
Abstract
Background:
Balloon dilation is a primary treatment for nonmalignant tracheobronchial stenosis, but often requires multiple treatment sessions to maintain therapeutic efficacy. No guideline is available to suggest the appropriate maximum number of treatment sessions. This study aimed to investigate the relationship between the number of balloon dilation sessions and its long-term therapeutic effectiveness in Chinese patients with nonmalignant central airway stenosis.
Methods:
A total of 111 patients with nonmalignant central airway stenosis treated with flexible bronchoscopic balloon dilation from January 2005 to September 2012 were included. The cumulative long-term effective rate was compared between any two adjacent sessions of balloon dilation treatment by McNemar’s test. Multivariate Cox regression was performed to investigate the independent factors associated with long-term effectiveness.
Results:
The cumulative long-term effective rate was significantly increased between any two adjacent sessions before the 6th session of treatment (all p < 0.05) but was no longer significantly increased after the 6th session. The stenosis diameter was larger in the patients receiving ⩽6 treatment sessions than those receiving ⩾6 treatment sessions. Multivariate Cox regression showed that the treatment session was an independent factor associated with long-term effectiveness (hazard ratio = 0.65, 95% confidence interval: 0.57–0.76, p < 0.001).
Conclusion:
These results suggest that the maximum number of treatment sessions of balloon dilation may be six, and patients requiring more treatment sessions were more likely to have delayed long-term effectiveness.
Keywords
Introduction
Nonmalignant central airway stenosis refers to tracheobronchial stenosis caused by nonmalignant lesions in the trachea and mainstem bronchi. 1 The gold standard treatment for nonmalignant airway stenosis is surgical resection of the stenotic tracheal segment, followed by end-to-end anastomosis with reconstruction.2,3 However, for patients with a long stenosis length, surgical resection and reconstruction are challenging and often cause postoperative complications. 4
Flexible bronchoscopic balloon dilation is a simple, minimally invasive method used for dilating airway stenosis, 5 which has become the primary treatment for nonmalignant tracheal stenosis.6–9 Flexible bronchoscopic balloon dilation can provide immediate symptom relief, and does not increase the stenosis length after dilation. However, balloon dilation itself may cause secondary airway injury, and the overgrowth of granulation tissue during airway repair may cause restenosis. 10 Patients with significant restenosis require another session of dilation. Although repeated balloon dilation is generally well tolerated and rarely causes severe complications, overdilation may cause airway laceration and hemorrhage, leading to excessive scar hyperplasia and aggravating restenosis.11,12 Currently, there is no clinical guideline suggesting the appropriate number of dilation treatment sessions. Investigating the appropriate number of treatment sessions can prevent overdilation and the timely adoption of other treatments to improve the therapeutic outcome. Therefore, the purpose of this study was to investigate the relationship between the number of balloon dilation sessions and long-term therapeutic effectiveness in Chinese patients with nonmalignant central airway stenosis to identify the appropriate maximum number of treatment sessions.
Methods
Patients
From January 2005 to September 2012, there were 422 patients with nonmalignant central airway stenosis treated in the First Affiliated Hospital of Guangzhou Medical University (Figure 1). Among them, 150 (35.5%) patients received flexible bronchoscopic balloon dilation, and 148 (98.7%) and 111 (74.0%) cases achieved short-term and long-term effectiveness, respectively. A total of 38 patients had short-term effectiveness but had no long-term effectiveness. These 38 patients then received other treatment for central airway stenosis and were excluded. The 111 patients with long-term effectiveness were included in this study. The inclusion criteria included patients with: (1) confirmed diagnosis of nonmalignant central airway stenosis by computed tomography (CT), chest X-ray, bronchoscopy, clinical or pathological findings; (2) achievement of long-term effectiveness of the flexible bronchoscopic balloon dilation. Patients with malignant airway stenosis, congenital airway stenosis, airway stenosis caused by external compression, endogenous stenosis or bracket placement were excluded. This study was approved by the institutional review board of the First Affiliated Hospital of Guangzhou Medical University, China. Written informed consent was waived by the institutional review board due to the retrospective nature of this study.
