hyperresponsiveness; and sputum eosinophil count of more than 2.5%. We excluded patients with the following conditions: a history of upper respiratory tract infection within 4 weeks; previous administration of ACE inhibitors, pregabalin or gabapentin, or any treatment that might modulate cough; pregnant or lactating women; current or recent smokers (<6 months’ abstinence), or ex-smokers with more than 10 pack-years. Comorbidity with gastroesophageal reflux disease, upper airway cough syndrome, and other causes of cough were ruled out based on medical history, investigations, and treatment.
The study was approved by The Ethics Committee of The First Affiliated Hospital of Guangzhou Medical University. Informed written consent was obtained from each subject. The study was registered on ClinicalTrials.gov (NCT02002715).
Procedures
Subject screening included medical history, physical examination, vital signs, chest X-ray, routine blood test, spirometry, bronchial challenge test, and sputum induction test. After screening assessment, subjects were randomly assigned (1:1:1) to receive 1-month, 2-month or 4-month treatment with inhaled budesonide (200 μg, twice daily). A computer-generated randomization list of permuted mixed block sizes (varying between 3 and 9) was used for allocation of treatment duration. Sputum induction and cough severity assessment were conducted at baseline and at the end of therapy with ICS. Follow-up visits were conducted after 1 year and upon recurrence of cough. Cough severity assessment, sputum induction test, spirometry, and bronchial challenge test were performed at follow-up visit. Patients were given telephone interviews when they had no symptoms or were unable or unwilling to attend the site visit.
Cough severity was assessed with Cough Visual Analogue Scale (VAS) and Cough Symptom Score (CSS). Cough VAS is a 10 cm scale on which patients indicated the severity of cough, with higher score meaning more severe cough. CSS is a two-part questionnaire relating to cough symptoms during day and night, in which each part score ranges from 0 to 5; 0 meant no cough; 5 indicated distressing coughs most of the day or preventing any sleep. 13
Sputum was induced and processed as described by the Clinical Practice Guidelines for Diagnosis and Management of Cough. 14 Briefly, sputum was induced with 3% saline inhaled for 10 min via an ultrasonic nebulizer. If an insufficient amount of sputum was collected, the above step was repeated until a sufficient amount of sputum was obtained, or the total duration of nebulization reached 30 min. Sputum was mixed with four times its volume of 0.1% dithiothreitol, and filtered through a nylon gauze. The cell smear was stained with hematoxylin-eosin. A differential count was obtained by counting 400 nonsquamous cells, including eosinophils, neutrophils, macrophages, and lymphocytes.
Spirometry and bronchial provocation tests were conducted as recommended by the American Thoracic Society. 15 The forced vital capacity (FVC), forced expiratory volume in 1 s (FEV1), and FEV1/FVC were recorded. Airway hyperresponsiveness was defined as a 20% fall in FEV1 at a methacholine dose ⩽12.8 μmol.
Outcomes
The primary outcome was the relapse rate of NAEB in 1 year. Relapse of NAEB was defined as repeated episodes of cough with sputum eosinophilia (sputum eosinophil count ⩾ 2.5%), normal lung function, absence of airway hyperresponsiveness, and responsiveness to ICS. 6 Secondary outcomes were changes from baseline to end of treatment in cough severity and sputum eosinophil count, and the timing of relapse after treatment finished. Risk factors for relapse of NAEB were explored as well.
Statistical analysis
In this open label study, we used a modified intention-to-treat analysis. The intention-to-treat population consisted of patients who underwent randomization and received at least one dose of ICS treatment, except for those who were misdiagnosed or withdrew consent. We did not impute missing data. Statistical analysis was performed with SPSS version 16.0 software (SPSS Inc., Chicago, IL, USA) or GraphPad Prism version 8.02. Normally distributed data were expressed as mean± standard deviation (SD), and non-normally distributed data were described as median [interquartile range (IQR)]. Numeric variables were compared with one-way ANOVA or Kruskal–Wallis test, whereas categorical data was examined with Pearson Chi-square test, and these were followed by appropriate post hoc tests for multiple comparisons. Changes in cough VAS, CSS scores, and induced sputum eosinophil count were analyzed using paired Student’s t test or matched-pairs Wilcoxon signed-rank test. Logistic regression was applied to identify the risk factors associated with the relapse of NAEB.
