
Abstract
Bronchiectasis occurs as a result of a vicious circle consisting of an impaired mucociliary transport system, inflammation, and infection and repair of the airways. Damage to the mucociliary system prevents secretion elimination and facilitates bacterial growth and bronchial inflammation. To facilitate mucociliary clearance, current guidelines recommend the use of hypertonic saline (HS) solutions in patients with bronchiectasis not secondary to cystic fibrosis (CF), although the evidence of efficacy in this pathology is sparse. A high percentage of patients with CF and bronchiectasis tolerate HS solutions, but often patients report cough, dyspnoea, throat irritation, or salty taste after inhalation. These adverse effects negatively impact adherence to treatment, which sometimes must be discontinued. Some studies have shown that the addition of hyaluronic acid increases the tolerability of HS solutions, both in patients with CF and in bronchiectasis of other etiologies. We aimed to review the benefits and safety of HS solutions in patients with bronchiectasis.
The reviews of this paper are available via the supplemental material section.
Introduction
Mucociliary clearance is one of the defense mechanisms of the respiratory system. Its efficacy depends on a number of factors, including the efficacy of cough and ciliary activity, the rheological properties of the mucus, and the volume of the epithelial lining fluid.1,2 In patients with cystic fibrosis (CF), mutations in the gene encoding the cystic fibrosis transmembrane conductance regulator (CFTR) result in an altered protein, which leads to increased sodium absorption and decreased chlorine secretion in the respiratory tract. Consequently, the secretions produced are thick and dehydrated, which hinders mucociliary clearance and the elimination of bacteria.3–6 This can lead to chronic obstruction, infection, and inflammation that progressively damages the lung.
In non-CF bronchiectasis, the bronchial dilatations that characterize this disease make mucociliary clearance difficult, contributing to the vicious circle of infection and inflammation. Patients usually present with mucus hypersecretion that obstructs the airways, increases their resistance, promotes air entrapment, increases the residual volume, and decreases exercise tolerance. In addition, poorly ventilated areas of the lung produce an alteration of ventilation-perfusion, causing hypoxemia. 7 All these effects contribute to morbidity and mortality in bronchiectasis patients.
For this reason, one of the main objectives of the treatment of patients with airway obstruction due to respiratory secretions and chronic bronchial infection, along with antibiotic treatment and chronic treatment with macrolides, is to reduce the production of respiratory secretions and promote their clearance.
The efficacy and safety of hypertonic saline (HS) in CF is well established.7–9 HS inhalation twice a day in these patients reduces exacerbations and improves lung function and quality of life (QoL).8,10 For this reason, for more than a decade, Unites States (US) guidelines have been recommending the use of HS as a chronic therapy for the treatment of CF, 11 and a high percentage of CF patients use it routinely, not only in the US, but also in Europe.12,13 In addition, it has been shown that HS could be useful as an adjuvant to physiotherapy in the treatment of exacerbations. 10 However, the properties of the mucus in CF patients are different from those of patients with bronchiectasis or chronic bronchitis, which could, in part, explain the difference in the efficacy of the treatments and clinical evolution of these diseases. The available evidence of the efficacy of HS in other chronic respiratory diseases, such as bronchiectasis, ciliary dyskinesia, or chronic obstructive pulmonary disease (COPD) is much lower than in CF, and, in fact, has often been contradictory.14–18
Hypertonic saline
Recommendations of international guidelines
Recommendations for the use of HS in bronchiectasis, collected in international guidelines, have derived mostly from the effectiveness and safety demonstrated in CF.19–25 As shown in Table 1, European guidelines recommend the use of HS before physiotherapy with the aim of reducing sputum viscosity and facilitating expectoration and expulsion of mucus. 23 Some, like the Australian or Spanish guidelines, recommend HS, among other indications, in patients with frequent exacerbations.21,24 Both the Saudi and the British guidelines recommend isotonic saline and HS.22,25 Most guidelines recommend that patients use a bronchodilator before HS.
Recommendations on the use of HS in international guidelines on bronchiectasis.

FEV1, forced expiratory volume in 1 s; HA, hyaluronic acid; HS, hypertonic saline; PEF, peak expiratory flow; QoL, quality of life.