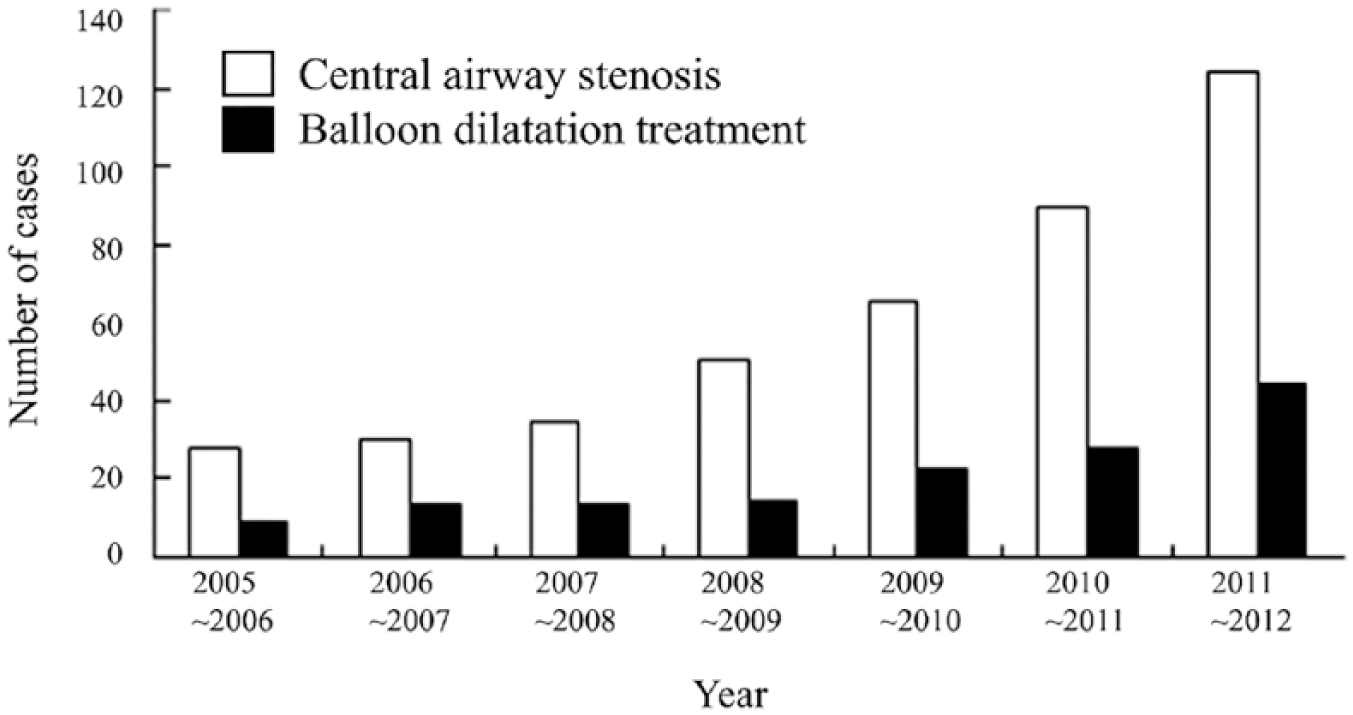
The number of patients with nonmalignant central airway stenosis in our hospital and the number undergoing dilation treatment.
