
Abstract
Avoidance of allergens in the treatment of asthma has hitherto not achieved significant benefit despite the strong evidence that allergy both increases severity and contributes to exacerbations of asthma. House dust mite, cat and dog allergens are the most common perennial allergic triggers and most avoidance strategies have focused on reducing exposures in bedrooms. Cochrane reviews have suggested that they neither significantly reduce allergen levels nor improve asthma. While the lack of efficacy may be assumed to be a consequence of exposures occurring outside the bedroom, prolonged sleep is associated with increased susceptibility to bronchospasm and airway inflammation. Thus, if efficient reductions in allergen exposure could be achieved during sleep, it might be expected that this would result in significant improvements in control of asthma. The temperature-controlled laminar airflow (TLA) is a system which can be employed over beds in a domestic environment and results in massive reductions in particulate exposure of recumbent subjects, including highly respirable allergens such as Fel. D1 from cats. Trials of TLA have demonstrated highly significant improvements in asthma quality of life and reductions on airway inflammation as monitored by exhaled nitric oxide levels. Furthermore, in patients with the worst disease, severe exacerbation frequency was significantly reduced. Based on UK health-service costs, the use of TLA falls well below the National Institute for Health and Care Excellence (NICE) threshold for the incremental cost effectiveness ratio (ICER) per quality adjusted life year (QALY). Indeed, for those with frequent exacerbations, it is cost saving and should be prescribed for such allergic asthmatic patients.
Keywords
Historical introduction
Aretaeus, the Cappodocian (2nd century AD), is credited with the earliest documented and recognizable description of asthma ‘. . . cough incessant and laborious; . . . neck swells with the inflation of breath.’ He also observed ‘the evil much worse in sleep’. 1 However, the existence of asthma was likely known in very early history. Seasonal respiratory difficulty was described in ancient Chinese literature 2 from more than 2000 years BC (Huang Di, known as the Yellow Emperor, 2697–2598 BC). The Ebers Papyrus from ancient Egypt (c. 1550 BC) recommended inhalation of smoking herbs for restricted breathing. 3 While Hippocrates is believed to be the first to suggest a relationship between the environment and respiratory problems, he considered disorders of the lung to originate as a consequence of imbalance of the ‘humors’ commencing in the brain. 4 This concept of a psychological cause for asthma has lingered for centuries.
Rhazes described rhinitis occurring in spring when ‘roses give forth their scent’. 5 Similar observations of seasonality and the effect of roses and other flowers triggering asthma attacks appeared over subsequent centuries. However, Charles Harrison Blackley (1820–1900) was the first to conclusively prove that hayfever and seasonal asthma were due to inhalation of pollen by experimentation on his own asthma and rhino-conjunctivitis. 6
In the 12th century, Moses Maimonides a Hebrew philosopher and physician wrote a manual addressed to his asthmatic patient, the son of the Sultan Saladin. He recognized the detrimental effects of extremes of environment including temperature, humidity, the ‘stagnant air of the city’ and emotional disturbance. 2 In 1552, Cardanus, a Pavian physician, successfully treated the asthmatic archbishop of St. Andrews, John Hamilton, in part by prohibiting the use of feather bedding. 2 John Baptista van Helmont, a Flemish physician, is likely the first to suggest dust as a cause of asthma when he wrote of a patient ‘as oft as any place is swept or the wind doth otherwise stir up the dust, he presently falls down being almost choked’. 7 Sir John Floyer, an asthma sufferer himself, also recognized the adverse effects of dust and described the frequent occurrence of nocturnal wheezing attacks. 8
It was not until the 20th century that the importance of house dust as a trigger of asthma was elaborated. Herman Dekker noted the presence of mites in house dust and suggested inhalation of live and dead mites caused attacks. He recommended keeping the bedroom empty and the use of clean bed clothes and hammocks rather than mattresses. 9 Eventually, Voorhorst and colleagues identified that the house dust mite (HDM) (Dermatophagoides Pteronyssinus) was probably the major allergenic component of house dust. 10 This was followed by a flurry of papers confirming the effect of HDM in aggravating asthma in more than 80–85% of cases particularly in childhood. 11
Inhalant allergen avoidance
Dust collected at high altitude in the Alps and Dolomites, where humidity is very low, contains few or no mites. 12 Similarly, dust from beds and floors in hospitals has little mite allergen. Thus, it has been suggested that the improvement in asthma, which occurs during hospital admission 13 or convalescence at high altitude is partly explained by reduced HDM exposure. Indeed, residence at high altitude reduces symptoms, treatment requirements, markers of allergic airway inflammation and levels of HDM IgE antibody- and HDM allergen-induced bronchial hyper-responsiveness. 12 Such observations have created the impetus for trials of HDM avoidance strategies in domestic environments.