Mechanism of action
The inhalation of HS improves mucociliary clearance through mechanisms that are not fully understood, and which derive mainly from the experience in CF patients. One theory supporting this is that HS increases the osmotic gradient of water to the bronchial surface, rehydrating and increasing the volume of the epithelial lining fluid and decreasing the volume of the bronchial epithelial cells. 26 In this manner, HS would facilitate the transport and expulsion of the mucus.27,28
The pharmacodynamic efficacy of HS on mucociliary clearance in CF patients increases with its continuous use. 29 A single dose of HS may have a longer duration in CF than in healthy subjects. 30 Donaldson and colleagues suggested that the large volume of dehydrated secretions in the airways in CF patients can function as a reservoir to induce the transport of water by HS to the luminal compartment. 29 The creation of this water deposit in the mucus layer could prevent its rapid resorption of the epithelial surface. This may explain why the duration of the effects of HS, and perhaps its efficacy, may depend on the severity of the patient’s respiratory disease and the amount of mucus, with greater effects in patients with more severe lung involvement, and lower effects in those with a milder affectation.31,32
In addition to improvement of mucociliary clearance, some studies have shown that HS decreases mucus viscosity,33,34 stimulates cough,9,35 enhances the effectiveness of respiratory physiotherapy in both CF and bronchiectasis patients,14,15,27 accelerates mucociliary clearance via electrostatic interactions with mucins, 36 or inhibits epithelial sodium channels (ENaC). 31 Using human bronchial epithelial cells, Goralsi and colleagues speculated that sodium transport would modify the magnitude of HS-induced airway surface liquid volume expansion immediately after initiation of HS administration. As compared with HS alone, coadministration of an ENaC blocker produced a more rapid and sustained airway surface liquid response during nebulization. 31
The possible anti-inflammatory effects of HS have been investigated, with inconclusive results.31,37–39 Thus, in a 48-week study conducted in CF patients treated with HS, Elkins and colleagues found no differences in cytokine levels, proinflammatory cytokines (IL-6, IL-8, IL-10), and tumor necrosis factor alpha (TNFα) in the sputum of patients at the beginning and end of the study. 8 Also, a study by Aitken and colleagues did not find a decrease in IL-8 concentrations in sputum. 40 In this latter study, the concentration of IL-8 and neutrophils was measured at five different times in the first 20 min after inhalation of HS. Although the percentage of neutrophils decreased, the concentrations of IL-8 remained stable. 40 In contrast, Reeves and colleagues concluded that HS decreases the concentration of IL-8 in the sputum of patients with CF, favoring the reduction of inflammation in the lower airways. 41 Other research groups have described additional mechanisms that could explain the efficacy of HS, which include the activation of antimicrobial peptides or the inhibition of Pseudomonas aeruginosa growth due to an antimicrobial effect.42,43
Studies in chronic bronchitis suggest that alteration of the factors that control mucus concentration (such as mucin secretion and hydration of the extracellular matrix) can slow mucociliary clearance and contribute to pathogenesis and loss of lung function. 44 Other studies have shown that the inhalation of HS also accelerates mucociliary clearance in healthy subjects and in those with other chronic diseases,45,46 as well as enhancing the effectiveness of respiratory physiotherapy. 14 Along these lines, the results of an in vitro study by Goralski and colleagues showed that HS nebulization produced a rapid increase in the weight of the epithelial lining fluid that paralleled a decrease in the weight of the bronchial epithelium cells, 31 suggesting that water flows from the epithelial cells to the lining fluid by osmosis, as in CF. However, it is unknown if this stimulation of mucus transport is effective in reducing bronchial obstruction and exacerbations in patients without CF.