Data collection and definitions
The demographic and clinical data of all patients were retrospectively collected from their medical records. The causes of nonmalignant central airway stenosis included endobronchial tuberculosis, endotracheal intubation or tracheotomy, lung transplantation or sleeve resection, trauma, aspiration injury, foreign body, relapsing polychondritis and unknown cause. The stenosis location included lower glottis and upper airway; middle airway; lower airway and carina; left main bronchus; right main bronchus; right middle lobe bronchus; lower airway, carina and both primary bronchi. The degree of stenosis was classified according to the central airway stenosis classification proposed by Freitag and colleagues as follows: code 1: 25% decrease (in cross-sectional area); code 2: 50% decrease; code 3: 75% decrease; code 4: 90% decrease; code 5: 100% decrease. 13 The dyspnea index was defined using the dyspnea rating criteria of the American Thoracic Society as follows: Level 0: normal; Level 1: dyspnea while fast walking; Level 2: dyspnea while walking at a normal speed; Level 3: stopping normal speed walking for dyspnea; Level 4: dyspnea after mild exercise. 14 The range of the stenosis segment was defined based on three-dimensional reconstruction of the chest CT or direct measurement under bronchoscopy.
Flexible bronchoscopic balloon dilation
All patients underwent examinations including routine bloods, coagulation function, fasting blood glucose, chest X-ray film, chest CT scan, arterial blood gas analysis and routine bronchoscopy, before the balloon dilation treatment. Three-dimensional reconstruction of the tracheobronchial CT examination was performed to identify the extent, length, location of the stenosis and the lesions of the distal airway and lungs if necessary.
The anesthesia methods including local anesthesia, local anesthesia combined with intravenous sedation and analgesia, and general anesthesia, were chosen based on the patient’s age, condition, the degree of tracheal stenosis and systemic condition. The size of the balloon was determined based on the diameter and length of the airway stenosis. The balloon dilation was guided by a flexible bronchoscope with an outer diameter of 6 mm. A small balloon and a low pressure were adopted for the first session of dilation. Then the diameter of the balloon and pressure were gradually increased in the following sessions. During the treatment, the balloon was fully inflated or inflated until the patient could not tolerate it, to reach a pressure of 3–10 times atmospheric pressure for 20 to 120 sec. After which, the balloon was emptied, and then dilated again at an interval of 2–3 min for 3–4 rounds. Postoperative complications such as local bleeding and mucosal injury and airway diameter were recorded. After 3 to 7 days, bronchoscopy was performed to observe the dilation of the stenosis, and patients with unsatisfactory treatment outcomes would receive the next session of balloon dilation. The 3–4 rounds of balloon dilation within the same day were defined as one session of treatment. Re-dilation after 3 to 7 days was defined as the second session of dilation treatment. 8 If the stenosis was still not improved, the dilation was suspended and other treatments were considered. All of the 111 cases included in this study were treated with balloon dilation alone.
For patients with significant scar tissue on the stenotic airway, the scar tissue was cut by electrosurgical needle (output power = 20–40 W) guided by bronchoscopy prior to the balloon dilation.
Follow up
All patients were regularly followed up every 1–3 months for at least 1 year. The follow-up examinations included clinical physical examination, airway ultrasound, bronchoscopy, chest X-ray or CT scan. Patients with restenosis confirmed by clinical findings or bronchoscopy received the next session of balloon dilation. Restenosis was defined as a recurrence of stenosis or a stenosis at the same location after a period of time. 8
Short-term therapeutic efficacy
Short-term therapeutic efficacy was defined according to Bergler and colleagues’ study 15 as follows: (1) Completely effective: complete removal of the lesions in the airway, and full functional recovery; (2) Partially effective: the diameter of the stenotic airway was dilated ⩾50%, the symptoms were relieved, and the function was mainly normal; (3) Mildly effective: the diameter of the stenotic airway was dilated <50%, the distal stenosis was absorbed and dissipated by drainage, and pneumonia at the distal stenotic airway was dissipated by drainage; (4) Invalid: no subjective or objective evidence of clinical improvement. Airway diameter and cross-sectional stenosis rates were measured using a 6-mm bronchoscope and calculated by a self-developed image measurement software. 16
Long-term therapeutic efficacy
The long-term therapeutic efficacy of balloon dilation was determined as previously described 17 : (1) Cure: initial successful dilation of the airway, improvement of symptoms, and the diameter of the dilated airway was stable for more than 1 year; (2) Effective: initial successful dilation, improvement of symptoms, and the diameter of the dilated airway was stable for more than 3 months but less than 1 year; (3) Invalid: initial successful dilation, improvement of symptoms, and the diameter of the dilated airway was stable for less than 3 months or final airway occlusion occurred; (4) Failure: initial unsuccessful dilation. According to the above efficacy evaluation, patients with ‘cure’ (the diameter of the dilated airway was stable for more than 1 year) were defined as having long-term effectiveness.