Numerous avoidance approaches have been employed including simple hygiene; high efficiency vacuuming;14,15 chemical methods using acaricides; 16 barriers applied to bedding; 17 dehumidification and whole-house ventilation systems. 18 The vast enterprise has sadly not been rewarded by consistently successful outcomes. Consequently, Cochrane reviews with meta-analyses of controlled trials have concluded that such measures not only have limited value in reducing exposures but also confer no benefit for house mite allergic asthma patients. 19 The rider to these observations is that there is considerable heterogeneity between trials and the selection process employed in the systematic reviews, which has been questioned. It has been suggested that as most avoidance studies have focused on the bedroom, the ubiquitous exposure elsewhere in the home and beyond inevitably compromises potential benefits. Perhaps a combination of avoidance strategies will be required as asthma is a multi-factorial disease with diverse triggers including infection, non-specific irritants, cold and dry air. In other words, avoidance of one factor will not improve the disease. As pharmacotherapy is highly effective in controlling asthma for many, though not all patients, guidelines such as those from BTS/SIGN, have become ambivalent in discussing an allergy focus.
Notwithstanding the negativity that is prevalent in medical circles in relation to allergen avoidance, patients and their carers are well aware of the impact of environment on their asthma, and other associated conditions such as eczema and rhinitis. Their expectation from medical consultations is that triggers will be identified and that they will be empowered to take control of their condition including the employment of avoidance strategies. This could be described as ‘a shared misunderstanding’. As we now move into the era where physicians listen to and address the wishes and expectations of their patients, it is incumbent upon us to re-evaluate environmental control.
Allergen exposure
HDM allergen is present in mattress and pillow dust, as well as carpets, curtains, and soft furnishing in most homes in temperate climates,20,21 but tends to only be rendered airborne with disturbance. 22 Pet allergen particles by virtue of mass and size, such as from cat dander, are not only more easily rendered airborne, but are readily transferred between locations carried on the clothing of cat owners. 22 They are also more respirable, penetrating further into the bronchial tree. Cat allergen is transferred from homes to schools on clothing and can, if many children in a class come from cat-containing homes be in sufficient quantities to exacerbate asthma in cat allergic children in the same class.23,24 Pet allergen can often be detected in the air and soft furnishings of nonpet-containing homes. 25 This suggests that pet allergen avoidance will require more extensive environmental intervention than achieved by addressing the bedroom alone.
As has been reported for many centuries, asthma often is at its worst during prolonged sleep. While this might be assumed to be due to HDM allergy, nocturnal asthma is equally common in non-HDM-sensitive individuals. It is likely that many factors contribute to this susceptibility. Intense particulate exposure, worse for those with allergy to dust contents clearly plays a part. However, the diurnal rhythms in both hormonal and immune profiles render the airways more susceptible to bronchospasm and inflammation. Therefore, there remains a priority to attempt to optimize the nocturnal environment of asthma patients.
People spend at least 30% of the day in bed, and are thus in close contact with bedding surfaces. In such situations, the quantity of allergen inhaled will be related to the surface concentration and will be modified by disturbance during turning in bed; head position; and room ventilation. Studies have shown that there are convection currents around a recumbent person’s head which acts like a heat generator, creating a temperature gradient highest around the face (See Figure 1A). Particles, including allergens, are thereby carried from bedding surfaces into the breathing zone. 26 Air filtration units, which clean air in a nondirectional manner, have been used for allergen avoidance. Controlled trials of such units for treating pet allergic asthmatic patients have shown no clinical benefit and actually little effect on airborne pet allergen levels. 27 Laminar airflow systems have been developed to remove airborne particles in the micro-chip industry and in operating theatres. In an uncontrolled study, one bedside device using horizontal laminar airflow was shown to improve rhinitis symptoms and reduce daytime somnolence, although exposures were not measured. 28 Logically, the ideal strategy to affect the direction of convection currents around an individual’s head while in bed is to reverse the temperature gradient while continuing to ensure laminar flow.