With data for 30 patients in each group, we predicted this study to have about 80% power to achieve statistical significance at the 5% significance level (two-sided p test). This analysis assumed a 60% reduction in the relapse rate of NAEB with 4-month treatment compared with 1-month treatment, and the relapse rate in the 1-month treatment group was assumed to be 59%.
Results
Of the 106 patients diagnosed with NAEB that were recruited, 5 were excluded (3 caught an upper respiratory tract infection before randomization, and 2 had taken oral corticosteroids within a month). The remaining 101 patients were assigned randomly to 1-month (1-M group) (n = 33), 2-month (2-M group) (n = 35) or 4-month (4-M group) (n = 33) treatment with inhaled budesonide (200 µg, twice daily). Six subjects were lost to follow up and seven subjects withdrew from the study: three withdrew for personal reasons; one was immediately lost to follow-up without taking ICS treatment; three did not response to ICS and were finally diagnosed as cough due to obstructive sleep apnea, gastroesophageal reflux-related cough and chronic refractory cough, respectively, after further investigation and treatment. In the 4-month treatment group, three subjects took an actual duration of 2 months ICS. A total of 89 participants completed the trial (Figure 1).

Trial profile.
The baseline characteristics of patients are summarized in Table 1. The majority of the subjects were middle-aged and all patients in all three groups had normal spirometry. The demographic and physiologic parameters collected included gender, body mass index (BMI), cough duration, morbidity rate of allergic rhinitis, and cough severity, and were comparable in all three groups.
Baseline demographic and clinical characteristics.
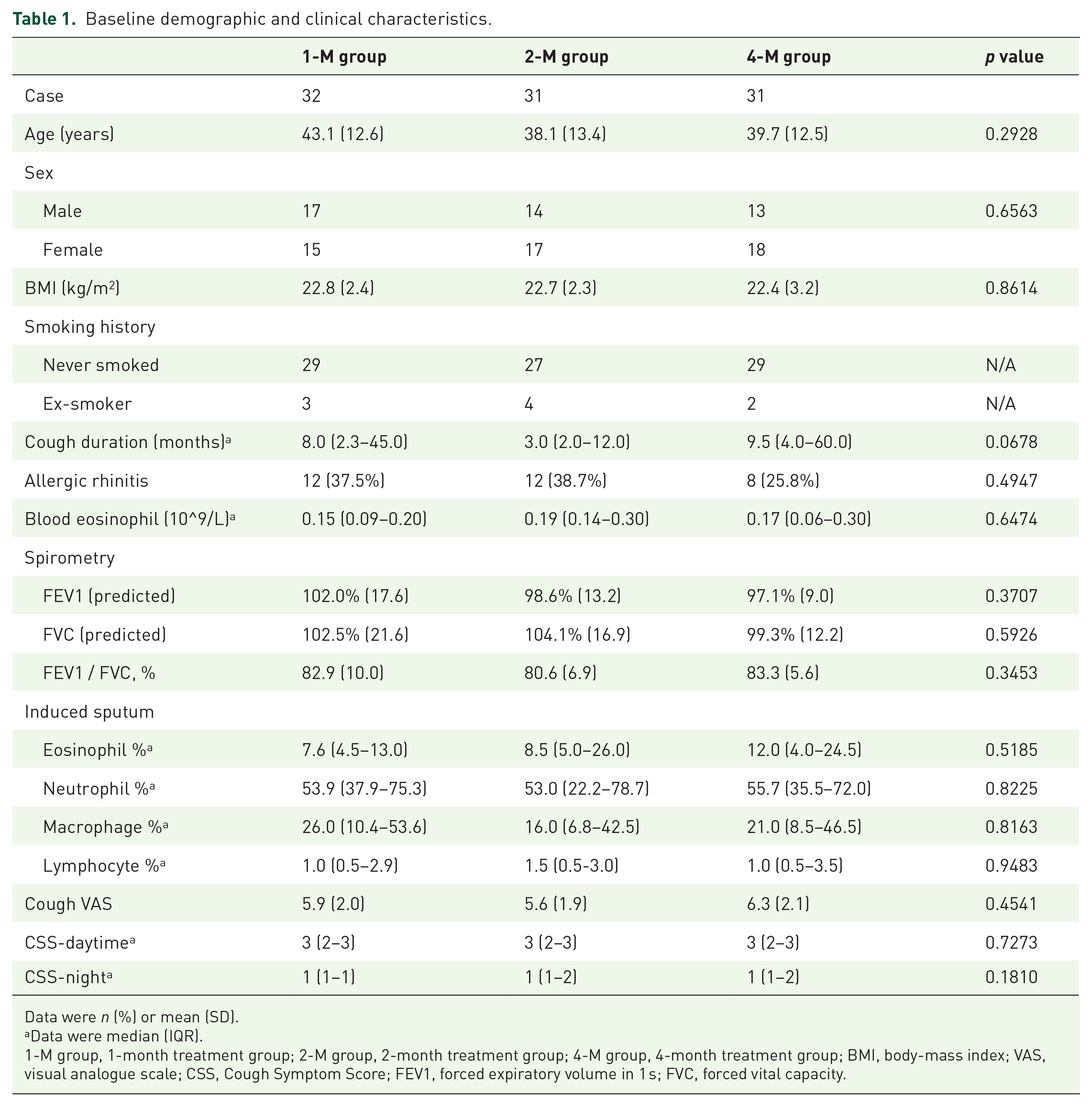
Data were n (%) or mean (SD).