Although the mechanism of HS in bronchiectasis patients is not well understood, in these patients the sodium and chloride concentrations are below the optimum for mucociliary transport, as suggested by Wills. 33 Retained mucus favors infection, which ultimately causes the vicious cycle of events leading to chronic lung inflammation. HS could possibly increase the salinity of the retained secretions, particularly the gel surface, where improved effectiveness of interactions with cilia could result in increased mucociliary clearance. 33
Other facets of HS: concentration and volume
The optimal salt concentration of HS has not been clearly established. Although the effect appears to be dose-dependent (as higher salt concentrations increase the amount of expectorated sputum), adverse events also increase. A salt concentration of 12% is at the higher limit of patient tolerability, 27 but the most commonly used concentrations are 6% 16 or 7%.8,15,29
The volume of HS that is usually used ranges from 4 ml to 5 ml. 8,15,16,29 In most studies, HS is used twice a day,8,16 although in other works HS is nebulized once a day,14,15 or four times a day. 29 Regarding the nebulization system, the most commonly used system is the jet type.8,47
Clinical studies of HS in bronchiectasis
Study design
Only three randomized clinical trials have studied the use of HS in bronchiectasis, with a total of less than 100 patients (Table 2). They present marked differences in design, patient inclusion and exclusion criteria, severity of respiratory disease, posology of HS, and nebulizers used.14–16 The quality of evidence obtained in patients with bronchiectasis has been rated as moderate by the Cochrane Collaboration in 2014. 48 Generally, the introduction of various treatment-related variables in these studies, such as physiotherapy, 14 or the use of bronchodilators make interpretation of the efficacy of HS difficult.14–16
Studies of use of HS in patients with bronchiectasis.

ABPA, allergic bronchopulmonary aspergillosis; ACBT, active cycle of breathing techniques; CF, cystic fibrosis; FEV1, forced expiratory volume in 1 s; FVC, forced vital capacity; HRCT, high resolution computed tomography; HS, hypertonic saline; IS, isotonic saline; LCQ: Leicester cough questionnaire; LRTI-VAS, lower respiratory tract infections - visual analogue scale; QoL-B: quality of life for bronchiectasis; SGRQ, St George’s respiratory questionnaire; TNS, tobramycin nebulizer solution.
In a single-center, randomized, double-blind, crossover study, Kellet and colleagues compared four treatment regimes in 24 bronchiectasis patients for 4 weeks separated by one washout week. 14 Treatment regimens included active cycles of breathing techniques (ACBT) alone, nebulized terbutaline followed by ACBT, nebulized terbutaline followed by nebulization of one dose of 0.9% isotonic saline (IS) and then ACBT, and nebulized terbutaline followed by nebulization of one dose of the HS and then ACBT. The patients received only one type of treatment per week during the 4 weeks of the study in order to complete the four treatment schemes. The study focused on the results of a single dose of saline solutions. Patients were included in the study if they had difficulty in expectorating viscous and sticky sputum, and if they had required at least one cycle of antibiotics in the previous 6 months. Patients with a previous history of ‘thoracic tightness,’ wheezing or dyspnoea, or a drop in forced expiratory volume in 1 s (FEV1) of more than 10% after inhalation of HS were excluded from the study. No patients were excluded due to decreased lung function after inhalation of HS. 14
A second, single-center, randomized, single-blind, crossover study from the same research group analyzed 30 patients over a period of 8 months. 15 Of these patients, 28 met the inclusion and exclusion criteria and completed the study, which compared a treatment daily regimen of 4 ml of IS with 4 ml of 7% HS. After 1 month of screening, patients were randomized to receive 7% HS or IS for 3 months. After a 1-month washout period, patients were crossed over to receive another treatment cycle (HS or IS) for another 3 months, ending the study with a further 1 month of follow up without treatment. The inclusion criteria stated that the decrease in FEV1 after HS inhalation in the screening period should be > 10%; exclusion criteria included any serious medical condition that discouraged the use of HS, or a history of bronchial hyperreactivity. Two patients had a decrease in FEV1 of at least 10% after inhalation of HS in the screening period, so they were excluded from the trial. 15