A cartoon representation of the direction of convection currents when lying in bed without (A) or with (B) the temperature-controlled laminar airflow device operating. The red arrows indicate the direction in which particles will flow; across the face and therefore breathing zone in A with no TLA and away from the face when TLA is employed.
Temperature-controlled laminar airflow
A device using temperature-controlled laminar airflow (TLA) has now been developed. It controls nocturnal exposure to particles by delivering cooled and filtered air from above the head of the individual with asthma during sleep. The greater density of the cooled air reverses the convection current, which hitherto had been bringing allergen-bearing particles into the breathing zone, and displaces them onto the floor (See Figures 1B). This is demonstrated by the use of the TLA in a smoke-filled room. There is a smoke-free cone around the recumbent subject’s face (See Figure 2).

The temperature-controlled laminar airflow in action in a smoke-filled room demonstrating the particle-free area around the breathing zone of a recumbent subject.
A detailed study of particle and allergen exposure of health subjects lying on heavily cat-allergen-laden bedding demonstrated that TLA achieved massive reductions in both total particle and cat allergen concentrations in the breathing zone. TLA caused >99% reductions in total airborne particles of all sizes with no concomitant changes in concentrations of particles outside the TLA zone of effect. There was an equivalent large reduction in cat allergen particle counts using the TLA device. Most importantly, there was a significant reduction in cat allergen reaching the nasal airway of the subjects as detected in nasal air samplers. Movement of subjects in the bed increased particle and cat allergen exposures, which was not modified by an active TLA device. 29 Nevertheless, based on a simulation of overnight sleeping, the TLA would significantly reduce even highly respirable allergen particles.
Clinical trials
Two double-blind placebo-controlled trials of the use of the TLA in patients’ homes have been completed and published involving, in total, 310 allergic asthmatic subjects. Both studies selected allergic asthmatic patients whose disease control was poor despite regular pharmacotherapy. Thus they added TLA to existing therapy at a time when otherwise escalation of conventional asthma therapy would have been necessary. The first (n = 28 adults) was a crossover trial (10 weeks each on active and placebo) and showed significantly improved asthma quality of life (mini AQLQ) and decreased exhaled nitric oxide as a marker of eosinophilic airway inflammation. 30 The second was a parallel group study for 12 months in 282 subjects: this included adults and children, aged between 7 and 70 years with HDM, cat or dog allergy (the 4A trial) and similarly showed significant improvement in asthma-specific quality of life (mini AQLQ and Paediatric AQLQ) and significantly decreased exhaled nitric oxide. 31 Within this latter trial, there was a progressively greater significance of difference as the severity of asthma increased. This was a consequence of decreasing placebo effect with increasing severity while the benefit on active treatment was sustained. This is unlike any pharmacotherapy for asthma other than omalizumab. A later subanalysis showed a significant reduction in asthma exacerbations using the active TLA in those with the greatest severity of asthma and at least two different aeroallergies 32 (See figure 3). Within the second study, a subgroup of 49 children with significant associated allergic rhinitis completed rhinitis-specific quality of life questionnaires (RQLQ). Compared with placebo, TLA significantly improved the sleep domain of the RQLQ. 33 Similarly in a post hoc analysis, patients with poorly controlled asthma (ACT > 18) despite GINA stage 4 therapy had significant improvements in both symptom and sleep components of the AQLQ (See Figure 4).

Post hoc analysis of 4A trial data showing the effect of temperature-controlled laminar airflow on asthma severe exacerbations. While the trial was not powered to detect differences, in those patients with the most severe disease, there was a significant reduction in exacerbations.