Data were median (IQR).
1-M group, 1-month treatment group; 2-M group, 2-month treatment group; 4-M group, 4-month treatment group; BMI, body-mass index; VAS, visual analogue scale; CSS, Cough Symptom Score; FEV1, forced expiratory volume in 1 s; FVC, forced vital capacity.
The changes in cough severity after treatment with ICS are summarized in Table 2. Inhaled budesonide led to a great reduction in cough VAS and CSS at the end of treatment. There were no statistically significant between-group differences in cough VAS (p = 0.3310), CSS daytime (p = 0.7850), or CSS night (p = 0.4604) after treatment, and no statistically significant between-group differences in those changes from baseline to the end of treatment. After treatment with ICS, sputum eosinophil count was significantly decreased to 1.0% (0.0%–3.2%) in 1-M group, 1.5% (0.5–3.1%) in 2-M group, and 1.8% (0.5–4.0%) in 4-M group, respectively (Figure 2). There were no statistically significant between-group differences in sputum eosinophil count at the end of treatment (p = 0.4319), or in changes of sputum eosinophil count from baseline to the end of treatment (p = 0.6092).
Efficacy analysis for ICS in the treatment of NAEB between groups.

Data are median (IQR). Post refers to the end of therapy visit.
Data are mean (SD).
p value for between-group difference in changes from baseline to end of therapy visit.
ICS, inhaled corticosteroids; 1-M group, 1-month treatment group; 2-M group, 2-month treatment group; 4-M group, 4-month treatment group; NAEB nonasthmatic eosinophilic bronchitis.

Changes in sputum eosinophil count from baseline to the end of treatment visit.
Of 89 patients, 22 (24.7%) experienced recurrent episodes of NAEB within 1 year. Significantly more participants in the 1-M group experienced recurrent episodes of NAEB in the 1-year follow-up than did those in the 4-M group [13 (41.9%) of 31 versus 3 (10.7%) of 28; p = 0.0071]. The relapse rate of NAEB was 20.0% (6/30) in the 2-M group, and that was lower but not statistically significantly different than in the 1-month treatment group (p = 0.0644). There was no significant difference in the relapse rate of NAEB between the 2-M and 4-M groups (p = 0.5398) (Figure 3).

Relapse rate of NAEB in 1 year.
The median time of relapse was 2 (1–10.8) months in the 1-M group, 4 (2.5–7.8) months in the 2-M group, and 1 (1–2) month in the 4-M group, respectively, and there were no statistically significant between-group differences (p = 0.2497).
Sputum eosinophil count at the end of treatment in patients with relapse was significantly higher than those without relapse [3.3% (1.0–6.0%) versus 1.0% (0.0–2.6%), p = 0.0079] (Supplemental Table 1). Multiple logistic regression analysis indicated that increased sputum eosinophil count at the end of treatment was a risk factor of relapse (Supplemental Table 2).
