
Abstract
Background:
Hypertonic saline inhalation has been shown to be effective in patients with cystic fibrosis and lung disease. However, adverse events including marked airway narrowing are reported and a bronchodilator must be given before the administration of the product.
Methods:
We carried out a prospective, randomized, double-blind, parallel-group, controlled study of a hypertonic saline solution containing hyaluronic acid (Hyaneb) versus standard hypertonic saline therapy to assess whether the presence of hyaluronic acid would improve the tolerability of hypertonic saline.
Results and conclusions:
The results showed that nebulized Hyaneb was more effective in reducing the need for β2 bronchodilators and caused a significant reduction in the incidence of adverse effects compared with nebulized hypertonic saline solution alone. Its safety profile indicates that Hyaneb can be used for the treatment of lung disease in cystic fibrosis.
Introduction
Cystic fibrosis (CF), or mucoviscidosis, is a complicated genetic disease that causes the body to produce thick, viscous, mucous secretions especially in the lungs, liver, and intestines [Davis et al. 1996]. The respiratory tract is the organ system most affected and lung disease causes 95% of the mortality and morbidity in patients with CF [Voynow et al. 2008].
The bronchioles and bronchi, which normally produce a thin, clear mucus that traps foreign particles including bacteria and viruses, produce a thickened mucus in patients with CF. The movement of the ciliary projections on the surface of these passageways, which normally sweep the mucus along, out of the lungs and up the trachea to the back of the throat, where it may be swallowed or coughed up, are slowed down due to the thickened mucus. This increases irritation and inflammation of lung tissue. As normal mucociliary movement is one of the body’s main defences against lung infection, the impaired movement in patients with CF leads to lung disease.
The most important clinical finding is a difficulty in breathing with frequent lung and sinus infections. In CF lung disease, the isotonic volume-depletion hypothesis [Mall et al. 2004] proposes that defective chloride secretion and excessive sodium absorption reduce the volume of airway surface liquid, causing mucus dehydration, decreased mucus transport and mucus plugging of the airways, which are the hallmarks of the early disease [Donaldson and Boucher, 2007; Boucher, 2007]. Failure of effective mucus clearance initiates and exacerbates CF lung disease resulting in an inability to effectively prevent or eradicate bacterial infection, typically dominated by Pseudomonas aeruginosa [Matsui et al. 1998], and subsequent damage of the pulmonary tissue.
Based on the above hypothesis, therapies that increase the volume of airway surface liquid, and hence mucus clearance, should improve lung disease in patients with CF. Hypertonic saline (HS; NaCl 7%) inhalation has been proposed as a therapy to increase the hydration of airway surface liquid in patients with CF, thereby improving mucociliary clearance [Turino and Cantor, 2003]. Short-term administration of 7% HS is reported to improve the rheological properties and transportability of sputum, the hydration of the airway surface, mucociliary clearance and pulmonary function and to reduce the number of exacerbations and improve the quality of life in patients with CF.
In a 48-week, randomized, long-term, double-blind study, the HS group showed an improvement in lung function as early as 4 weeks after randomization with a plateau at 12 weeks which persisted for the rest of the study, maintaining a difference with the control group [Elkins et al. 2006]. The trial also demonstrated other important benefits of using HS as a routine therapy: the number and duration of pulmonary exacerbations were significantly lower and the percentage of patients remaining exacerbation free was significantly higher with HS. Other significant benefits were the reduced use of antibiotics for exacerbations and improved attendance at school, work and all usual activities [Elkins et al. 2006]. However, marked airway narrowing is reported in some patients with CF after inhalation of HS and this should be considered whenever HS nebulization is used [Ratjen, 2006]. In such cases a bronchodilator must be given before the administration of HS to prevent airway narrowing. However, even when a bronchodilator is used as premedication, some patients with CF describe airway narrowing and other adverse reactions such as cough, chest tightness and pharyngitis with HS. The saltiness of the HS solution is distasteful to some patients. All these adverse events could reduce treatment compliance.
A unique property of hyaluronic acid (HA) is its water-retaining properties and the water content of a tissue depends on the amount of HA it contains [Turino and Cantor, 2003]. Inhaled HA appears to prevent bronchoconstriction and protect against inflammatory mediator-induced bronchoconstriction [Scuri and Abraham, 2003; Petrigni and Allegra, 2006]. It has also been shown to mitigate the actions of human neutrophil elastase and human macrophage metalloelastase in animal models of pulmonary emphysema [Turino and Cantor, 2003; Scuri and Abraham, 2003; Petrigni and Allegra, 2006]. Patients with emphysema have been shown to have significant reductions in HA [Schmid et al. 1982].
