
Abstract
Background:
Fluticasone furoate/vilanterol (FF/V) is an effective long-acting β2 agonist/inhaled corticosteroid combination for managing persistent bronchial asthma. The aim of the study was to assess the outcomes achievable in patients with mild to moderate asthma receiving FF/V 92/22 µg once daily for 12 months.
Methods:
Data were automatically and anonymously obtained from the institutional database: forced expiratory volume in 1 s predicted values; the exacerbation and hospitalization rates; days of hospitalization; general practitioner (GP) or specialist visits; days of inactivity; courses of systemic steroids or antibiotics were recorded at baseline and after 3, 6 and 12 months of treatment. The overall adherence to treatment was also calculated. Analysis of variance was used for checking the trends of variables. The improvement in lung function was significant (p < 0.001) and time dependent. The mean (±standard error) exacerbation rate per patient changed from 1.05 (±0.16) at baseline to 0.28 (±0.07) after 3 months, 0.33 (±0.08) after 6 months and 0.18 (±0.08) after 12 months (p < 0.001). The mean hospitalization rate per patient changed from 0.30 (±0.07) at baseline to 0.08 (±0.04) after 3 months, 0.10 (±0.05) after 6 months and 0.03 (±0.03) after 12 months (p < 0.001). Also mean duration of hospitalization and days of inactivity were reduced over time (p < 0.001). GP visits were also reduced, together with specialist visits (both p < 0.001). Steroid and antibiotic courses dropped significantly (p < 0.001 and p < 0.001, respectively). Moreover, changes in all outcomes considered proved time dependent, particularly over the second semester. Finally, over time, adherence to treatment was high.
Conclusions:
The once-daily inhalation of combined FF/V 92/22 µg optimized systematically the exacerbation and hospitalization rates in mild to moderate asthma, together with all other outcomes over time. The effectiveness of FF/V 92/22 µg once daily proved to be time dependent over the period of the study.
Keywords
Introduction
Bronchial asthma is a chronic inflammatory disease of the airways. It is characterized by partially or totally reversible airflow limitation, bronchial hyperresponsiveness, and the periodic occurrence of relapses. 1
Activation of inflammatory cells within the airway mucosal, muscular and vascular structures represents the underlying mechanisms of asthma, which cause the release of several inflammation mediators and can lead to substantial airway remodelling.
Common signs of asthma are recurrent cough, dyspnoea, wheezing (at rest or during exercise), and chest tightness. 1 These clinical signs are of variable duration and can change among individuals or in the same subject over time. 2
Asthma is a very common condition all over the world. In particular, the Italian National Institute of Statistics (ISTAT) estimated a prevalence of asthma of 4.2% (4.3% in women, 4.2% in men) in Italy in 2012, 3 and the corresponding economic impact was estimated at about 5 billion euros per year in Italy. 4
Four levels of asthma severity are recognized: mild intermittent, mild persistent, moderate persistent and severe persistent, and each level depends on the frequency of symptoms; the lung function level [i.e. forced expiratory volume in 1 s (FEV1)]; the peak expiratory flow (PEF) variability; the consumption of short-term bronchodilators as needed; the reversibility of airway obstruction; the exacerbation rate; and the quality of life.
The main goal of asthma therapy is to achieve and maintain the control of the disease in real life, and a good quality of life. 2 The therapeutic strategy of asthma treatment includes two main categories of drugs: further to rescue medications which are used for relieving the symptoms of acute bronchoconstriction only, the controller medications should be assumed regularly in order to maintain disease control. As bronchial asthma is an inflammatory disease, inhaled corticosteroids (ICS) represent the first line of treatment, to which long-acting β2 agonist bronchodilators (LABAs) can be added. The combination of these two categories of drugs is the most recommended therapeutic strategy for persistent asthma. 1
One of the most recent LABA/ICS combinations for persistent bronchial asthma is fluticasone furoate/vilanterol (FF/V) 92/22 µg delivered via the Ellipta device (manufactured by GSK Pharma, London, UK).5–7 This combination covers 24 h and is assumed as a once-a-day regimen.