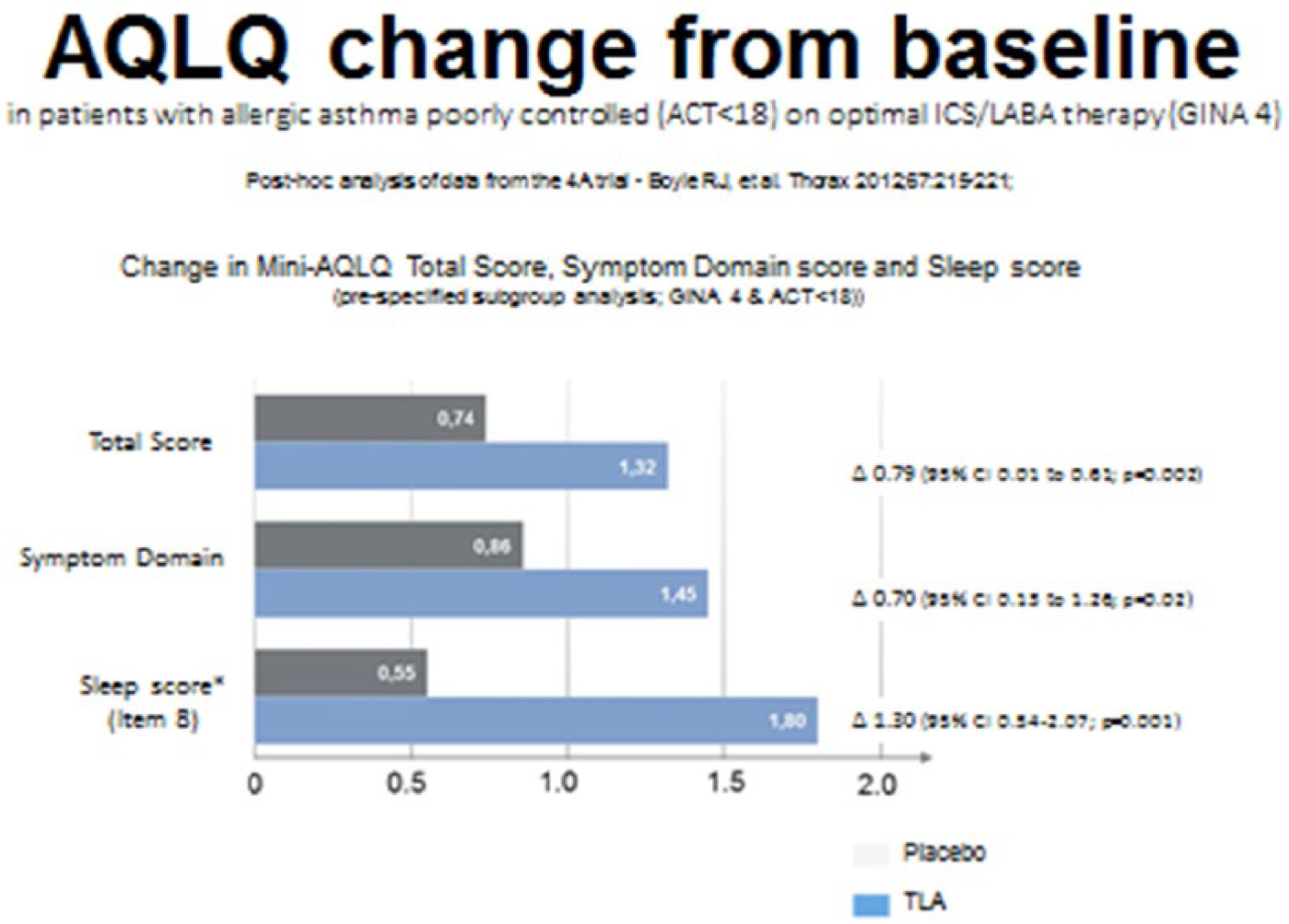
Post hoc analysis of data from the 4A trial demonstrating that the symptom and sleep components of the AQLQ were significantly improved with the use of temperature-controlled laminar airflow in those patients with poor control of asthma despite regular GINA stage 4 treatment.
There have also been a number of open-label observational studies showing similar benefits.
Seven adult allergic asthmatics had significant improvements in mini AQLQ and 22 allergic children had significant improvements in allergic rhinitis. 34 Latterly, interest has focused on eczema as the above studies gave an impression of benefits for this allergic skin disease, but were not specifically powered to detect differences. One observational study of eight cases of severe atopic eczema with aeroallergen sensitization showed significant improvements using TLA. 35
Overall, the trials and observational studies have confirmed that nocturnal rather than daytime exposures are significantly more important in terms of a pervasive adverse effect on asthma control. Not only do physiological factors render individuals more susceptible to exacerbation at night but also the consequent disturbed sleep has profound knock-on effects which compromise intellectual performance, and diurnal endocrine, metabolic and immunological rhythms.
Hitherto, there have been no trials combining TLA with other allergen-avoidance strategies. However, as the Cochrane review of such approaches in isolation has not shown efficacy, 19 it is unlikely that such an approach would gain any additional benefit beyond that achieved by TLA alone.
