
Abstract
Chronic inflammation plays a central role in the pathogenesis of chronic obstructive pulmonary disease (COPD). However, there are no effective anti-inflammatory pharmacologic therapies available for COPD so far. Recent evidence suggests that an immunologic mechanism has a role in the pathogenesis of COPD. Macrolides possess anti-inflammatory and immune-modulating effects may be helpful in the treatment of COPD. Several clinical studies have shown that long-term use of macrolides reduces the frequency of COPD exacerbations. However, the subgroups that most effectively respond to long-term treatment of macrolides still need to be determined. The potential adverse events to individuals and the microbial resistance in community populations raises great concern on the long-term use of macrolides. Thus, novel macrolides have anti-inflammatory and immuno-modulating effects, but without antibiotic effects, and are promising as an anti-inflammatory agent for the treatment of COPD. In addition, the combination of macrolides and other anti-inflammatory pharmacologic agents may be a new strategy for the treatment of COPD.
Introduction
Chronic obstructive pulmonary disease (COPD) is associated with enhanced chronic inflammation in the airways and the lung in response to inhaled cigarette smoke and other noxious particles [Global initiative for chronic obstructive lung disease, 2016]. Despite the high morbidity and mortality of COPD (it is projected to be the third-leading cause of death worldwide by 2020), there are no existing therapies that have been shown to effectively prevent the long-term decline in lung function of disease or reduce mortality. The aim of pharmacologic therapy is to reduce COPD symptoms, decrease the frequency and severity of exacerbations, and improve health status and exercise tolerance. The recognition that chronic inflammation plays a central role in the pathogenesis of COPD has led to the widespread use of corticosteroids in the treatment of this disease. However, patients with COPD are poorly responsive to glucocorticoids, even at high doses of inhaled or oral intake, when compared with those with asthma [Barnes, 2003]. Furthermore, treatment with corticosteroids is only recommended for patients with severe and very severe COPD and at high risk of exacerbations in the Global Initiative for Chronic Obstructive Lung Disease (GOLD) 2015 [Global initiative for chronic obstructive lung disease, 2016], indicating the limitation and lagging of traditional anti-inflammatory treatments for COPD. Particularly, there are no anti-inflammatory pharmacologic therapies available in early-stage COPD at present. Thus, it is urgent to identify novel targets and new anti-inflammatory drug therapies for COPD.
There are no effective anti-inflammatory therapies because of the lack of understanding of the cellular and molecular mechanisms associated with the chronic inflammatory processes of COPD. Recently, the observation that an abnormal immune response was involved in the chronic inflammation of COPD suggests that an immunologic mechanism has a role in the pathogenesis of the disease [Cosio et al. 2009]. Thus, some investigators proposed that COPD could be an autoimmune disease triggered by cigarette smoking [Agusti et al. 2003; Taraseviciene-Stewart et al. 2006; Curtis et al. 2007; Lee et al. 2007]. Although there have been reports that using immunoregulators in COPD can decrease the severity and frequency of exacerbations [Collet et al. 1997; Li et al. 2004], relatively little is known about the precise mechanisms involved.
It has long been recognized that 14-membered and 15-membered macrolides possess anti-inflammatory and immune-modulating effects that are independent of their antibiotic activity [Culic et al. 2001; Jaffe and Bush, 2001; Zalewska-Kaszubska and Gorska, 2001; Rubin and Henke, 2004]. The clinical benefits of macrolides in the treatment of diffuse panbronchiolitis encouraged the application of macrolides to a broader range of chronic inflammatory airway diseases such as cystic fibrosis, bronchiectasis and asthma [Nagai et al. 1991; Kudoh et al. 1998; Wolter et al. 2002; Kadota et al. 2003]. Recent literature revealed that the effects of macrolides on preventing COPD exacerbations, but the possible anti-inflammatory mechanisms have not yet been fully elucidated. Here, we review the latest studies regarding long-term macrolide treatment in COPD in order to explore the mechanisms by which macrolides may contribute to the disease and to estimate the clinical benefit and potential harmful effects of these agents.