Hence, to reduce the adverse events and to avoid or minimize poor compliance with HS therapy, a new formulation containing 7% NaCl and 0.1% HA (Hyaneb, Eupharma s.r.l., Bologna, Italy) was recently proposed. The above-mentioned properties of HA support its use in lung disease. It is postulated that the hydration properties of inhaled HA would increase the volume of airway surface liquid resulting in mucous hydration, increased mucous transport and less mucous plugging of the airways. In addition, it is postulated that the presence of HA would improve the pleasantness and the tolerability of nebulized HS [Buonpensiero et al. 2010].
The main objectives of our study were to assess the tolerability of the study products and their efficacy on bronchospasm, as measured by the number of β2 agonists used and the measurement of forced expiratory volume in 1 s (FEV1) before and after inhalation of each product. The secondary objectives included an assessment of the tolerability of the two products on the airways (e.g. incidence of coughing, burning sensation in the throat, salty taste, and thoracic oppression) and an assessment of the efficacy of the treatments on pulmonary function.
Study design
This was a single-centre, prospective, randomized, double-blind, parallel-group, controlled study of a new HS formulation containing NaCl 7% and 0.1% HA versus standard HS containing NaCl 7%. The study was approved by the local regulatory authority and ethics committee and was conducted in accordance with the Declaration of Helsinki and its amendments. Written informed consent was obtained from patients, parents or legal representatives before enrolling patients into the study. The study was carried out at the Regional Reference Centre for Cystic Fibrosis in Palermo, Italy.
The inclusion criteria were male and female patients aged at least 10 years, diagnosed with CF, with FEV1 at least 40% of predicted value, undergoing stable antibiotic, mucolytic or anti-inflammatory treatment in the 3 months prior to study inclusion and having provided informed consent.
Patients were excluded from the study if they presented any of the following: Burkholderia cepacia infection; used HS therapy in the 15 days preceding enrolment; an exacerbation of infection in the 15 days preceding inclusion and which required antibiotic therapy; changes in chronic therapy (antibiotic, DNase, anti-inflammatory drugs) in the 28 days preceding enrolment.
Treatment was one bronchial inhalation of the assigned product twice a day for a period of 28 days.
Blinding
The study participants, investigators, study monitors and study personnel were blind to the treatment assignment of the patients. The two test products were packed in identical containers. However, the investigator had access to a sealed envelope containing the randomization code of patients which was to be opened only in the case of a medical emergency.
Data entry and data analysis were also performed in a blind manner, that is, before the codes were broken.
Concomitant treatments
Patients were allowed to continue their usual treatment for lung disease or use treatments for concomitant diseases, including inhaled antibiotic treatment for lower airway treatment or treatment with mucolytics (DNase) as long as they were under such treatment at study inclusion. However, treatment with systemic antibiotics, mucoactive products or corticosteroids was not permitted after the start of the study and throughout the study if the patient was not already being treated with these products at inclusion. Any patient requiring the initiation of such treatment after the study start was dropped from the study.
Experimental procedures
After obtaining signed informed consent, eligible patients were randomized to one of the treatment groups using a computer-generated randomization list. Their demographic data was recorded. Treatment was either 7% HS or Hyaneb administered by bronchial inhalation, twice a day for a period of 28 days.
FEV1 was measured before and 1 h after the inhalation of the test or control product. This 1 h time period was necessary to allow the bronchi to return to normal as there is risk of bronchospasm in some patients after inhalation of HS [Ratjen, 2006]. Each patient was required to complete a questionnaire after inhalation about the symptoms of cough, thoracic constriction, throat irritation and saltiness, and also express a pleasantness judgment on the assigned treatment. Each item was assessed using a four-point ordinal score: 1 = absent; 2 = light; 3 = moderate, and 4 = severe. The measure of pleasantness was scored using a scale from 0 to 5: 0 = disgusting and 5 = neutral.
A short-acting β2 bronchodilator was to be administered in the case of bronchospasm. The pulmonary examination was to be repeated and FEV1 was to be evaluated until normalization.
After treatment at the baseline visit, patients who tolerated the assigned treatment received treatment sufficient for a period of 28 days, to be administered twice a day at home. They also received a patient diary in which they recorded their judgements on the tolerability and pleasantness of the assigned treatment on a weekly basis, preferably on days 7, 14, 21, and 28. The need for β2 bronchodilators was also to be recorded daily. Patients who did not tolerate the assigned treatment at the baseline visit, even after using a β2 bronchodilator, were dropped from the study.