Aim
The aim of the present study was to assess the outcomes in patients with mild to moderate asthma 1 receiving FF/V 92/22 µg once a day over a 12-month treatment period.
Methods
The study consists of an observational, retrospective analysis of patients with mild to moderate asthma (mild n = 6 and moderate n = 34) referred over the period February–September 2015 to the Lung Unit of the Specialist Medical Centre (CEMS), Verona, Italy.
Data were obtained automatically and anonymously from the institutional, UNI EN ISO 9001-2008 validated database, and the classic Boolean algebraic formula was used for selection. 8 Selection criteria were the presence of documented mild to moderate asthma in subjects of both sexes, over 18 years of age, nonsmoker status, with normal cognitive function, stable respiratory condition (spirometrically assessed) in the last 2 weeks before the study start, receiving FF/V 92/22 μg once a day for the last 12 (±2) months. At baseline, sex, age, absolute and % predicted values of FEV1, and comorbidities of all patients were recorded. All patients were followed over 12 (±2) months. FEV1 values, number of relapses and of related hospitalizations, duration of hospitalization (in days), number of general practitioner (GP) or specialist visits, days of inactivity, and number of courses of systemic steroids and antibiotics were recorded over the study period at baseline and after 3, 6 and 12 months of treatment. Baseline values for outcomes were corresponding to values assessed over the 3 months preceding the index date for selection. Furthermore, as the inhaler device (Ellipta) is provided with a clear and precise dose counter, the patients’ adherence to treatment was also recorded monthly, and expressed in % inhalations versus the expected number of inhalations at each period of the study.
Data reported at baseline (which refer to the trimester before the index data for selections) and after 3 months of both treatments correspond to those already published in a previous study, which was limited to a 12-week observational period for the same cohort of patients. 9 Data collected from the same patient cohort after 6 and 12 months were used in the present study in order to complete the trend over 12 months of treatment.
Analysis of variance (ANOVA) was used to check the four-point trend of variables (baseline, 3, 6 and 12 months) recorded during treatment for all outcomes.
The study was approved by the R&CG Ethical Committee during the session officially held on 11 January 2016.
Results
Clinical data of 40 patients treated with FF/V 92/22 μg once a day were obtained. Characteristics of the entire cohort at baseline are summarized in Table 1. At baseline, male prevalence was 37.5%. Mean [±standard error (SE)] age was 50.2 (±2.43). Mean (±SE) FEV1 in liters was 2.5 (±0.12), mean (±SE) FEV1% predicted was 81.9% (±2.00). The proportion of patients with perennial allergy was 62.5% (25/40), while that for seasonal allergy was 37.5% (15/40). The percentage of patients with established comorbidities was 42.5%. The following comorbidities were reported: arterial hypertension (the most prevalent comorbidity, found in 10.4% of cases), kyphoscoliosis, obesity, severe depression, acquired immunodeficiency syndrome (AIDS), diabetes mellitus, severe osteoporosis and ischemic heart disease. Table 2 summarizes all changes calculated for each variable over the study period.
Characteristics of the entire cohort at baseline.