Macrolides: the benefit from animal models and research in vitro
It has been well established that macrolides exerted anti-inflammatory effects by attenuated mucus secretion and decreased accumulation of neutrophils and macrophages in the airway through reduced production of proinflammatory cytokines, adhesion molecules and chemokines [Kanoh and Rubin, 2010]. New animal experiments show that the administration of erythromycin can alleviate inflammation in the airway, lung parenchyma, and pulmonary vascular system and protect the destruction of alveoli in a smoking murine model of emphysema [Mikura et al. 2011]. Further study revealed that, compared with rats exposed to cigarette smoke, inflammatory cells (e.g. neutrophils, lymphocytes and macrophages) were significantly decreased in bronchoalveolar lavage fluid from those receiving erythromycin. Meanwhile, the matrix metalloproteinases (e.g. MMP-2, MMP-9) and proinflammatory mediators (e.g. tumor necrosis factor-α, interleukin [IL]-6) are also significantly reduced [Zhou et al. 2012]. In vitro, erythromycin can suppress the activation of transcription factor nuclear factor (NF)-κB and activator protein 1 (AP-1) which induced by hydrogen peroxide in human bronchial epithelial cells. [He et al. 2008]. In addition, erythromycin also has a beneficial effect on the pulmonary vascular remodeling in rats exposed to cigarette smoke. Our latest studies showed that a greater number of T-helper (Th)1/T cytotoxic (Tc)1, Th17/Tc17 cells and a fewer number of regulatory T-cells were found in mice exposed to cigarette smoke or patients with COPD, and this imbalance of T-lymphocyte subsets persisted even after cessation of cigarette smoke exposure [Chu et al. 2011; Zhang et al. 2012; Duan et al. 2013]. However, these abnormal immune responses in mice exposed to cigarette smoke were partly corrected by administered erythromycin [Bai et al. 2012]. These observations suggest the immunomodulatory properties of macrolides.
Compared with patients with asthma, even high doses of glucocorticoids exerted limited anti-inflammatory effects on the patients with COPD, suggesting the corticosteroid resistance of COPD [Barnes, 2003]. This phenomenon may be due to a reduction and inactivity of histone deacetylase 2 (HDAC2) as a result of over expression of NF-κB and phosphoinositide 3-kinase (PI3K) which induced by oxidative and nitrative stress [Ito et al. 2005; Adcock and Barnes, 2008; Barnes, 2013]. In previous studies, we have found that erythromycin was able to reverse the corticosteroid resistance through increasing HDAC-2 protein expression which was impaired by cigarette smoke extract (CSE). These changes were associated with the suppression of NF-κB activity in human macrophages in vitro [Li et al. 2012]. Collectively, these data elaborated the possible mechanisms underlying the anti-inflammatory effects and immune-modulating effects of macrolides and suggested a possible clinical application of macrolides in COPD treatment.
Macrolides: recent clinical study on the treatment of COPD
Clinical evidences of erythromycin on the treatment of diffuse panbronchiolitis introduced the applications of macrolides in a variety of inflammatory airway diseases [Crosbie and Woodhead, 2009; Spagnolo et al. 2013]. Exacerbation of COPD is an acute event characterized by a worsening of the patient’s respiratory symptoms and relates to an accelerated rate of decline in lung function [Donaldson et al. 2002], dramatically changing the nature of the course of the disease, leading to significant mortality. COPD exacerbations are associated with increased upper and lower airway and systemic inflammation, which suggests the potential effects of macrolides on preventing the exacerbation of COPD. In fact, several recent clinical studies have shown that long-term use of macrolides reduced the frequency of COPD exacerbations and extended the time to the next event (Table 1). Firstly, Seemungal and colleagues [Seemungal et al. 2008] conducted a single-center, randomized, double-blind, placebo-controlled study, in which they administered erythromycin at 250 mg twice daily to 109 patients with moderate-to-severe COPD over 12 months. They found erythromycin treatment was associated with a significant reduction in exacerbations in patients with COPD but there were no statistically differences between the groups in terms of forced expiratory volume in 1 second (FEV1), sputum IL-6, IL-8, myeloperoxidase, serum C-reactive protein, or serum IL-6. Subsequently, He and colleagues confirmed Seemungal’s findings by performing 6 months’ treatment with erythromycin (125 mg, 3 times/day) in 35 COPD patients [He et al. 2010]. The outcome showed not only a reduction in exacerbations in COPD patients who received erythromycin but that this was linked to a decrease in airway inflammation, as shown by a decreased number of neutrophils and neutrophil