Statistical analysis
Continuous data were expressed as the mean ± SD (standard deviation) and compared by a Student’s independent t-test. If normality was not assumed, a Mann–Whitney U test would be used for comparisons between groups. Categorical data were indicated by the number and percentage (%) and compared by a Chi-squared test or Fisher’s exact test (if an expected value ⩽5 was observed). McNemar’s test was used to test the difference between two rates within the same group (dependent data). Univariate and multivariate Cox regression models were used to investigate the association of independent variables to the patient’s long-term effect. For the variables which were significant in both univariate and multivariate results, these were seen as associated factors of the patient’s long-term effect. Since the endpoint of the patient was reaching a long-term effect, the parameters estimated by survival analyses should be interpreted as a ‘good’ outcome (and not a hazard viewpoint). For example, a hazard ratio (HR) >1 would indicate a tendency of reaching a long-term effect. The significance level of all analyses was set at a p value <0.05 and was two-tailed. All analyses were performed using SPSS version 20 (SPSS Statistics, IBM Corporation, Somers, NY, USA).
Results
Demographic and clinical characteristics
A total of 111 patients (30 men and 81 women, mean age = 33.98±14.05 years) with a long-term effectiveness were included in this study. As shown in Table 1, the major cause of nonmalignant central airway stenosis was endobronchial tuberculosis (n = 76, 68.5%), followed by endotracheal intubation or tracheotomy (n = 23, 20.7%). Regarding the degree of stenosis, there was 1 patient (0.9%) in code 2; 36 (32.4%) patients in code 3; and 74 patients (66.7%) in code 4. Other clinical characteristics, including the location, diameter, and length of stenoses are summarized in Table 1.
Patient’s demographic and clinical characteristics.
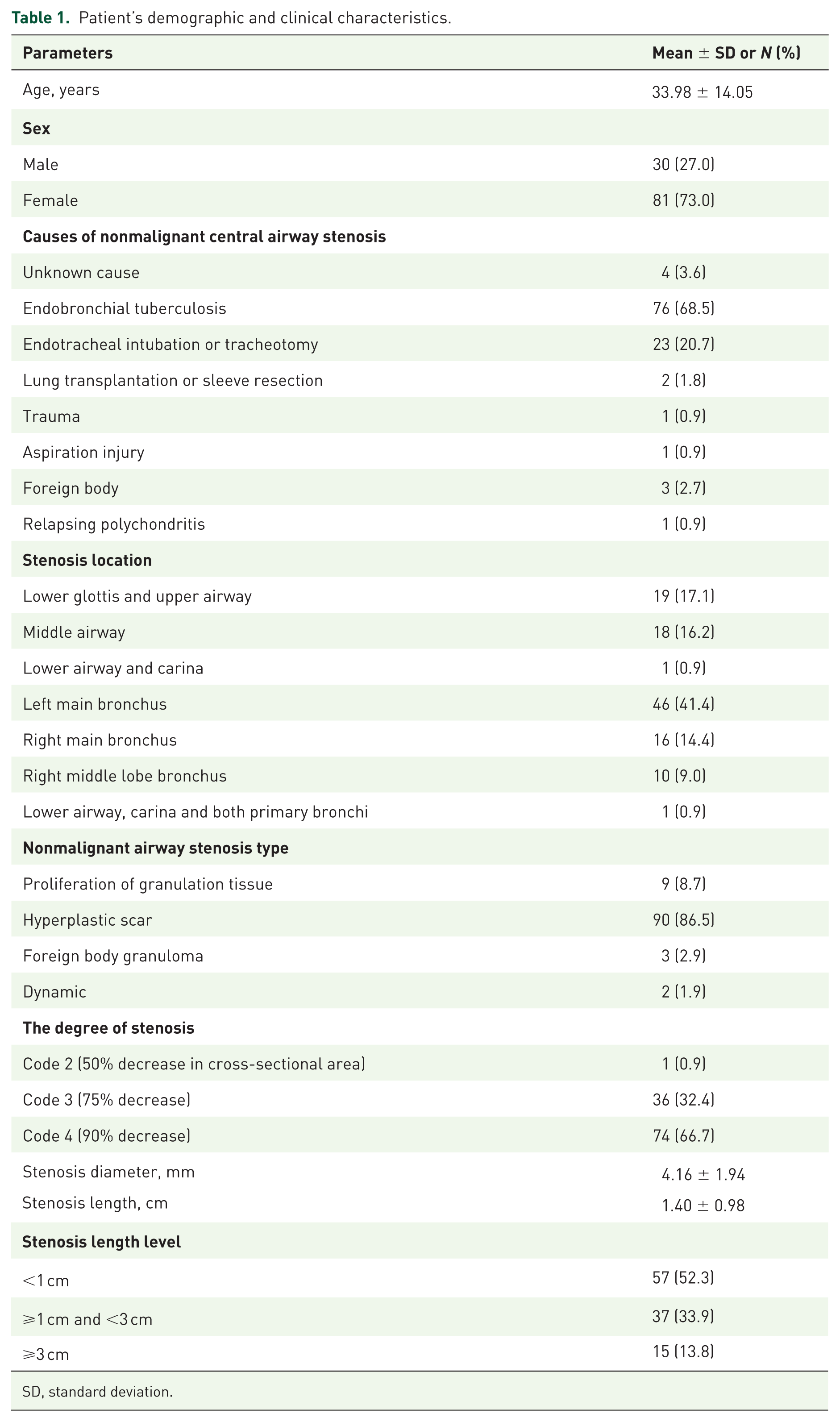