Discussion
To the best of our knowledge, this is the first study to assess the effects of duration of treatment with ICS in patients with NAEB. Findings from this trial have shown that patients taking ICS treatment for 2 months or 4 months have less than half the recurrence rate compared with 1-month treatment, though there were no statistically significant between-group differences in therapeutic efficacies of cough severity or sputum eosinophil count. These results suggest that more than 2 months treatment with ICS might be necessary for NAEB.
NAEB is one of the common causes of chronic cough. Patient demography was similar to that of the whole chronic cough population, presenting as predominately female and aged,4,8,16 while there was equal sex distribution and presentation at a younger age in the Chinese population.3,17 The overall relapse rate in this trial was similar to the 21% reported by Park and colleagues, 8 but lower than that reported by Berry and colleagues, 7 and by our previous study. 6 Cigarette smoking could attenuate the response to ICS. 18 In this trial, the participants were cigarette nonsmokers without comorbidities such as gastroesophageal reflux disease or other causes of cough, which may explain why the participants responded well to low dose of ICS, and may explain why the relapse rate was relatively low. In addition, the follow-up period was just 1 year, which may also contribute to the low relapse rate in the study.
NAEB shares similar eosinophilic inflammation with asthmatics despite no airway hyperresponsiveness in NAEB. There were similar degrees of sputum, bronchoalveolar lavage fluid, biopsy eosinophils, T lymphocytes and mast cells, and a similar degree of basement membrane thickening in bronchial biopsy specimens in both conditions.5,11,19,20 In addition, NAEB also shows increased sputum concentrations of the inflammation mediators, cytokines such as IL-5, histamine, cysteinyl-leukotrienes and eosinophilic cationic protein as in asthma.2,21,22 In asthma, corticosteroids were able to decrease the production of pro-inflammatory cytokines, like T2 cytokines IL-4, 5, and 13 cysteinyl-leukotrienes; and to reduce the influx and survival of inflammatory cells, specifically eosinophils, lymphocytes, macrophages, and mast cells. 23 Long-term treatment with corticosteroids was essential to control symptoms, relieve inflammation, and prevent exacerbation in asthmatics. Previous studies have showed that 1-month treatment with ICS could significantly decrease cough severity and sensitivity, and reduce the sputum eosinophil count in patients with NAEB.24,25 In this trial, we found that a 1-month treatment with ICS could improve cough and decrease eosinophil count in sputum. Besides, efficacies for relieving cough and decreasing sputum eosinophil count with 1-month ICS treatment were comparable to those with 2- or 4-months ICS treatment. However, 1-month treatment was insufficient to prevent the relapse of NAEB. In this trial, we only assessed the airway inflammation by differential cells in induced sputum, without detecting changes of inflammation mediators in airway. Hence, we did not know whether an ‘endogenous trigger’ that played a key role in disease status had been eliminated or not during the 1 month treatment period. Longer treatment with ICS seem to be a better option for NAEB, as the relapse rates following 2- or 4-month treatment with ICS were decreased by over 50% compared with that following 1-month treatment.
The time to relapse in different treatment regimens did not show any statistically difference, but the data has to be interpreted cautiously due to the small number of relapsed cases, in particular with the 2- or 4-month treatment regimen. We used correlation, multiple linear regression, and Cox regression analysis to explore the relationship between timing to relapse and a set of exploratory variables, including sputum eosinophil at baseline, sputum eosinophil at the end of therapy, cough VAS, cough duration, and duration of treatment with ICS, while results did not show any statistically significant correlation (data not shown). However, sputum eosinophil at the end of treatment may help to phenotype the subgroup of patients that most benefit from longer ICS treatment since increased sputum eosinophil at the end of treatment was a risk factor of relapse. Just as asthmatics benefit from tailoring asthma interventions based on sputum eosinophil in reducing the frequency of asthma exacerbations, 26 tailoring interventions based on sputum eosinophil may be beneficial in patients with NAEB as well. However, this still needs further research.
There are limitations to our study. Since the duration of treatment was difficult to blind, this trial is an open-label design, which is a limitation of the study. Nevertheless, the investigators adjudicating outcomes were masked to the duration of ICS treatment. Another limitation of this study is that the sample size was small. The study seems underpowered to detect differences in relapse rate between the 1-month and 2-month treatment groups, although it was sufficient to detect a difference between the 1-month and 4-month treatment regimens. However, the reduction in relapse rate in the 2-month treatment group was impressive at over 50%, and the relapse rate in 2-month treatment group was significantly lower than in the 1-month treatment group [18.2% (6/33) versus 41.9% (12/31); p = 0.0377] when assigning the three subjects who had completed the follow-up period in the 4-month treatment group but had only taken 2 months treatment with ICS to the 2-month treatment regimen.