elastase in the sputum. Since neutrophils are the major inflammatory cell in the airways of patients with COPD, the decrease of neutrophils and neutrophil activity in sputum may be partly responsible for the clinical beneficial effects in patients receiving erythromycin. Pomares and colleagues next investigated the clinical benefits of long-term azithromycin treatment (500 mg, 3 times/week) over 12 months in patients with severe COPD and at least four acute exacerbations per year [Pomares et al. 2011]. Their results revealed that azithromycin therapy significantly decreased the number of acute exacerbations of COPD (2.8 ± 2.5 versus 6.8 ± 2.8, p, 0.001), hospitalizations, and cumulative annual days of hospital stay. In a large, randomized, double-blind, multicenter, parallel controlled study, Albert and colleagues reported that the addition of azithromycin (250 mg daily) for 1 year with standard therapy in COPD patients who had an increased risk of exacerbations was associated with a 27% decrease in the frequency of exacerbations per patient-year and an increase in the median time to exacerbation (266 days in azithromycin group versus 174 days in placebo group) [Albert et al. 2011]. Moreover, the decrease of exacerbations was accompanied by an improvement of the quality of life, as observed in the participants receiving azithromycin who had better scores on the St. George’s Respiratory Questionnaire. More recently, Uzun and colleagues performed a trial aimed to assess maintenance azithromycin use in patients with COPD who had received treatment for three or more exacerbations in the previous year [Uzun et al. 2014]. The observation revealed that the patients that received azithromycin 500 mg three times a week for 12 months resulted in a significant reduction in the exacerbation rate compared with those that received placebo. The exacerbation rate per patient per year was 1.94 for the azithromycin group versus 3.22 for the placebo group [0.58, 95% confidence interval (CI), 0.42–0.79; p = 0.001], and increased the median time to first exacerbation [130 days (95% CI, 28–232) versus 59 days (95% CI, 31–87); p = 0.001]. These findings are in agreement with results from a meta-analysis presented by Yao and colleagues, which showed that macrolide therapy was effective and well tolerated, decreasing the frequency of exacerbations in patients with COPD, and a significant benefit was achieved only when therapy lasts >6 months [Yao et al. 2013].
Summary of random-control studies evaluating the clinical effectiveness of macrolide therapy in COPD.

COPD, chronic obstructive pulmonary disease; ICS, inhaled corticosteroid.
Questions raised from macrolide treatment of COPD
Some patients with COPD are prone to suffer frequent and severe exacerbations while other patients are not. This subgroup of patients are now recognized as having a distinct and important phenotype of COPD [Han et al. 2010]. Results from the studies of Albert and colleagues and Uzun and colleagues demonstrated that the maintenance of azithromycin treatment showed the most benefit in patients with COPD who exhibited the phenotype for frequent exacerbations. This observation raised the question of the kind of patients with COPD that are more likely to benefit from the use of long-term macrolide therapy [Albert et al. 2011; Uzun et al. 2014]. Consequently, Han and colleagues [Han et al. 2014] carried out a secondary analysis of this large randomized trial to identify the subgroups to most effectively respond to long-term treatment of azithromycin. They noted that azithromycin is more effective in older patients and patients ranked in milder GOLD stages, especially in those requiring both antibiotic and steroid treatment, but there was no difference in efficacy by sex, history of chronic bronchitis, oxygen use, or concomitant COPD therapy. The relatively little effect among current smokers suggested that azithromycin should be cautiously administrated in this subpopulation. Interestingly, their results demonstrated an increased treatment response for patients at milder GOLD stages. Since this subpopulation accounts for a large part of COPD, this finding may provide evidence for pharmacological intervention with macrolides in the early stages of COPD. In COPD patients with stable neutrophilic bronchitis, Simpson and colleagues found that the addition of azithromycin 250 mg daily for 12 weeks to standard respiratory medications resulted in a trend for a reduction of severe exacerbations experienced and in the markers of neutrophilic airway inflammation [Simpson et al. 2014]. Even though the causal relationship between the anti-exacerbation effect of azithromycin on COPD and an anti-neutrophilic mechanism was unverified, it is reasonable to conclude that the patients with stable neutrophilic bronchitis would be the subgroup which would benefit from the long-term macrolide therapy.