SD, standard deviation.
Symptoms and treatments
Patients’ symptoms are listed in Table 2, including 15 (16.9%) fever, 1 (1.1%) rigor, 82 (92.1%) cough, 68 (76.4%) phlegm, 61 (68.5%) dyspnea, 14 (15.7%) wheezing and 2 (2.2%) chest pain. All patients underwent balloon dilation, while 26 (23.4%) patients underwent scar cutting by an electrosurgical needle prior to balloon dilation. The mean number of balloon dilation treatment sessions was 2.92 ± 2.49 (median: 2, range: 1–14) and the mean overall treatment duration was 63.49 ± 222.71 days (median: 7, range: 1–1796).
Treatment and symptoms.

SD, standard deviation.
Post-dilation complications
The post-dilation complications included different levels of mucosal injury (n = 111, 100%), severe bronchial laceration (n = 6, 5.4%) and slight mediastinal emphysema (n = 2, 1.8%), which was resolved by symptomatic treatment. A total of 101 (91.0%) patients complained about slight chest pain intraoperation or post-operation, which was tolerable and not needing to be treated. All patients had slight bleeding post-dilation. A total of 90 (81.1%) patients had a little bleeding and needed no specific treatment, while the other 21 (18.9%) patients had bleeding of 10–15 ml which was treated with local spraying of adrenaline (1:20,000 dilution). No other severe complications were observed.
Long-term effectiveness
To analyze the maximum appropriate sessions of balloon dilation treatment, the relationship between long-term effectiveness and the number of treatment session of balloon dilation was investigated. As shown in Table 3 and Figure 2, the cumulative long-term effective rate was 36.0% after the first session of treatment, but significantly increased between any two adjacent sessions before the sixth session of treatment (all p < 0.05). After dilation over the sixth session, the cumulative long-term effective rate was no longer significantly increased. These results suggest that six sessions may be the appropriate maximum number of balloon dilation treatments.