In a single-center, randomized, double-blind, parallel group study of 12 months duration and 48 patients, Nicolson and colleagues compared treatment of 5 ml twice-daily IS versus 6% HS. 16 Each treatment arm had 20 patients, and the inclusion criteria stated that patients were able to expectorate daily, and that they had had at least two exacerbations per year that required antibiotics during the previous 2 years. Exclusion criteria included a decrease in FEV1 ⩾ 15% of predicted value after inhalation of HS, and having a FEV1 of <1 L. Of the 48 patients screened, 8 were excluded before randomization: 1 due to a decrease in FEV1 ⩾ 15% of predicted value after HS inhalation, 3 due to FEV1 < 1 L, and 4 due to refusing to enter the study. 16
In a single-center, randomized, controlled, double-blind, crossover study, Paff and colleagues compared regimens of 5 ml twice-daily IS versus 7% HS in patients with ciliary dyskinesia over 28 weeks. 17 Of the 86 patients screened, 22 met the criteria to participate in the study. Patients were randomized to receive 7% HS or IS for 3 months and, after a washout period of 4 weeks, were crossed to receive another cycle of treatment (HS or IS) for another 3 months. Inclusion criteria included a postbronchodilation FEV1 ⩾ 40% of predicted value; exclusion criteria included a decrease in FEV1 ⩾ 15% of predicted value over the prebronchodilator value after 15 min of inhalation of HS with quinine, or decrease in arterial oxygen saturation <90% after inhalation. 17
Lung function
No significant differences in FEV1 (% of predicted values) and FVC (% of predicted values) between IS and HS were found in the initial work of Kellett and colleagues. 14 Patients inhaled the solutions only once in each phase of the treatment so it was uncertain if any differences could be detected. 14 In a study published in 2011, these authors found clinically and statistically significant differences in favor of HS in the FEV1 and FVC percentages with respect to baseline in the two treatment phases (FEV1 improved 15.1 with HS versus 1.8 with IS). However, they did not find these differences in absolute FEV1. 15 In contrast, Nicolson and colleagues found no significant differences in absolute FEV1 and absolute FVC between HS and IS after 3, 6, or 12 months. Also, there were no differences with respect to baseline in any group at 12 months. 16 Paff and colleagues did not find differences in FEV1 or FVC between the groups. 17 The differences in the spirometry parameters between the groups could be explained because the patients in the Kellett study [baseline FEV1, mean % predicted (SD) = 66.4 (26.1)] had worse pulmonary function than patients in the studies of Nicolson and colleagues [baseline FEV1, mean % predicted (SD) = 80.4 (21.1) for the group treated with IS and 84.8 (20.5) for the group treated with HS], or Paff and colleagues [baseline FEV1, median % predicted (IQR) = 75.5 (58.8–94.5)] studies, and, in these patients, it is more difficult to observe improvements.
Quality of life
The differences in QoL between groups treated with IS and HS were analysed by two studies using the St. George Respiratory Questionnaire (SGRQ).15,16 In addition, the study by Nicolson and colleagues also used the Leicester Cough Questionnaire (LCQ), with incongruent results. 16
Using the SGRQ, Kellett and colleagues reported a significant benefit of HS over IS in its overall score, and in the symptoms and impact domains of the disease, but not in the activity domain. 15 Nicolson and colleagues found no differences between the HS and IS groups in the SGRQ in the domains of activity, impact, and symptoms at 3, 6, and 12 months of the study, but did not report data regarding the total value of the SGRQ. In the same study, no significant differences were found between both saline solutions in the physical or social domain of the LCQ at 3, 6, and 12 months. In the psychological domain at 6 and 12 months there were no differences, although there was a slight, but significant, difference, at 3 months in favor of HS. No data were reported regarding the total score of the LCQ. However, QoL improved significantly with respect to baseline with both saline solutions in all the SGRQ and LCQ domains at 3, 6, and 12 months. 16
The study by Paff and colleagues did not find significant differences in the median of the total SGRQ score between the HS and IS groups. In the Bronchiectasis Quality of Life Questionnaire (QoL-B), the study found clinically and statistically significant differences in favor of HS in the health perception dimension. In the dimensions of respiratory symptoms and vitality, the differences were also clinically meaningful in favor of HS, but not statistically significant. In contrast, changes in role limitation were statistically significant, but did not reach the minimum clinically important difference. Patients presented a slight, but significant, improvement in the perception of pain intensity, as measured by the modified visual analogue scale of lower respiratory tract infections (LRTI-VAS) while treated with HS versus IS. 17