Health economic evaluation
Based on the above trials, it was apparent that the greatest health/economic benefit was achieved by using TLA in allergic asthmatic subjects who have frequent exacerbations.
The UK direct healthcare costs for asthma are more than £1 billion per year, of which a high percentage is expended to manage the top quartile of severity due to frequent exacerbations and the frequent demands for unscheduled care. Having excluded avoidable and perhaps treatable causes of the high morbidity, currently those with severe persistent allergic asthma are considered for treatment with expensive biologicals such as omalizumab. One additional study, which specifically focused on severe cases has been added to the literature. 36 It was conducted in Germany, as a pre/postobservational study. Patients (n = 30) with moderate-to-severe poorly controlled allergic asthma and frequent exacerbations, despite optimal pharmacological treatment were recruited. They used the TLA for 12 months and progress was compared with the previous 12 months. When comparing the last 12 months pre-TLA with the subsequent 12 months of TLA use, the significant outcomes were: reduced exacerbations; reduced A&E visits and hospital admissions. Finally, there were no Intensive Care admissions after TLA was introduced as compared with 14% during the previous year, though due to small numbers this latter difference was not statistically significant. This study has facilitated a health economic calculation of the use of TLA in patients with recurrent severe asthma exacerbations. By also incorporating the quality-of-life data from the 4A trial, 31 it has been possible to calculate the incremental cost effectiveness ratio (ICER) based on UK health service costs. For patients requiring regular inhaled steroid prophylaxis with continuing poor control, the ICER was £8988 per QALY (quality adjusted life year). This is well within the £20,000 benchmark ratio used by the National Institute for Health and Care Excellence (NICE). The costs, based on asthma severity, ranged from £18,883/QALY for relatively milder cases through to being cost saving for the most severe. As the latter patients might otherwise be considered for treatment with the much more expensive biologicals, employment of TLA could generate significant cost savings while still maintaining quality of life.
Clinical experience
Patients and their families very clearly perceive that asthma is triggered by a host of environmental factors. As such, they expect that clinicians will empower them to take action in avoiding relevant triggers. Failure to address these expectations has the potential to compromise concordance with pharmacotherapy which remains the mainstay of treatment. The disappointing results achieved hitherto by avoidance trials has been the main reason for physician reluctance in the UK to recommend allergen avoidance. By failing to address this unmet desire, patients frequently gravitate to complementary and alternative medicine, which has no proven efficacy (see BTS/SIGN evidence based review of asthma management). In my experience, patients and families welcome allergy testing and recommendation on relevant avoidance strategies. They are consequently more likely to also follow advice on pharmacotherapy. While the standard allergen avoidance advice in relation to HDM allergy is relatively ineffective, with TLA, we now have published evidence of efficacy. Unlike any other trial of treatment for asthma in which I have been involved, families were very keen to be enrolled. We had no difficulty in recruiting the required numbers for the 4A trial. The TLA proved to be very acceptable for the overwhelming majority and use was sustained over long periods, unlike the common lapses in concordance with other treatments. Among those patients with the most severe disease not responding well to inhaled steroids, allergy is a common and important co-morbidity. TLA is a novel management modality which addresses a current unmet need. It not only improves asthma control but simultaneous benefits allergic rhinitis. There is the potential it might also alleviate allergic eczema symptoms. Certainly clinical experience suggests this might be the case. Two trials of TLA are currently in progress in UK. The Laminar Airflow in Severe Asthma for Exacerbation Reduction (LASER) trial with over 200 participants is specifically focused on adult asthmatics with frequent exacerbations. 37 Authors of the second study aim to recruit 15 children with severe allergic eczema to a detailed study of efficacy and particularly, its effect on sleep quality 38 Both studies will add to the accumulating evidence, which I believe will result in the more extensive provision of TLA for patients with severe manifestations due to exposure to inhalant allergens.
Footnotes
Acknowledgements
The author is employed through Imperial College on a grant from the National Institute for Health Research, Collaboration for Leadership in Allied Health Research and Care (NIHR CLAHRC for NW London). The views expressed in this publication are those of the author and not those of the NHS, the NIHR or the Department of Health.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest statement
The author was a member of the Scientific Advisory board designing and over-seeing the conduct of the 4A trial discussed in the paper. He has also given paid lectures at Airsonett sponsored symposia during international medical conferences. However, the paper was written without any influence from the company and represent his views alone.