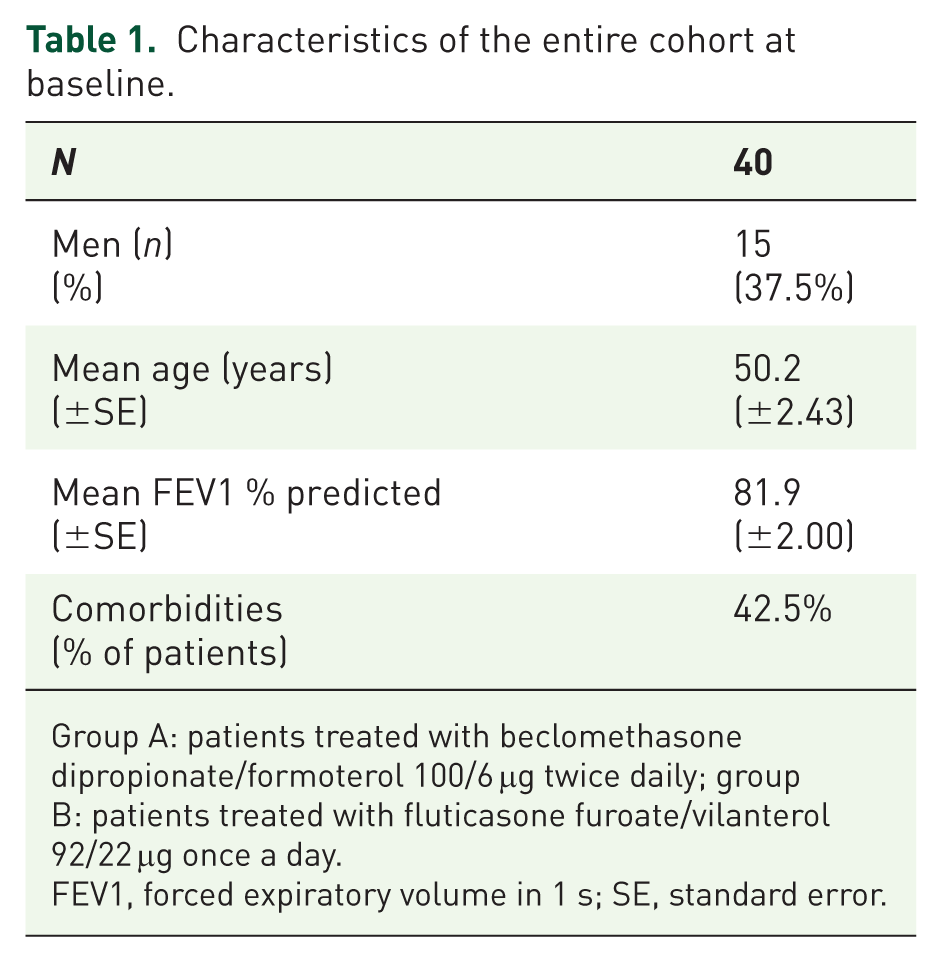
Group A: patients treated with beclomethasone dipropionate/formoterol 100/6 μg twice daily; group B: patients treated with fluticasone furoate/vilanterol 92/22 μg once a day.
FEV1, forced expiratory volume in 1 s; SE, standard error.
Means ± standard error (SE) for each variable calculated at baseline, and at 3, 6 and 12 months of treatment with fluticasone furoate/vilanterol (FF/V) 92/22 µg once daily via Ellipta.