There are several explanations for the differences in QoL among the three studies, such as the different methodology and population studied (bronchiectasis in the studies by Kellett and colleagues, and Nicolson and colleagues, ciliary dyskinesia in Paff’s study, or different severity of patients with respect to lung function and exacerbations), the small size of the patient populations studied, or the short duration of the trials. In addition, the QoL questionnaires used in the study of patients with ciliary dyskinesia may not be sensitive enough to assess improvements in the QoL of these patients, who also tend to have upper airway symptoms that would not necessarily improve with the HS used by aerosolized route with a buccal interface. And, finally, it is possible that HS was useful in some types of patients with bronchiectasis but not in patients with ciliary dyskinesia. 49
Exacerbations and use of antibiotics
Kellett and colleagues showed a significant difference in favor of HS over IS in reducing the frequency of exacerbations (2.14 exacerbations/year in the HS group compared with 4.85 in the IS group). There was also a reduction in the use of antibiotics in favor of the group treated with HS: 2.4 cycles per year versus 5.4 cycles of antibiotics per year in the IS group. 15
On the contrary, Nicolson and colleagues did not find differences between both groups in the frequency of annual exacerbations, exacerbations that required antibiotics, number of days with exacerbation, or number of days with exacerbation that required antibiotics. The median number of exacerbations requiring antibiotics was 1 for the HS group and 0.5 for the IS group. However, in both groups the frequency of exacerbations with respect to the year prior to the study was significantly reduced. 15
The differences between the studies of Nicolson and colleagues and Kellett and colleagues regarding exacerbations and QoL could be explained by several factors. The data obtained by Nicolson and colleagues regarding the exacerbations that the patients had the previous year were collected retrospectively, which could entail some degree of error. In addition, it is possible that the very large decrease in the frequency of exacerbations in the year of the study with respect to the previous year could be explained, at least in part, by the positive implications in adherence to treatment that any study entails. Finally, in the study by Kellett and colleagues, unlike that of Nicolson and colleagues, patients were not selected according to the number of exacerbations.
In the study by Paff and colleagues, no differences were found regarding the number of exacerbations in the two phases of treatment with HS. 17
Hospital admissions
The only work that studied hospital admissions was that of Nicolson and colleagues, who showed that there were no significant differences between the group treated with HS and the group treated with IS with respect to the number of hospital admissions and days of hospital stay. Four of the participants in the study (10%) had to be hospitalized, one in the group treated with HS for 68 days, and three in the group treated with IS for 3, 5, and 61 days, respectively. 16
Cough and expectoration
Both solutions, added to respiratory physiotherapy, were better than physiotherapy alone to facilitate expectoration,14,15 reduce sputum viscosity, and increase the amount of expectorated sputum. 14 However, there were no differences between groups with respect to the frequency of cough at 3, 6, and 12 months. 16
Microbiology
This aspect was contemplated only in the work of Nicolson and colleagues. The percentage of patients with potentially pathogenic microorganisms in the sputum samples decreased from 55% and 60% at the beginning of the study in the HS and IS groups, respectively, to 15% at the end of the study in both groups. This decrease was statistically significant with respect to the baseline situation, although there were no significant differences between the two. 16
Inflammatory markers
The study by Paff and colleagues analyzed inflammatory markers but did not observe any change after the treatment with HS. 17
Adverse events
In most of the studies, patients with suspected or confirmation of nontolerance to HS were excluded,15,16 so the number of adverse events caused by HS would have to be lower than expected in the general population of patients with bronchiectasis. There were no deaths in any of the trials.
