
Abstract
Objective:
The objective of this study was to share our experience in the management of congenital tracheal stenosis (CTS) using self-expanding intraluminal stents in infants.
Methods:
From January 2010 to August 2012, 31 infants with CTS treated using stents by bronchoscope in pediatric intensive care units (PICUs) were recruited for this study.
Results:
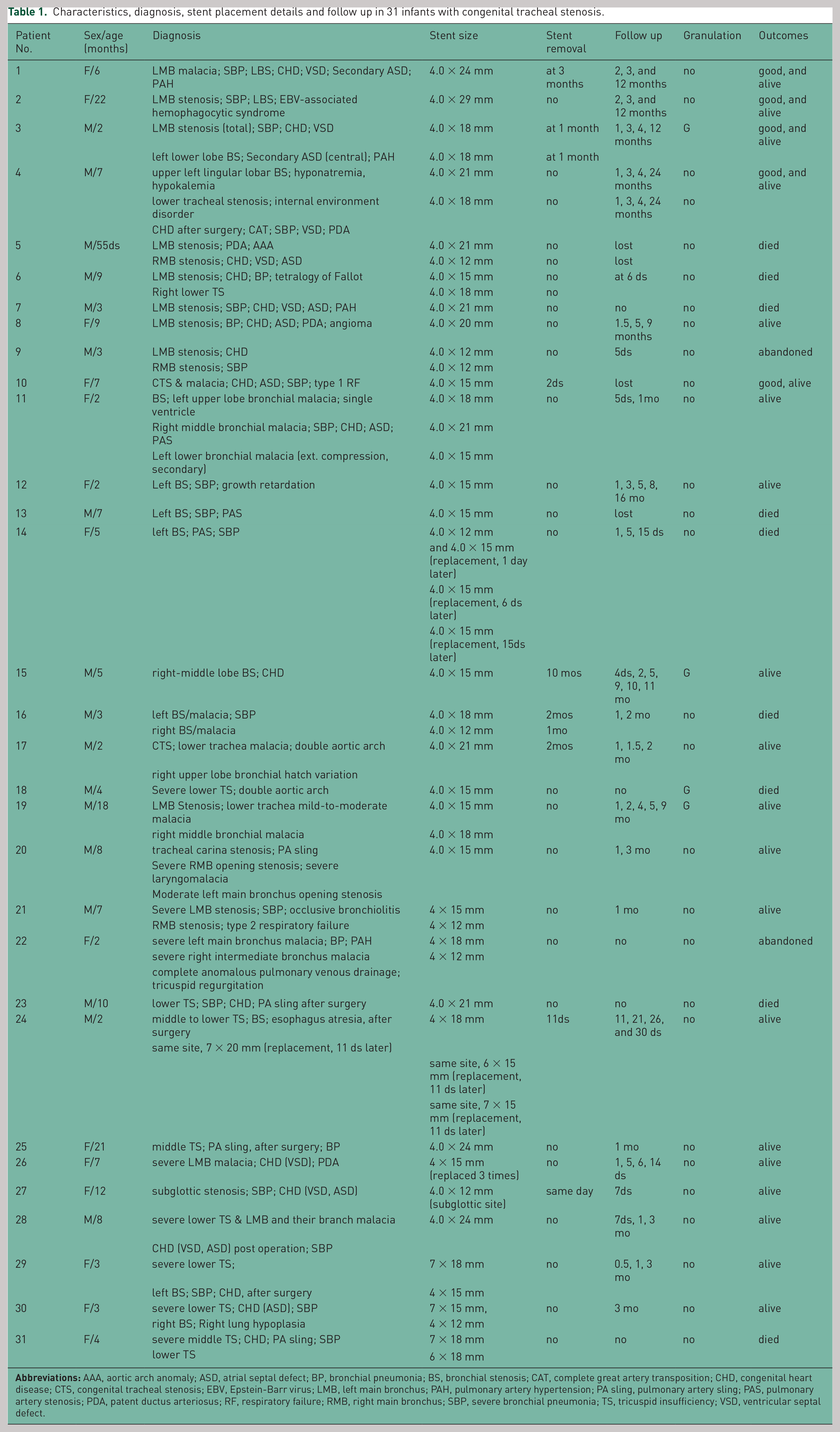
Among the 31 patients, 17 were male and 14 were female with their ages ranging from 55 days to 22 months. CTS was associated with congenital heart disease (CHD) in 22 patients. There were no immediate stent-related airway complications. A significant and immediate improvement of respiratory obstruction following stent placement in all 31 patients led to successful weaning from the breathing machine and extubation. Granulation tissue formation as a complication was observed in three (9.7%) patients, but all were successfully managed using cryotherapy. During follow up (up to 24 months), stents in 29 infants remained functional. In seven cases, stents were retrieved under bronchoscope (the same day to 10 months), and three cases required stent replacement (each of the three cases had the stent replaced three times). Nine infants died after stenting due to other causes and two infants abandoned treatment.