Cumulative long-term effective rate after each treatment session.
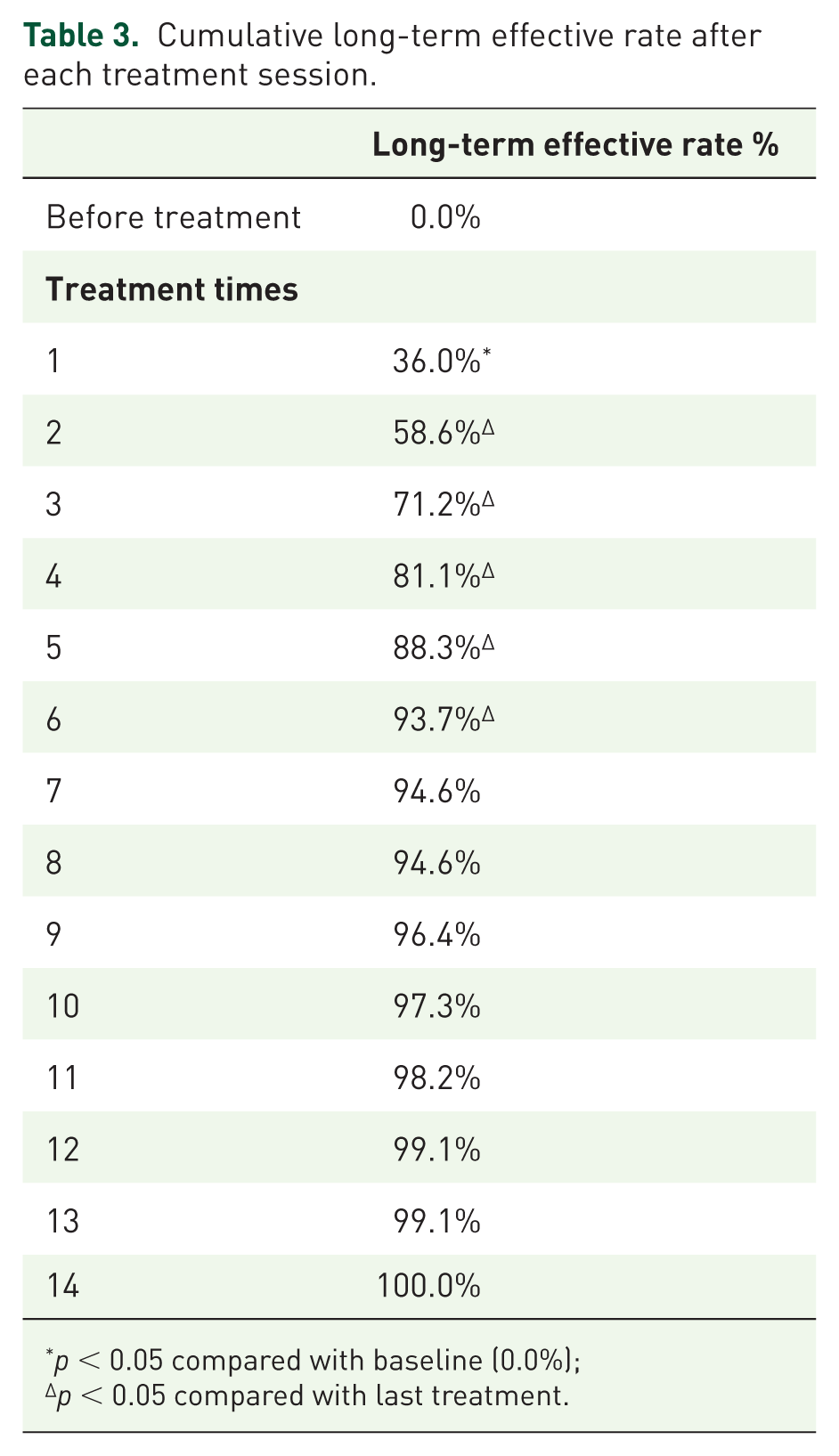
p < 0.05 compared with baseline (0.0%);
p < 0.05 compared with last treatment.