In the study by Kellett and colleagues, no patients were excluded for initial intolerance to HS or significant reduction in FEV1 following HS inhalation. In the 2011 study, 2 out of 32 patients were excluded for initial intolerance to HS. No adverse events in either of the two trials were reported, and no patient had to leave the study as a consequence of the treatment.14,15 In the study by Nicolson and colleagues, 1 patient out of 48 in the initial screening was excluded because for significant reduction in FEV1 following HS inhalation. There were three adverse effects in the HS group. One patient had ‘tightness in the chest’ during the inhalation that resolved with treatment of the underlying exacerbation; another had an episode of hypertension that resolved spontaneously. Both cases were considered unrelated to the treatment and continued the study. The third patient had an episode of atrial fibrillation, and treatment with HS was discontinued. There were no adverse events in the IS group. The differences in adverse events between the two groups were not significant. 16
In the study by Paff and colleagues, three patients left the study: two from the HS group due to bronchoconstriction and intolerance to salbutamol, and one on treatment with IS for nausea. 17
HS and hyaluronic acid
Hyaluronic acid
Hyaluronic acid (HA) is a glycosaminoglycan with an important role in the regulation of the fluid balance in the interstitial space through its capacity to imbibe water, as has been observed in the lungs of people and animals, facilitating ventilation and gas exchange. 50
Hyaluronan, a ubiquitous naturally occurring glycosaminoglycan, is a major component of the extracellular matrix. HA participates in many biological processes such as homeostasis, angiogenesis, and cell migration and proliferation. Some studies suggest that HA and its degradation products can play an important role in the pathobiology of the respiratory tract. 50 HA could also have a protective effect against harmful agents in a large number of respiratory diseases, such as asthma, 51 CF, or COPD, 52 modulating the secretion of neutrophilic elastase and attenuating bronchial hyperreactivity.53,54 According to some authors, HA could also reduce the number of exacerbations in patients with chronic bronchitis, 55 possibly improving the cellular defenses of the organism. The role of HA in attenuating bronchial hyperreactivity in asthma is controversial.56,57 Although it has been claimed that HA can prevent the development of biofilm associated with chronic infection,58,59 its effects on this issue and on inflammation are not clear at present.60,61
Studies of the use of HA in bronchiectasis
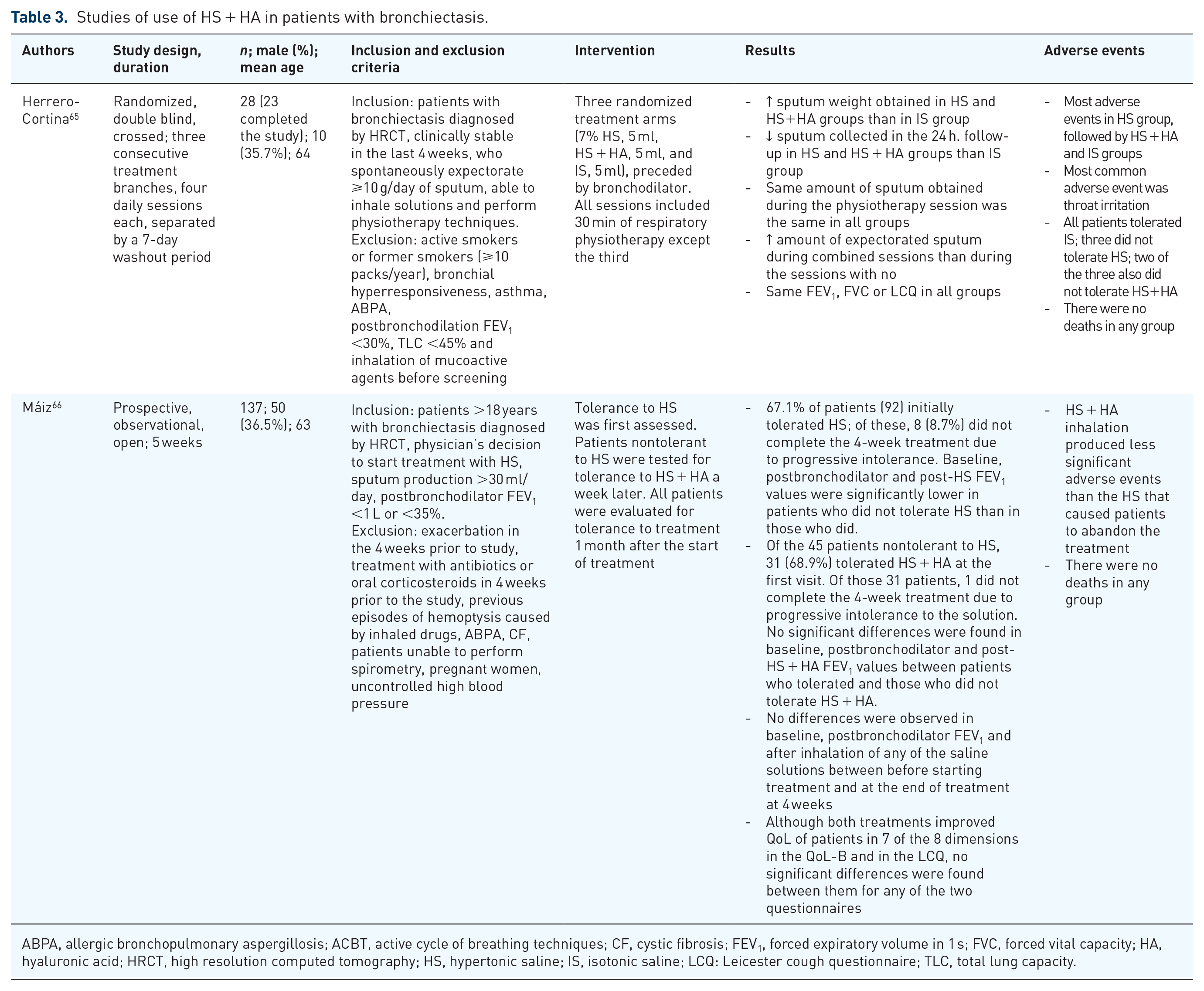
The addition of HA to HS has been studied mainly in patients with CF with the aim of improving tolerability and decreasing bronchial hyperreactivity and salty flavor.62–64 Recently, two trials with very different design investigating the tolerance of HS+HA in patients with bronchiectasis were published (Table 3).65,66
Studies of use of HS + HA in patients with bronchiectasis.