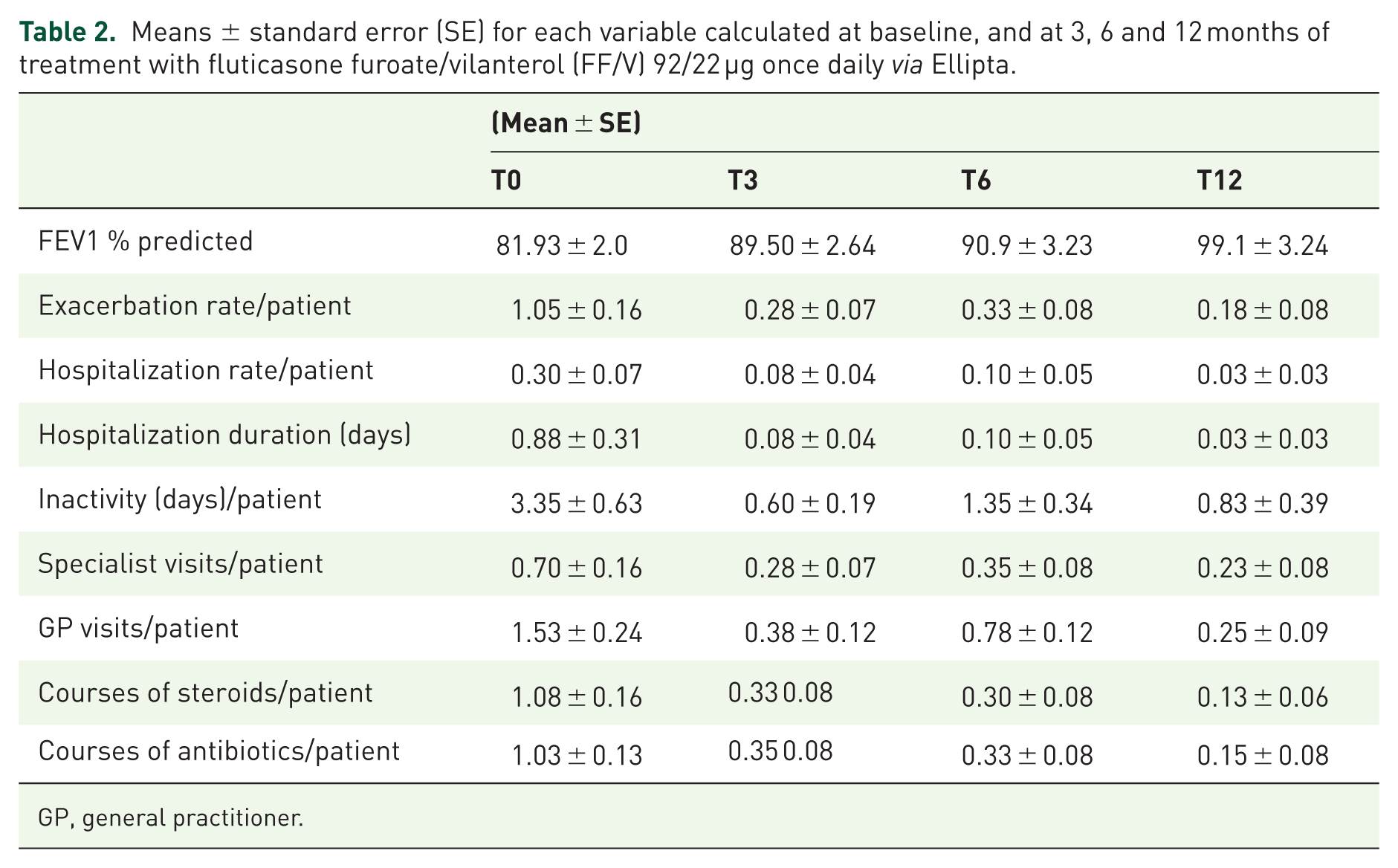
GP, general practitioner.
Mean FEV1 % predicted changed from 81.93% (±2.00) at baseline to 89.50% after 3 months, 90.9% after 6 months and 99.1% after 12 months of treatment (ANOVA, p > 0.001) (Figure 1).
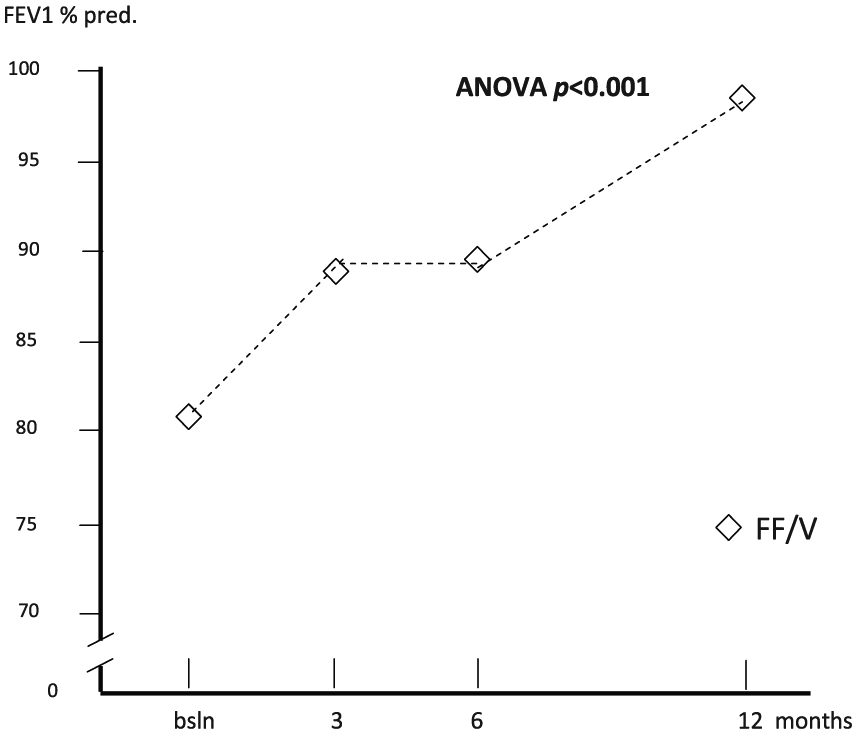
Changes in mean forced expiratory volume in 1 s % predicted (FEV1 % pred.) over 12 months. ANOVA, analysis of variance; bsln, baseline; FF/V, fluticasone furoate/vilanterol.