Conclusion:
Airway stenting may provide an important therapeutic option in infants with CTS.
Introduction
Congenital tracheal stenosis (CTS) and tracheomalacia occur in children, infants in particular, and they are frequently associated with quite severe symptoms that require mechanical ventilation. CTS is an innate narrowing of the trachea causing airway obstruction. This condition is common in children in pediatric intensive care units (PICUs), but, in such occurrences, it presents particularly difficult problems in the PICU and clinical management is difficult and challenging [Yu et al. 2011]. It is important to explore the diagnostic and therapeutic methods for perioperative children with congenital heart disease (CHD) with airway stenosis in PICUs.
Tracheal stenosis in children is mostly congenital and relates to the presence of complete tracheal rings. The extent of the stenosis ranges from the involvement of the localized segment to the entire trachea or bronchus, and may even extend to the proximal bronchi. Evaluation may often be delayed as symptoms are frequently attributed to asthma. Tracheal and bronchial malacia in infants is sometimes caused by external pressure from adjacent abnormally-located vessels or by enlarged vessels in conditions such as tetralogy of Fallot without a pulmonary valve. Hence, evaluation of airway obstruction should include electrocardiography (ECG) and imaging, such as computerized tomography (CT) or magnetic resonance imaging (MRI). Airway stenting may relieve extrinsic compression in CTS children, and stents may also be indicated in the setting of tracheomalacia after airway reconstruction [Phipps et al. 2006].
A variety of techniques have been attempted to relieve airway obstruction. Surgical intervention may present a high reoperational rate for residual stenosis and mortality from later airway complications. Hence, the approach has shifted from surgical intervention to balloon expanding intraluminal stents. Flexible fiberoptic bronchoscopy (FFB) in infants not only helps in evaluation of airway obstruction, particularly anatomic airway lesions, but also aids in precise stent placement for children with tracheal stenosis. In the current study, we utilized balloon dilatation and the expandable metallic airway stent placement via FFB as a therapeutic option in infants with airway stenosis, including those associated with CHD. We aimed to explore the benefit of endoluminal stenting in the management of tracheobronchial stenosis in infants with CHD and assessed their outcome in pediatric patients.