Bronchiectasis coexisting in patients with COPD is identified with increasing use of computed tomography in the assessment of patients with COPD. This radiological change is associated with longer exacerbations and increased mortality, which suggests the clinical importance of coexisting bronchiectasis in COPD [Patel et al. 2004; Martinez-Garcia et al. 2013]. Although the treatment strategies recommended in GOLD 2015 are the usual COPD therapies combined with conventional lines for bronchiectasis [Global initiative for chronic obstructive lung disease, 2016], there are still controversies in the best regimen and lack of pharmacologic agents for this subpopulation of COPD. A growing body of evidence has shown the clinical beneficial effects of long-term macrolide therapy on non-CF bronchiectasis patients. The latest evidence from three randomized, double-blind, placebo-controlled trials, which demonstrated significant reductions on pulmonary exacerbations and better quality of life among non-CF bronchiectasis patients treated with long-term, low-dose macrolide therapy (azithromycin or erythromycin), further confirmed the notion that macrolide maintenance treatment provided clinical benefit in non-CF bronchiectasis [Wong et al. 2012; Altenburg et al. 2013; Serisier et al. 2013]. Therefore, patients with COPD coexisting with bronchiectasis might be a potential population to benefit from maintenance macrolide therapy. Nevertheless, the most suitable population for long-term macrolide treatment and the time the agent should be administered remains uncertain.
It seems that maintenance treatment with erythromycin, azithromycin and clarithromycin all achieved clinical benefits in patients with COPD, so a question remains on the kind of macrolides that should be prescribed. Over the past decades, the progressive introduction of long-acting macrolides, particularly azithromycin, but also clarithromycin, resulted in substantial and sustained increases in macrolide resistance in the community [Karlowsky et al. 2009; Serisier, 2013]. Although erythromycin is the only drug isolated from nature, and has long been used in the treatment for diffuse panbronchiolitis (DPB), it seems to be better tolerated and displays a lower risk of induction of macrolide resistance than azithromycin and other macrolides. In light of this, erythromycin may be a more appropriate and responsible alternative than azithromycin or clarithromycin for patients with COPD.
Concerns about long-term use of macrolides
Despite the beneficial effects of reducing exacerbation of COPD, an agreement on the concerns about the potential adverse events of long-term macrolide use in COPD has not been reached. The common adverse effects in long-term use of macrolides included gastrointestinal intolerance, impairment of liver function and hearing impairment. Uzun and colleagues reported that approximately one-fifth of patients in the azithromycin group complained of diarrhea [Uzun et al. 2014]. Compared with those receiving placebo, a higher rate of hearing impairment in participants receiving azithromycin was found in the study by Albert and colleagues (25% versus 20%) [Albert et al. 2011]. A great concern to individuals rises from the potential cardiovascular toxicity in chronic use of macrolides. There is accumulating evidence that macrolides can cause potential proarrhythmic effects, including QT-interval prolongation, torsades de pointes and polymorphic ventricular tachycardia which closely related to cardiovascular death. These arrhythmia-related adverse cardiac effects of macrolides are more likely to occur in patients with other coexisting cardiac risk factors such as resting tachycardia, prolongation of the QTc interval, hypokalemia or hypomagnesemia or in patients taking some antiarrhythmic agents concomitantly. Ray and colleagues reported their findings in an observational retrospective study which revealed that when compared with amoxicillin or ciprofloxacin, there was an increased risk of cardiovascular death during 5 days of azithromycin therapy [Ray et al. 2012]. The risk of cardiovascular death was most pronounced among patients at a high baseline risk of cardiovascular disease. In a nationwide historical cohort study involving adults 18–64 years of age, Svanstrom and colleagues did not find that azithromycin use was associated with an increased risk of death from cardiovascular causes, as compared with penicillin V [Svanstrom et al. 2013]. Since the young and middle-aged adults have less opportunity for coexisting cardiovascular risk factors, this observation may raise the risk of prescribing macrolides to older patients. In another large retrospective, cohort study, to assess the association of azithromycin use with mortality and cardiovascular events in older patients hospitalized with pneumonia, Mortensen and colleagues compared patients (⩾65 years) receiving azithromycin therapy with patients receiving another antibiotic therapy between 2002–2012 [Mortensen et al. 2014]. Their results revealed that treatment with azithromycin in older patients was associated with a lower risk of 90-day mortality when compared with those who received other antibiotics. However, a small but significant increase in the odds of myocardial infarction was observed in patients receiving azithromycin therapy, but not any other cardiac event, cardiac arrhythmias or heart failure. Overall, it seems that there was a cost to be paid in exchange for a clinical beneficial of the maintenance macrolide treatment. Thus, it is critical to identify patients in whom the benefits outweigh risks for the long-term macrolide therapy and to monitor electrocardiographs at the time of the initiation of macrolide therapy and at appropriate intervals thereafter, to exclude the presence of QTc prolongation.