In conclusion, a low daily dose of ICS was sufficient to improve cough and suppress airway eosinophilia in patients with NAEB. Duration of treatment with ICS influenced the recurrence episodes of NAEB. Although a 1-month treatment results in significant improvement in cough and airway inflammation, proportion of relapse is higher compared with 2- and 4-month treatments. The longer duration of treatment with ICS (at least 2 months treatment) could lower the relapse rate.
Supplemental Material
Author_Response_v.1 – Supplemental material for Duration of treatment with inhaled corticosteroids in nonasthmatic eosinophilic bronchitis: a randomized open label trial
Supplemental material, Author_Response_v.1 for Duration of treatment with inhaled corticosteroids in nonasthmatic eosinophilic bronchitis: a randomized open label trial by Wenzhi Zhan, Jiaman Tang, Xiaomei Chen, Fang Yi, Lina Han, Baojuan Liu, Wei Luo, Qiaoli Chen and Kefang Lai in Therapeutic Advances in Respiratory Disease
Supplemental Material
Reviewer_1_v.1 – Supplemental material for Duration of treatment with inhaled corticosteroids in nonasthmatic eosinophilic bronchitis: a randomized open label trial
Supplemental material, Reviewer_1_v.1 for Duration of treatment with inhaled corticosteroids in nonasthmatic eosinophilic bronchitis: a randomized open label trial by Wenzhi Zhan, Jiaman Tang, Xiaomei Chen, Fang Yi, Lina Han, Baojuan Liu, Wei Luo, Qiaoli Chen and Kefang Lai in Therapeutic Advances in Respiratory Disease
Supplemental Material
Reviewer_2_v.1 – Supplemental material for Duration of treatment with inhaled corticosteroids in nonasthmatic eosinophilic bronchitis: a randomized open label trial
Supplemental material, Reviewer_2_v.1 for Duration of treatment with inhaled corticosteroids in nonasthmatic eosinophilic bronchitis: a randomized open label trial by Wenzhi Zhan, Jiaman Tang, Xiaomei Chen, Fang Yi, Lina Han, Baojuan Liu, Wei Luo, Qiaoli Chen and Kefang Lai in Therapeutic Advances in Respiratory Disease
Supplemental Material
Supplementary – Supplemental material for Duration of treatment with inhaled corticosteroids in nonasthmatic eosinophilic bronchitis: a randomized open label trial
Supplemental material, Supplementary for Duration of treatment with inhaled corticosteroids in nonasthmatic eosinophilic bronchitis: a randomized open label trial by Wenzhi Zhan, Jiaman Tang, Xiaomei Chen, Fang Yi, Lina Han, Baojuan Liu, Wei Luo, Qiaoli Chen and Kefang Lai in Therapeutic Advances in Respiratory Disease
Footnotes
Acknowledgements
The authors thank all the patients who participated in this study and Mei Jiang for assistance with data analysis.
Author contributions
All authors participated in manuscript writing and editing. Conception and design: Kefang Lai. Recruiting subjects and acquisition of data: Jiaman Tang, Xiaomei Chen, Fang Yi, Lina Han, Baojuan Liu. Performing induced sputum test and spirometry: Wei Luo, Qiaoli Chen. Analysis and interpretation: Wenzhi Zhan. Critical review and editing: Kefang Lai, Wenzhi Zhan. All authors read and approved the final manuscript.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and publication of this article: This study was supported by National Natural Science Foundation of China (81070019; 30670934); Guangzhou Municipal Science and Technology Key Project (2002Z2-E0091); Incubative Project for Innovation Team of GMU (2017-159); and Clinical Research Foundation of GMU (2017-160). The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Conflict of interest statement
The authors declare that they have no competing interests
Ethics approval and consent to participate
The study was approved by the research ethics committee of the First Affiliated Hospital of Guangzhou Medical University (No. 20134). All subjects gave written informed consents prior to participation.
Availability of data and materials
The datasets used and analyzed during the current study are available from the corresponding author on reasonable request.
Supplemental material
The reviews of this paper are available via the supplemental material section.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.