The mean (±SE) exacerbation rate per patient changed from 1.05 (0.16) at baseline to 0.28 (0.07) after 3 months, 0.33 (0.08) after 6 months and 0.18 (0.08) after12 months of treatment (ANOVA, p < 0.001) (Figure 2).

Changes in mean number of exacerbations per patient over 12 months. ANOVA, analysis of variance; bsln, baseline; FF/V, fluticasone furoate/vilanterol.
The average (±SE) rate of asthma-induced hospitalizations per patient changed from 0.30 (0.07) at baseline to 0.08 (0.04) after 3 months, 0.10 (0.05) after 6 months and 0.03 (0.03) after 12 months (ANOVA, p < 0.001) (Figure 3).

Changes in mean number of hospitalizations per patient over 12 months. ANOVA, analysis of variance; bsln, baseline; FF/V, fluticasone furoate/vilanterol.
The corresponding mean duration of hospitalization was 0.88 (0.31) days at baseline, 0.08 (0.04) days after 3 months, 0.10 (0.05) days after 6 months and 0.03 (0.03) days after 12 months (ANOVA, p < 0.001) (Figure 4), while the mean duration of inactivity was 3.35 (0.63) days at baseline, 0.60 (0.19) days after 3 months, 1.10 (0.21) days after 6 months and 0.83 (0.39) days after 12 months (ANOVA, p < 0.001) (Figure 5).

Changes in mean duration of hospitalization per patient over 12 months. ANOVA, analysis of variance; bsln, baseline; FF/V, fluticasone furoate/vilanterol.
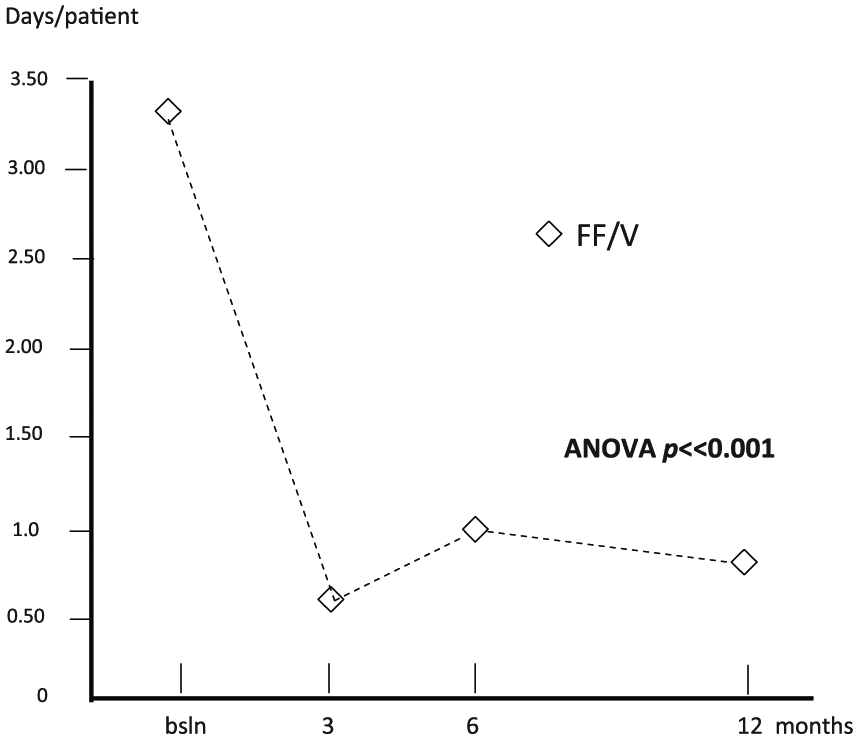
Changes in mean duration of inactivity per patient over 12 months. ANOVA, analysis of variance; bsln, baseline; FF/V, fluticasone furoate/vilanterol.