Long-term effective rate after each dilation treatment.
To perform a treatment session-stratified subgroup analysis, all patients were dichotomously divided into two subgroups using six sessions as a cutoff: ⩽6 sessions (n = 104) and >6 sessions (n = 7) groups. It was found that patients with ⩽6 treatment sessions had a larger stenosis diameter (4.27 ± 1.95 versus 2.57 ± 0.53 cm, p = 0.004; Table 4). The difference in the degree of stenosis between the two subgroups reached marginal significance (p = 0.052; Table 4).
Patient’s clinical characteristics by treatment sessions.

Association of the independent variables with long-term effectiveness
Next, the univariate and multivariate Cox regression was performed to investigate the independent factors associated with long-term effectiveness. The multivariate model was adjusted for significant variables in the univariate model, patients’ age, sex, and degree of stenosis. As shown in Table 5, the treatment session was the only variable significant in the multivariate model [HR = 0.65, 95% confidence interval (CI): 0.57–0.76, p < 0.001], indicating that patients requiring more treatment sessions were more likely to have a delayed long-term effectiveness.
Cox regression models of independent variables associated with long-term effectiveness.

CI, confidence interval; HR, hazard ratio.
Discussion
In this study, we investigated the relationship between the number of balloon dilation sessions and long-term therapeutic effectiveness in Chinese patients with nonmalignant central airway stenosis. The cumulative long-term effective rate was significantly increased between any two adjacent sessions before the sixth session of treatment but was not significantly increased after the sixth sessions. Multivariate Cox regression analysis showed that the number of treatment sessions was the factor associated with long-term effectiveness (HR = 0.65, 95% CI: 0.57–0.76, p < 0.001). Taken together, these results suggest that six sessions may be the maximum appropriate number of balloon dilation treatments, and patients requiring more treatment sessions are more likely to have delayed long-term effectiveness.
It was found that the cases of nonmalignant central airway stenosis gradually increased within the 7 years of this study. Our data showed that patients younger than 45 years accounted for more than 70% of all cases. Flexible bronchoscopic balloon dilation is a well-tolerated and effective method for the dilation of airway stenosis, 18 and has been widely used for the primary treatment of airway stenosis. Our data showed that patients receiving balloon dilation accounted for 35.55% of all cases of nonmalignant central airway stenosis over the 7-year duration of the study. The short-term effective rate of balloon dilation was 98.67% (148/150), and the long-term effective rate was 73.33% (110/150). The incidence of post-dilation complications was low. In clinical practice, balloon dilation is more frequently adopted for patients with a stenosis degree of 3 or 4. In this study, the patients mainly had a stenosis degree of 3 and 4, accounting for 90.99% (101) of all patients.
In balloon dilation treatment for nonmalignant airway stenosis, multiple treatment sessions are often required to maintain therapeutic efficacy. When the initial therapeutic efficacy is unsatisfactory, it is crucial to determine whether further sessions of treatment should be continued. Investigating the appropriate maximum number of treatment sessions is helpful in making the treatment decision. Regarding studies of the number of treatment sessions of balloon dilation for nonmalignant central airway stenosis, Li and colleagues reported that the mean sessions of balloon dilation treatment of 114 cases of nonmalignant central airway stenosis was 3.22 ± 1.24. 19 Li and colleagues demonstrated that among 12 patients undergoing balloon dilation with mean treatment sessions of 3.5, 18% of the patients developed restenosis within 6 months after dilation. 20 In this study, we retrospectively analyzed the medical records of 111 cases of nonmalignant central airway stenosis, and found that dilation over the sixth session no longer significantly increased the cumulative long-term effective rate, which is in line with the current clinical situation. This finding suggests that six sessions may be the maximum appropriate number of balloon dilation treatments. It is recommended that other therapies should be considered if the long-term effectiveness of balloon dilation still cannot be achieved after six sessions of treatment.