The greatest concern regarding the wide use of maintenance macrolide therapy in COPD is microbial resistance in community populations [Serisier, 2013]. There is little information available on the clinical consequences of macrolide resistance to individuals. In the study by Albert and colleagues, they found the rate of nasopharyngeal colonization with pathogens resistant to macrolides was 81% in the azithromycin group during the course of the study when they were not colonized with selected respiratory pathogens at the time of enrollment [Albert et al. 2011]. This was twice as high as the placebo group (41%). Similarly, long-term, low-dose macrolide therapy significantly increased the proportion of macrolide-resistant respiratory pathogens in non-CF bronchiectasis patients [Wong et al. 2012; Altenburg et al. 2013; Serisier et al. 2013]. Given the greater patient population of COPD, the maintain use of macrolide treatment in this population may greatly affect population macrolide resistance in the community.
Promising macrolide treatments for COPD
To overcome the potential effect of traditional long-term macrolide therapy on the development of antimicrobial resistance in the community, several novel macrolides, which have anti-inflammatory and immuno-modulating effects but without antibiotic effects, are under development (Table 2). A novel class of nonantibiotic 14-membered macrolide derivatives of azithromycin with anti-inflammatory and immune-modulatory effects, CSY0073, was reported to correct the inflammation-driven immune dysfunction in models of inflammatory bowel diseases and arthritis [Mencarelli et al. 2011]. Furthermore, CSY0073 also can attenuate lung inflammation induced by lipopolysaccharide challenge in mice. Balloy and colleagues reported that CSY0073 diminished the production of proinflammatory cytokines by macrophages exposed to Pseudomonas aeruginosa LPS [Balloy et al. 2013]. EM703 is another new agent related to a 12-membered macrolide-derivative of erythromycin that also possess anti-inflammatory properties but without antibacterial effect. It has been found that EM703 suppressed the activation of NF-κB and the production of IL-8 in human bronchial epithelial cell induced by diesel exhaust particles [Li et al. 2013]. Solithromycin (SOL; CEM-101) is a novel macrolide fluoro ketolide, that not only exhibits a greater antimicrobial activity but also displays superior anti-inflammatory profiles compared with other macrolides currently used. It is able to restore corticosteroid sensitivity by inhibition of PI3K signaling under oxidative stress [Kobayashi et al. 2013]. More recently, another novel 12-membered nonantibiotic macrolide EM900 has been shown to inhibit rhinovirus (RV) infection by reducing the ICAM-1 levels and the number of acidic endosomes, therefore modulate the airway inflammation associated with RV infections [Lusamba Kalonji et al. 2015]. Considering RV is the major cause of COPD exacerbation [Hewitt et al. 2016], EM900 could be a candidate drug for the prevention of COPD exacerbation. In addition, EM900 has been documented to exert direct inhibitory effects on mucus secretion from airway epithelial cells [Tojima et al. 2015]. Furthermore, EM900 derivatives (e.g. EM939) significantly attenuated lung and alveolar inflations, functionally and histologically in a cigarette-smoking guinea pig model [Sugawara et al. 2016]. These findings collectively indicated that these novel macrolides hold great promise for the treatment of COPD in the future, while maintaining the benefits of macrolide use without increasing the risk of antimicrobial resistance.