ABPA, allergic bronchopulmonary aspergillosis; ACBT, active cycle of breathing techniques; CF, cystic fibrosis; FEV1, forced expiratory volume in 1 s; FVC, forced vital capacity; HA, hyaluronic acid; HRCT, high resolution computed tomography; HS, hypertonic saline; IS, isotonic saline; LCQ: Leicester cough questionnaire; TLC, total lung capacity.
Herrero-Cortina and colleagues carried out a single-center, randomized, double-blind, cross-over study with three consecutive treatment arms of four daily sessions each, and separated by 7-day washout periods. 65 All sessions except the third (control period), included 30 min of physiotherapy. They compared 5 ml of three saline solutions (7% HS, 7% HS + 0.1% HA, and IS) in 28 bronchiectasis patients and chronic expectoration. One of the inclusion criteria was that patients should expectorate sputum amounts greater than 10 g/day. Patients with diagnoses of bronchial hyperreactivity, asthma, a postbronchodilator FEV1 <30% or a total pulmonary capacity <45% were excluded from the study. 65
The HS and the HS + HA groups generated a similar sputum expectoration during the sessions, and more than in the IS group. Sputum collected during the 24-h follow up after the end of the sessions with saline solutions tended to be lower for the HS and HS + HA groups than for the IS group. This suggested that hypertonic solutions could achieve greater expectoration of sputum during treatment, reducing the need to expectorate during the rest of the day, as has been observed in studies with respiratory physiotherapy in bronchiectasis patients. 67 The amount of sputum obtained during physiotherapy was the same, regardless of the type of saline solution previously used. They also observed that the amount of expectorated sputum was greater during the combined sessions (saline solutions followed by physiotherapy) than during the session in which physiotherapy was not performed, without differences with respect to the saline solution used. No differences were found in FEV1, FVC, or LCQ between any of the treatment arms. 68
Most of the serious adverse events were reported in the HS group. Cough and throat irritation were the most common. Three patients presented a mild oxygen desaturation during inhalation, recovering spontaneously after inhalation. While all patients tolerated IS, three patients did not tolerate HS. Two of the three also did not tolerate HS + HA. These three patients were older (⩾75 years) and with worse pulmonary function (FEV1 ⩽40% of the predicted) than the average patients in the study.