In this study, there were seven patients receiving more than six sessions of balloon dilation. All these seven patients had a stenosis degree of four. Treatment session-stratified subgroup analysis showed that the difference in the degree of stenosis between the ⩽6 sessions and the >6 sessions groups reached marginal significance (p = 0.052). Therefore, further investigation is needed on whether the preoperative degree of stenosis has an effect on long-term effectiveness. Among seven cases in the >6 sessions group, the stenoses were all located in the bronchus (Table 4), implying that therapeutic efficacy might be relatively worse in the bronchus segment than other segments. However, there was no significant difference in the stenoses location between the ⩽6 sessions and >6 sessions groups, which may be attributed to the small sample size of the >6 sessions group. On the other hand, the stenosis diameter was significantly larger in the patients receiving ⩽6 treatment sessions than those receiving >6 treatment sessions, suggesting that the preoperative stenosis diameter may influence the therapeutic outcome. However, multivariate Cox regression analysis did not support that stenosis diameter is a factor associated with long-term effectiveness. Therefore, the effect of degree of stenosis, stenosis location and stenosis diameter on long-term effectiveness of balloon dilation needs to be further evaluated.
The most common causes of nonmalignant central airway stenosis are granulation tissue resulting from the endotracheal tube, tracheostomy tube, or airway foreign bodies, and tracheobronchomalacia.1,21 Other less common causes include infectious diseases, chronic inflammatory diseases and collagen vascular diseases. 21 Nevertheless, because of the high tuberculosis incidence in China, 22 endobronchial tuberculosis has been reported in an etiology study (n = 368) by Li and colleagues, to be the most common cause of nonmalignant central airway stenosis in China, followed by prolonged orotracheal intubation or tracheotomy. 23 Consistently, in this study, endobronchial tuberculosis was the most common cause (68.5%), followed by endotracheal intubation/tracheotomy (20.7%). It has been shown that the therapeutic efficacy of balloon dilation for tuberculosis-induced nonmalignant central airway stenosis is good, with high short- and long-term effective rates. 24 Among the 111 patients in this study, the causes of nonmalignant central airway stenosis had no effect on the therapeutic efficacy of balloon dilation. Nevertheless, in the 12 cases other than tuberculosis, endotracheal intubation or tracheotomy, the number of treatment sessions of balloon dilation were fewer than six. This phenomenon is in agreement with the previous observation that nonmalignant central airway stenosis caused by nonmalignant tumors, foreign body or localized scars could be cured by a single session of balloon dilation. 25 Animal studies have demonstrated that respiratory infection is a risk factor for the occurrence or aggravation of airway stenosis.26,27 Among the 111 patients, 81 patients had infectious symptoms such as fever, cough and phlegm. However, we did not collect data on sputum etiology and serum inflammation markers. Hence, the impact of respiratory infections on the therapeutic efficacy of balloon dilation remains to be further investigated.
Several limitations of this study should be mentioned. First, this was a retrospective study, and the sample size was relatively small. In the future, a prospective trial will be necessary to validate the findings of this study. Moreover, it is worth investigating whether the nonmalignant central airway stenoses with different causes have different appropriate maximal maximum numbers of treatment sessions. All these should be addressed in future studies.
In summary, our findings suggest that the maximum number of treatment sessions of balloon dilation may be six, and that patients requiring more treatment sessions were more likely to have delayed long-term effectiveness.
Footnotes
Acknowledgements
We thank Professor Yu Chen and the doctors and nurses at the Bronchoscopy Center of the First Affiliated Hospital of Guangzhou Medical University, China for their great support.
Funding
This work was supported by the medical scientific research project of Foshan Health and Family Planning Bureau, China (20160131).
Conflict of interest statement
The authors declare that there is no conflict of interest.