The mean number of GP visits per patient changed from 1.53 (0.24) at baseline to 0.38 (0.12) after 3 months, 0.55 (0.09) after 6 months and 0.25 (0.06) after 12 months (ANOVA, p < 0.001) (Figure 6), while the mean number of specialist visits per patient changed from 0.70 (0.16) at baseline, to 0.28 (0.07) after 3 months, 0.35 (0.08) after 6 months and 0.23 (0.08) after 12 months (ANOVA, p < 0.009) (Figure 7).
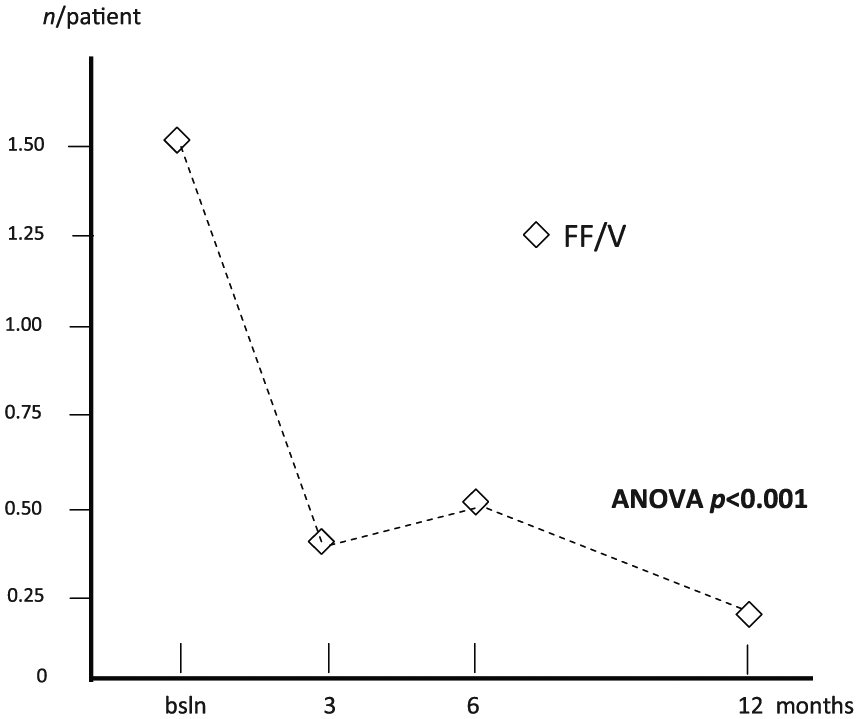
Changes in mean number of general practitioner visits per patient over 12 months. ANOVA, analysis of variance; bsln, baseline; FF/V, fluticasone furoate/vilanterol.

Changes in mean number of specialist visits per patient over 12 months. ANOVA, analysis of variance; bsln, baseline; FF/V, fluticasone furoate/vilanterol.
Finally, the mean number of courses of systemic steroids per patient dropped from 1.08 (0.16) at baseline to 0.33 (0.08) after 3 months, 0.30 (0.08) after 6 months and 0.13 (0.08) after 12 months (ANOVA, p < 0.001) (Figure 8), while the mean number of courses of antibiotics per patient dropped from 1.03 (0.13) at baseline to 0.35 (0.08) after 3 months, 0.33 (0.08) after 6 months and 0.15 (0.08) after 12 months (ANOVA, p < 0.001) (Figure 9).