At end of the final treatment visit (4 weeks after the baseline visit), a clinical examination was carried out which included cardiac and respiratory frequency, oxygen saturation, and pulmonary function tests. Spirometry was performed before and after inhalation of the assigned treatment to obtain the FEV1 values and each patient was required to complete the evaluation questionnaire and also express a pleasantness judgment on the assigned treatment. Patients returned the unused test product for an assessment of compliance. The patient diary was collected for evaluation and all adverse events were recorded.
Sample size calculation and statistical analysis
Although this was an exploratory study, an estimate of sample size was based on cough and throat irritation perceptions. Thirty patients (15 patients per group) were judged to be appropriate to detect a difference between treatments of 0.4 in the proportion of patients experiencing cough and throat irritation with a power greater than 80% at the 0.05 level of probability for the Wilcoxon test. Statistical analyses were conducted on full-set data.
The Wilcoxon rank sum test and the Cochran-Mantel-Haenszel test corrected for time were applied to analyze cough, irritation, thoracic constriction, saltiness, and final judgment. FEV1 values and β2 bronchodilator consumption were analyzed using Student’s t test. β2 bronchodilator consumption during the 4 weeks of treatment was also analysed by analysis of variance for repeated measures. Descriptive statistics were used for demographic data. A statistical threshold of 0.05 was set for a two-tail test.
Three patient populations were assessed: the safety set, which included all patients who had received at least one nebulization of either the test or control product; the intention-to-treat (ITT) population, which was defined as patients who received at least one nebulization of either the test or control product and returned for at least one visit thereafter; while the PP population was defined as patients who completed the study protocol without major protocol deviations
Results
Thirty male and female patients with CF were enrolled in the study for a 4-week treatment period. One patient in the HS group dropped out of the study after the baseline visit, while two patients (one in the Hyaneb group and one in the HS group) did not complete the diary but attended all the visits. Missing data were not substituted and hence the data of 27 patients were analysed. The disposition of the patients is presented in Figure 1.

Disposition of the patients.
Five of the 30 patients were below 10 years of age but were still included as it was felt that they would benefit from treatment. The two study groups were homogeneous at baseline for demographic characteristics and spirometric evaluation (Table 1).
Demographic data and spirometric evaluation.

CLM, confidence limits of the mean; FEV1, forced expiratory volume in 1 s; NS, nonsignificant.
Table 2 shows the spirometric evaluations of FEV1 (% of predicted value) at baseline and at the end of the study (week 4) in the ITT and per protocol (PP) populations. There were no statistically significant differences between groups for age and FEV1 at baseline.
Spirometric evaluation at baseline and at 4 weeks.

FEV1, forced expiratory volume in 1 s; ITT, intention to treat; PP, per protocol; SD, standard deviation.
Spirometric evaluation of patients showed changes in FEV1 at baseline before and after treatment in both groups (see Table 3, 95% confidence limits not including zero). The change was greater in the HS group than in the Hyaneb group (4.3 versus 2.2 respectively). In contrast, after 4 weeks of treatment no differences before and after treatment were observed as demonstrated by 95% confidence limits that did not include zero.
Spirometric evaluation and β2 bronchodilator consumption.

(n), mean ± SD, 95% confidence interval difference.
Cochran Mantel-Haenszel test p= 0,0070 corrected for time, Cochran–Mantel–Haenszel test, p = 0.0070; analysis considered in the model the correction for time.
Analysis of variance for repeated measure: treatment p < 0.0001; week p ≤ 0.0001; treatment * week p < 0.001.
Student’s t test, p < 0.0001; 95% confidence limits −1.3 to −1.1.
FEV1, forced expiratory volume in 1 s; SD, standard deviation.
The consumption of β2 bronchodilators was statistically significantly lower in the Hyaneb group compared with the HS group (Table 3). At baseline, only one patient (6.7%) in the Hyaneb group required β2 bronchodilators compared with seven patients (47.7%) in the HS group. At the end of the study, two patients (14.3%) in the Hyaneb group required β2 bronchodilators compared with five (35.7%) in the HS group. This is in agreement with a lower incidence of bronchoconstriction experienced by patients who inhaled Hyaneb (Table 4).
Symptom questionnaire.