Materials and Methods
From January 2010 to August 2012, 31 patients who underwent endoluminal stent placement at Bayi Children’s Hospital (Beijing, China) were enrolled in this study. Informed consent from the infant’s parents was obtained in all cases. All patients had respiratory distress during the newborn period or in early infancy and required ventilatory support before stenting. A total of 22 infants had CHD. The diagnosis of severe tracheal or bronchial stenosis was confirmed by bronchoscopy combined with CT. Balloon-expandable metallic angioplasty rapamycin-coated stents (Partner, Beijing, China) were used for endoluminal stenting. The stents were made of stainless steel mesh and were readily available in different sizes. The stent length was based on the measured length of the narrowed tracheal or bronchial segment, and the stent diameter was chosen by reference of the diameter of the adjacent normal trachea or bronchus. All stents were placed through a 2.8 mm bronchoscope (Olympus BF-XP260F or BF-XP60, Olympus Optical Co Ltd, Tokyo, Japan) with a 1.2 mm working channel, positioned in the airway segment, and expanded (Table 1). Balloon expansion was achieved with a standard angioplasty syringe equipped with a pressure gauge. A pressure of 18–22 atm was applied to inflate the balloon and stent. The actual length of the stent was ensured to be longer than the stenosis site by at least 0.5 cm above and below. The position and expandability of the stent were observed on the display screen. Bronchoscopic examination under direct vision was conducted immediately after stent placement to confirm the proper location of the stent. All infants underwent conventional chest radiography 1–3 days after stent placement to verify the expansion status and position of the stent. Physical examination, blood gas analysis, chest radiography and bronchoscopy were performed again 1 week after the stent placement and patients were followed up once a month thereafter for 24 months. Clinical success was defined as weaning from the ventilator, airway extubation or improvement of dyspnea after stent placement.
Characteristics, diagnosis, stent placement details and follow up in 31 infants with congenital tracheal stenosis.
The main complication associated with the use of the balloon-expandable stents was granulation tissue formation. Granulation tissue has to be removed from the target area by bronchoscopic cryotherapy, which use carbon dioxide freezing treatment, freezing the probe head on the metal surface to promote granulation tissue, and rapidly produce ice hockey probe and its adhesion to tissue removed.
The stents were retrieved through the fiberoptic bronchoscope with pliers (Olympus Optical Company Ltd, FB52C-1, 1050 mm length, 2 mm diameter) under multifunctional ECG monitoring and oxygen administration through a nasal catheter. To the area of stent placement, 1 ml of adrenaline (1:10,000) was sprayed through a transcatheter of the fiberoptic bronchoscope, and the child was closely observed for the presence of a cough and quantity of blood in the phlegm. In cases of repeated bleeding, local spraying of adrenaline was repeated to achieve hemostatic control.
Results
Among the 31 patients who underwent endoluminal stenting, 17 were male and 14 were female, with ages ranging from 55 days to 22 months. A total of 22 patients had associated CHD for which they were receiving surgical correction. The location of stenosis and the sites of stent placement are shown in Table 1. In all cases, following stent placement, the patients’ breathing machine modes could be changed to pressure support ventilation (PSV: 10 cm H2O) and continuous positive airway pressure (CPAP: 5 cm H2O, FiO2 < 40%), and then they could successfully be extubated. There were no symptoms of respiratory distress, tachypnea or tachycardia and blood gas parameters were normal.
A total of 15 of the 31 infants were placed with one stent, while 12 required two stents simultaneously, 1 infant needed three stents simultaneously, and 3 infants required three stent replacements after the initial stent placement. Stents have been placed for the longest time of 24 months without severe complications.
Immediate improvement of respiratory airway obstruction was observed in all 31 infants after stent placement. Further follow up was performed from 3.2 to 24 months. There were no severe complications associated with placement of the stents. Granulation tissue formation over the stent placement was noticed in three infants, but they all could be managed by scraping or cryotherapy. A total of 20 patients were alive with their airway stents in place at 3.2–24 months, while two patients abandoned stent treatment and nine died of heart or infectious diseases during follow up.
The stent was successfully and safely retrieved through FFB in seven patients who never manifested dyspnea on exertion, and no complications occurred during or after stent retrieval (Table 1).
Discussion
CTS is an uncommon disease, occurring mostly in children, and is often associated with CHD. Long segment tracheal stenosis occurs mostly in infants and often manifests with severe symptoms. Tracheal stenosis and tracheomalacia in children are difficult to manage; however, a variety of surgical options are available and the final choice depends mostly on the pediatrician’s preference and clinical experience [Myer et al. 1994; Jaquiss, 2004; Speggiorin et al. 2011]. For nearly 40 years, FFB has been used in the clinical investigation of pediatric airway disorders as a minimally invasive technique. FFB examination is intuitive, not limited by patient’s anatomical space, and can be implemented at the bedside. FFB can find early airway stenosis, and has become the preferred means for the management of tracheal stenosis in recent years [Maeda et al. 2001; Elliott et al. 2003; Loukanov et al. 2005; Xu et al. 2012]. A chest CT scan and three-dimensional reconstructions combined with FFB examination can usually identify airway stenosis.