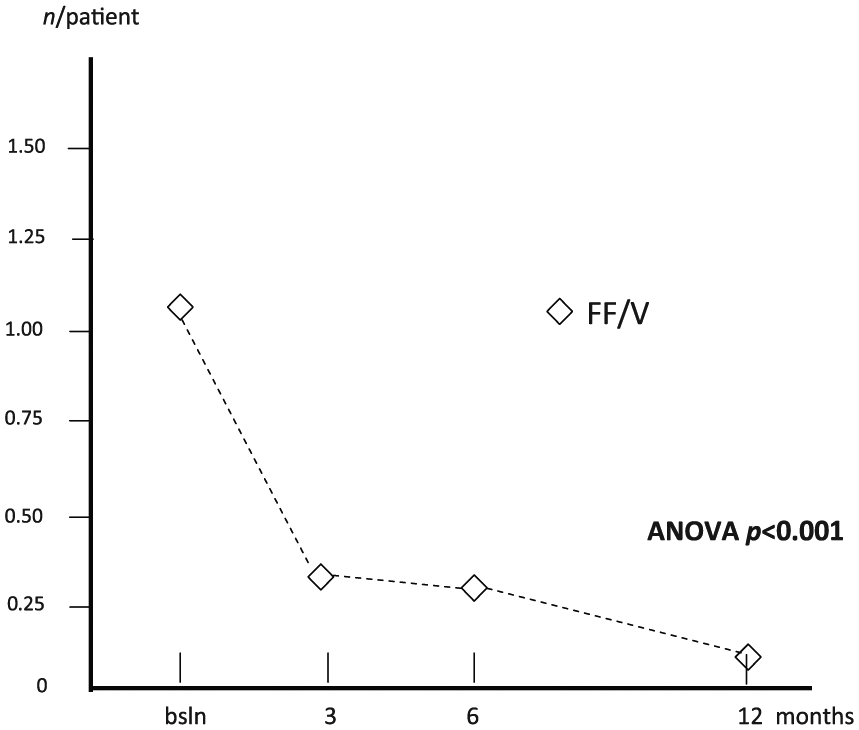
Changes in mean courses of oral steroids per patient over 12 months. ANOVA, analysis of variance; bsln, baseline; FF/V, fluticasone furoate/vilanterol.
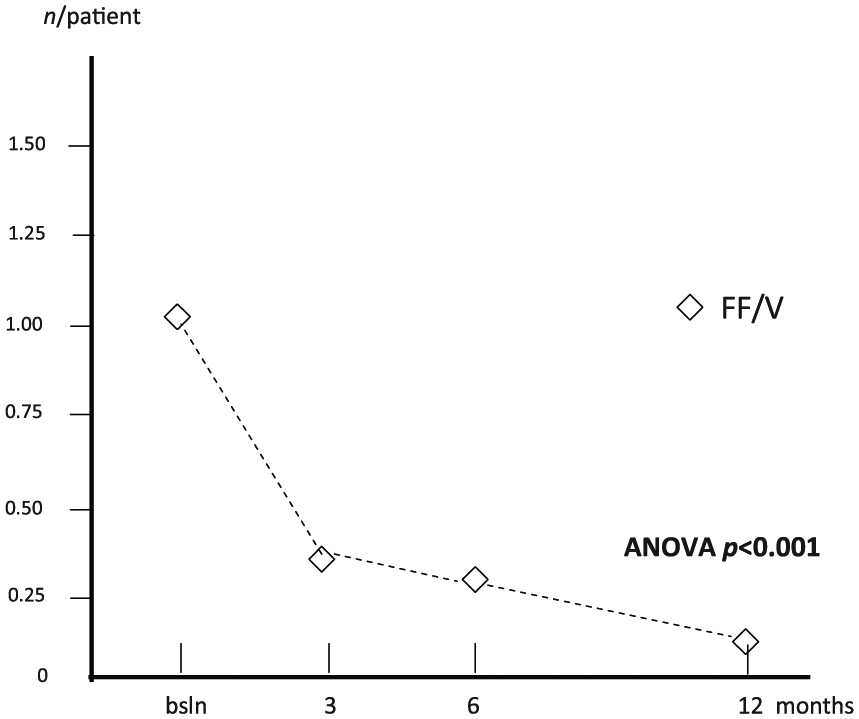
Changes in mean courses of antibiotics per patient over 12 months. ANOVA, analysis of variance; bsln, baseline; FF/V, fluticasone furoate/vilanterol.