Throughout the study, patients in the Hyaneb group required significantly fewer puffs (mean = 0.2 ± 0.6 puffs) compared with the HS group (mean = 1.4 ± 0.9) (p < 0.0001; 95% confidence limits −1.3 to −1.1) (Table 3). This result is confirmed by analyzing the patient questionnaire, in which cough and throat irritation were statistically significantly lower (p = 0.0010) in favour of the Hyaneb group (Table 4) while constriction (Table 4) showed only a trend to significance (p = 0.0646). In fact, at baseline six patients (42.8%) in the Hyaneb group had no cough compared with four (26.7%) in the HS group. By week 4, 11 patients (78.6%) in the Hyaneb group had no cough compared with 3 (23.0%) in the HS group.
The results for throat irritation are also impressive (Table 4). Most of the patients in the Hyaneb group had none or light throat irritation throughout the study while patients in the HS groups had light to moderate throat irritation. At baseline 14 patients (100%) in the Hyaneb group had no throat irritation or light irritation compared with 11 (73.3%) in the HS group. However, at this time point, three patients (20.0%) in the HS group had moderate and one (6.7%) had severe throat irritation. By week 4, 10 patients (71.4%) in the Hyaneb group had no irritation and four (28.6%) had light irritation compared with eight patients (61.5%) with no irritation and three (23.1%) with light irritation in the HS group. At this assessment point, two patients (15.4%) in the HS group compared with none in the Hyaneb group had moderate throat irritation.
Concerning the pleasantness of treatment, most of the patients (92.8–100%) in the Hyaneb group reported an absence of taste or only a light salty taste sensation throughout the study after nebulization. In contrast, between 46.7% and 69.3% of the patients in the HS group reported an absence of taste or only a light salty taste sensation throughout the study (see Table 4), with a significant difference (p < 0.0001) in favour of the Hyaneb group.
The overall judgment of treatment pleasantness was significantly different in favour of the Hyaneb group compared with the HS group (see Table 5). Using a five-point scale (1 = disgusting; 2 = unpleasant; 3 = acceptable; 4 = more than acceptable; 5 = neutral), none of the patients in the Hyaneb group found the treatment disgusting or unpleasant throughout the study. In fact, all the patients in the Hyaneb group judged the treatment as being acceptable, more than acceptable and neutral. In contrast, between 23.1% and 40% of the patients in the HS group judged treatment to be disgusting or unpleasant throughout the study.
Diary questionnaire on treatment judgment.
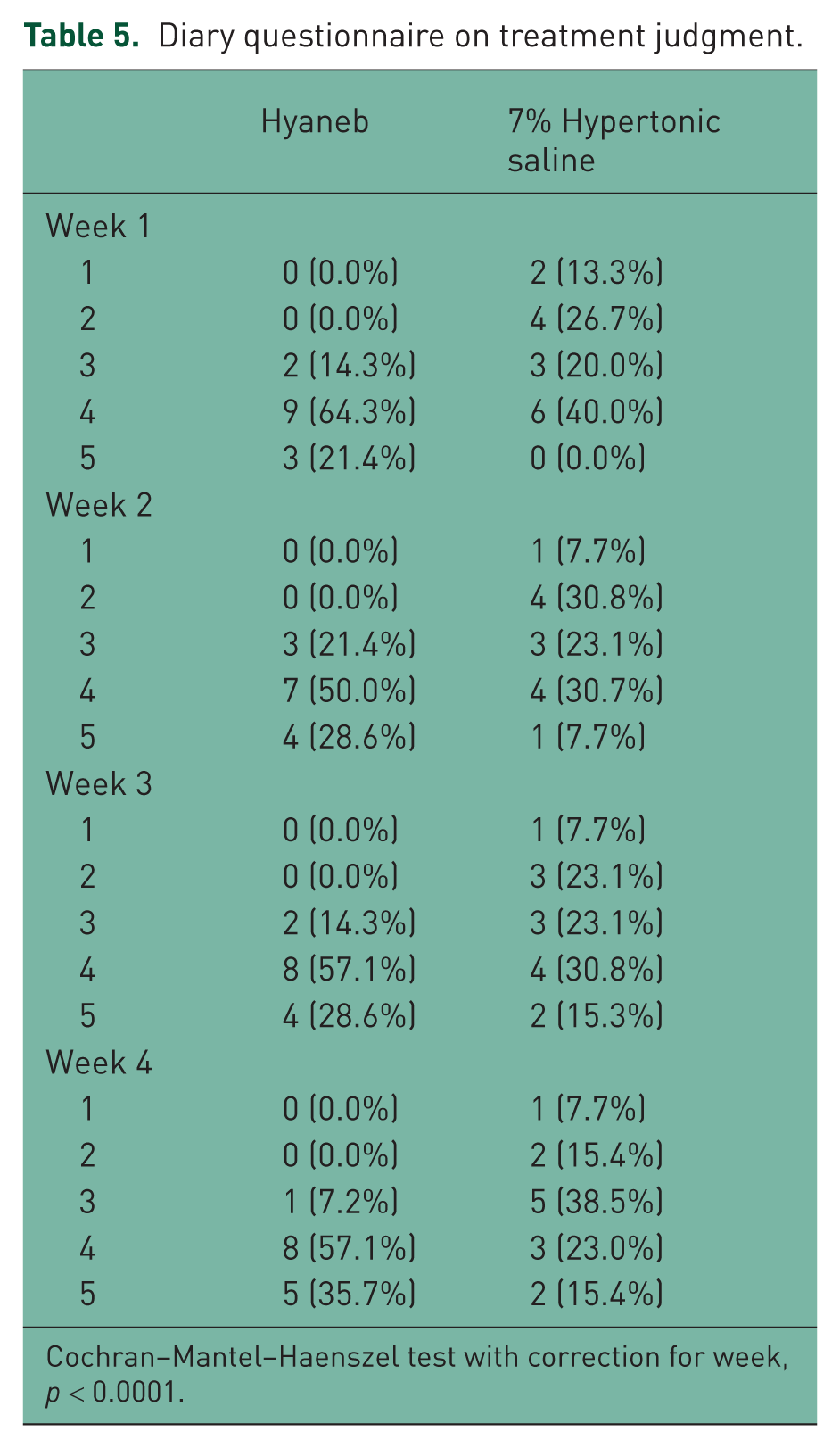
Cochran–Mantel–Haenszel test with correction for week, p < 0.0001.
No adverse events were reported in either group during the study.
Discussion