Candidates of novel macrolides for the treatment of COPD.
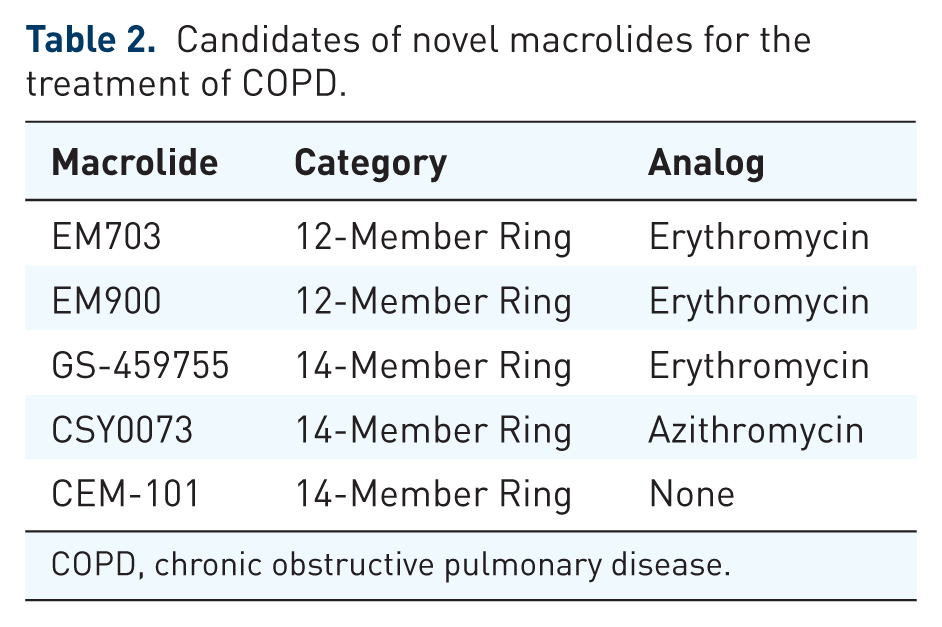
COPD, chronic obstructive pulmonary disease.
In view of the special anti-inflammatory properties of macrolides, the combination of macrolides and other anti-inflammatory pharmacologic agents may be a new strategy for the treatment of COPD. Recently, our study demonstrated that the combination of erythromycin and dexamethasone improved corticosteroid sensitivity through inhibiting the PI3K-δ/Akt pathway and enhancing glucocorticoid receptor α expression. Furthermore, the combination of erythromycin and dexamethasone markedly reduced the production of IL-8 by peripheral blood mononuclear cells of COPD patients and U937 cells exposed to CSE [Sun et al. 2015]. Therefore, combining macrolides with corticosteroids might enhance the anti-inflammatory effects of steroids in the treatment of COPD.
In addition to the direct anti-inflammatory activities, macrolides have the potential to influence the adaptive immune response by modulating the function of many immune cells. Our latest study found that under the stimulation of CSE, erythromycin dramatically down-regulated the expression of the co-stimulatory molecule CD40 on dendritic cells in vitro, thus inhibiting the differentiation of Th17 cells induced by dendritic cells (data unpublished). Given dendritic cells play a critical role in the initiation of an adaptive immune response, this finding may helpful in understanding the immunomodulatory mechanisms of macrolides and may open a new window for the treatment of COPD in the future.
Conclusion
Evidence from in vivo and in vitro studies and large-scale multicenter clinical research confirmed the unique anti-inflammatory effects and clinical benefit of maintenance macrolide use in the treatment of COPD. However, the precise mechanism of how macrolides prevent the acute exacerbations of COPD are not fully understand and it still needs to be determined which subgroups of COPD are likely to derive the greatest benefit from this therapy. Furthermore, compared with the wide use of long-acting β agonists and long-acting antimuscarinic agents with or without inhaled corticosteroids, a consensus has not yet been achieved on the long-term use of macrolides for patients with COPD. Further long-term, large-scale, multicenter clinical studies would be required to further evaluate the risks and clinical effectiveness of maintenance macrolide use in the management of COPD.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest statement
The authors declare that there is no conflict of interest.