The adherence to treatment calculated in terms of expected doses over the period (stemming from the index date) was 93.3% at 3 months, 91.7 at 6 months and 90.6 at 12 months. In other words, an average of 44 doses were skipped (corresponding to 44 days of treatment) over the 12 months of treatment.
No relevant side effects were reported during treatment. Only transient hoarseness in five patients and transient tachycardia in one patient were recorded.
Discussion
A variable extent of airway inflammation usually characterizes bronchial asthma and this biological condition can correspond to a variable degree of airway obstruction. In persistent mild to moderate asthma, the regular use of ICS or ICS/LABA is recommended for preventing the occurrence of asthma relapses, even though several factors can affect the outcomes. Actually, the pharmacological characteristics of the molecules, the frequency of inhalations required over 24 h, the usability of inhaler devices, the patient’s adherence to treatment, the presence of comorbidities, the cost of treatment, and the basic lung function represent substantial variables to take into account.
The present observational, retrospective study was aimed at assessing real life outcomes achievable in patients with mild to moderate asthma receiving FF/V once daily for 12 months. In a previous pharmacoeconomic study, a short-term cost analysis carried out over 12 weeks in mild to moderate asthma suggested the effectiveness of FF/V 99/22 μg once daily via Ellipta. 9 In this study, a significant improvement was achieved in lung function, together with a significant drop in GP and specialist visits, and a substantial reduction in extra medication use, suggesting that good asthma control was achieved in daily life. 9
Moreover, data from the present 12-month study showed a progressive improvement in all outcomes considered according to a time-dependent trend over the study period, particularly during the second 6 months of treatment. In other words, the results for long-term treatment contributed to magnify the extent of FF/V clinical convenience previously assessed during a short-term therapeutic period only. 9 In particular, the dramatic reduction in exacerbation and hospitalization rates, patients’ length of inactivity, GP and specialist visits, and courses of oral steroids and antibiotics strongly supports the substantial and progressive effectiveness achievable with long-term FF/V once daily, and the corresponding good asthma control in real life.
These outcomes can stem from the pharmacokinetics and pharmacodynamics of FF and V.10–12 The corresponding fixed combinations obviously reflect these pharmacological patterns, which also support and provide evidence for their clinical efficacy and effectiveness in clinical terms. In particular, the high selectivity and persistency of steroid receptors which are for FF, together with the high selectivity and persistency of ß2 receptors for V represent crucial aspects.10–12 Actually, these are the peculiarities which mainly confirm the long-lasting therapeutic action of the FF/V combination. 13
Once-daily administration helps to achieve patient adherence during a long-term therapeutic strategy.7,14,15 In the present study, FF/V once daily resulted in very good adherence to treatment over the 12-month observational period (namely, only 44 skipped doses), which likely contributes per se to explain the long-lasting and the time-dependent asthma control achievable with this treatment. Obviously, the easy handling and intuitiveness of the inhalation devices (namely, Ellipta) also contributed significantly to these results.16,17
Hospitalization and exacerbation rates, as well as patients’ absenteeism and medical referrals, represent the main components of asthma annual costs.15–18 The dramatic and progressive drop in these four indices obtained over the 12-month treatment period with FF/V strongly supports and emphasizes the economic convenience of this strategy aimed at the long-term management of mild to moderate asthma.
The main limits of the present study are the relative small number of subjects included and its monocentric design, even though patients belonged to all Italian regions and were anonymously selected. A true strength is the automatic selection of subjects from a unique database. Furthermore, the monthly registration of the number of doses remaining in the device (which is provided with a clear and precise dose counter) rendered the information collected highly reliable in terms of adherence to treatment in real life.
Conclusion
The present study showed that once daily inhalation of FF/V 92/22 µg for 12 months results in time-dependent efficacy in terms of lung function and all the main clinical outcomes in mild to moderate asthma, thus suggesting its long-term economic convenience.
Footnotes
Acknowledgements
R.W. Dal Negro: study design and statistics; P. Turco: checked all clinical data and outcomes; L. Bonadiman: anonymous selections and extraction from the database, data bank construction, and numerical models.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest statement
The authors declare that there is no conflict of interest.