Nebulization treatment with 7% HS solution is a recommended treatment in patients with CF and lung disease and short-term clinical studies have demonstrated the efficacy and tolerability of such therapy [Matsui et al. 1998]. HS solution has been shown to increase the hydration of the airways by increasing the airway surface liquid [Donaldson and Boucher, 2007; Matsui et al. 1998], resulting in an improvement in mucociliary clearance, increased pulmonary function, reduced number of exacerbations, and an improved quality of life of the patients [Matsui et al. 1998]. However, some patients experience adverse reactions such as bronchial constriction, cough, chest tightness, and throat irritation and many require β2 bronchodilator before HS inhalation, resulting in about 10% of the patients dropping out [Buonpensiero et al. 2010]. Under such circumstances, an effective treatment with HS cannot be assured and some patients may never start such a treatment. Patients also complain about the saltiness of the HS solution. The above problems lead to decreased treatment compliance even in the short term and some patients stop treatment after a short time.
The results of our study support data reported in other studies which report an improvement in the tolerability and acceptability of HS in the treatment of lung disease in patients with CF with similar efficacy. The known adverse event profile of HS was also confirmed in our study. Patients’ judgment of HS treatment remained constant during the 4 weeks of inhalation treatment but with a worsening trend in some cases. The saltiness of the HS solution was also mentioned as being marked.
The addition of HA to the 7% HS solution significantly improved the safety of the nebulization treatment. Not only was a statistically significant decrease in β2 bronchodilators observed in the Hyaneb group compared with the HS group, but this was supported by the observations of a lower incidence of bronchoconstriction, cough, and throat irritation in the patients who inhaled nebulized Hyaneb. The reduction in β2 consumption was not because patients refused the bronchodilating premedication but rather due to a reduced bronchoreactivity as a result of a lower irritant effect on bronchial muscles. The above data demonstrate that Hyaneb resulted in a considerable improvement in tolerability compared with the 7% HS alone.
Data not reported in this paper confirm the overlapping effects of both treatments on mucus production.
It is unknown how HA is able to reduce all the side effects of HS inhalation. It is possible that the hydration effect of the HA present in Hyaneb plays a major role in increasing the hydration of the airways, thus reducing the adverse effects due to HS alone. By regulating fluid balance in the interstitium through it high water-binding capacity, HA facilitates ventilation and gas exchange [Schmid et al. 1982]. In addition, by mitigating the actions of human neutrophil elastase and human macrophage metalloelastase in animal models of pulmonary emphysema, HA may exert a protective effect on the airways [Turino and Cantor, 2003].
In conclusion, the good safety profile of Hyaneb, and its similar efficacy compared with HS alone, suggests its use in the treatment of patients with CF and lung disease.