Máiz and colleagues carried out a multicenter, prospective, observational, open study, in 137 bronchiectasis patients with chronic expectoration, to evaluate tolerance to HS + HA in patients who were intolerant to HS. Inclusion criteria included daily sputum production >30 ml. Patients with postbronchodilator FEV1 <1 L or <35% were excluded from the study. Tolerance to both solutions was assessed by a questionnaire, spirometry (decrease in FEV1 ⩾15% after inhalation of HS compared with postbronchodilation) and clinical evaluation. The tolerance of patients to HS was assessed first and nontolerant patients were then tested with HS + HA a week later. Tolerability was also evaluated 1 month after the start of either treatment in all patients. QoL, adherence to treatment, and adverse events were also evaluated. 66
Of the 137 patients, 92 (67.1%) initially tolerated treatment with HS. Of those 92 patients who tolerated the treatment at the baseline visit, 8 (8.7%) could not complete the 4-week treatment due to progressive intolerance. The most frequently reported adverse events were cough, pharyngeal irritation, and salty taste. Baseline, postbronchodilator and post-HS FEV1 values were significantly lower in those who were intolerant to HS compared with those who tolerated it. This suggests that FEV1 could be a useful indicator of patients who are less tolerant to HS. This observation would be in accordance with published data on CF and bronchiectasis patients.63,65
Of the 45 patients intolerant to HS, 31 (68.9%) patients tolerated HS + HA at the first visit. Of those 31 patients, 1 did not complete the 4-week treatment due to progressive intolerance to the solution. No significant differences were found in baseline, postbronchodilator and post-HS + HA FEV1 values between patients who tolerated and those who did not tolerate HS + HA. Inhalation of HS + HA generated fewer significant adverse events than those in the HS group that caused patients to abandon treatment.
Adherence to treatment was good in both treatment groups, with no significant differences between them. No significant differences were observed in baseline, postbronchodilator FEV1 and after inhalation of any of the saline solutions between before starting treatment and at the end of treatment after 4 weeks. QoL was evaluated by the validated Spanish version of QoL-B and the LCQ, at the beginning and at the end of the study. 69 Although both treatments improved QoL of the patients in seven of the eight dimensions in the QoL-B and in the LCQ, no significant differences were found between them for any of the two questionnaires. Although few of patients in the earlier studies using HS had to leave the studies because of intolerance,14–16 in the study by Maiz and colleagues, more than one-third of the patients were intolerant to HS in the 1st week of the study. 66 Although more studies are needed to know the factors determining tolerance in these patients, it is likely that older age and worse lung function contribute to decreased tolerability.65,66
Conclusion
Inhalation of HS twice a day is effective and safe in patients with CF. 8 The data obtained from clinical trials suggest that in these patients HS reduces exacerbations and improves QoL. 10 International CF guidelines recommend the use of HS before physiotherapy with the aim of reducing sputum viscosity and facilitating expectoration and expulsion of mucus. 11
In bronchiectasis there is less evidence for the use of HS or HS + HA than in CF. However, some studies suggest that HS can facilitate expectoration,15,16,65 decrease sputum viscosity,15,16 increase lung function, 16 and decrease the frequency of exacerbations. 16 Due to this, and the excellent clinical response to HS in clinical practice, most guidelines on bronchiectasis recommend its use.20,21,24
There is uncertainty concerning the proportion of patients who tolerate HS and the causes of intolerance; however, age and pulmonary function seem to play an important role. Tolerability is more likely develop in elderly with poor pulmonary function. 66
HA improves tolerability to HS by decreasing salty taste, cough, and dyspnea, in patients with both CF and bronchiectasis.62–64,65,66 In patients who do not tolerate HS, or in patients in serious condition, the formulation with added HA is an alternative to be evaluated.
Supplemental Material
Author_Response_1_3 – Supplemental material for Nebulized hypertonic saline in noncystic fibrosis bronchiectasis: a comprehensive review
Supplemental material, Author_Response_1_3 for Nebulized hypertonic saline in noncystic fibrosis bronchiectasis: a comprehensive review by Luis Máiz Carro and Miguel A. Martínez-García in Therapeutic Advances in Respiratory Disease
Supplemental Material
Reviewer_1_v.1_3 – Supplemental material for Nebulized hypertonic saline in noncystic fibrosis bronchiectasis: a comprehensive review
Supplemental material, Reviewer_1_v.1_3 for Nebulized hypertonic saline in noncystic fibrosis bronchiectasis: a comprehensive review by Luis Máiz Carro and Miguel A. Martínez-García in Therapeutic Advances in Respiratory Disease
Footnotes
Acknowledgements
The authors thank Francisco López de Saro (Trialance SCCL) for editorial support.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and publication of this article: this review was sponsored by Chiesi España SAU.
Conflict of interest statement
Luis Máiz reports participation in teaching and research activities supported by Chiesi SAU, Grifols SA, TEVA Pharma SL and Zambon SAU. Miguel A. Martínez-García reports participation in teaching and research activities supported by Chiesi SAU, Grifols SA, TEVA Pharma SL and Zambon SAU.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.