Patients with severe airway stenosis require rapid balloon expansion and stenting to quickly relieve their symptoms. FFB not only identifies the location and extent of the tracheal or bronchial stenosis and malacia, but can also perform balloon expansion and stenting, thereby reducing morbidity and mortality of the airway obstruction associated with CHD. In this study, we placed balloon-expandable stents in 31 cases and followed them up. The main complication, granulation tissue formation, was observed in three infants which were successfully managed with cryotherapy.
If an airway obstruction in infants with CHD undergoing surgical intervention is not resolved simultaneously, the majority of such children will remain dependent on a breathing machine as long as 7 days [Elliott et al. 2003; Loukanov et al. 2005]. In this study, we carried out radical surgical intervention for CHD and attempted to withdraw patients from the breathing machine, but it was unsuccessful due to associated airway obstruction in 22 patients. The airway obstruction in these patients was identified by FFB and treated with stenting, after which they were successfully extubated. If the surgery for tracheal stenosis is performed prior to cardiac surgery, the success rate is very low due to serious hypoxemia caused by CHD, chronic cardiac insufficiency, and pulmonary hypertension, all of which will seriously affect the postoperative healing of trachea or bronchus. In many cases, failure to wean from mechanical ventilation following surgery for CHD is related to the surgery itself, cardiac dysfunction, diaphragmatic paralysis, and respiratory infections [Hasaniya et al. 2006; Li et al. 2010]. The present study indicated that severe airway stenosis is one of the main reasons for such failure, which is rectifiable with airway stenting.
FFB has emerged as the golden diagnostic modality for airway diseases, such as tracheal or bronchial obstruction, in recent years [Davis et al. 2004]. As airway anomalies in children with CHD are increasingly being diagnosed [Peng et al. 2011], it seems essential to perform preoperative or postoperative evaluation of airway obstruction by FFB in this patient population. Simultaneous identification of concurrent airway anomalies and stent placement through FFB can improve the postoperative survival rate of children with CHD [Airway Reconstruction, 2005; Tibballs et al. 2007]. The main clinical benefits of stenting include improvement in ventilator weaning parameters, reduction in intubation time, and reduced length of hospital stay. Compared to conventional surgery, stent placement can reduce the period of foreign body sensation in the airway and reduce airway complications such as bleeding, infection, and restenosis. Presently, the stent placement technique, timing of stent placement in the airway, and the stenting indications are not well explored.
In our study, we retrieved stents in seven cases after stent placement. In these cases, the removed stents had good shape and completeness, the ventilatory function of the patient was unaffected, and there were no stent retrieval-related complications. These results show that the use of stents in the treatment of airway stenosis in children is well tolerated, reliable, and less invasive; the stents can be placed and taken out whenever necessary. However, the skilled operative technique, the tacit understanding of the operation, and intraoperative nursing as well as close observation in the postoperative period are essential to ensure safe stent placement.
We have previously reported our experience with FFB in assessing CHD-associated tracheal stenosis in children [Elliott et al. 2003]. Metallic expandable-airway stents may be hard to remove endoscopically if the maximal dilated diameter is inadequate. In such cases, thoracotomy with tracheotomy may be necessary and early removal before the incorporation of the stent into the airway wall is optimal. Based on our experience and literature review, we summarize the main viewpoints for the stent retrieval and removal as follows: (1) The stent has been in place for 2–3 months under a good follow-up program; (2) the airway remains unobstructed as confirmed by fiber bronchoscopy and CT imaging examination with 3D-airway reconstruction showing no granulation tissue; (3) absence of dyspnea and airway or pulmonary infection, blood gas analysis showing no ventilation dysfunction, normal X-ray and ECG examinations; (4) tracheal stent clearly seen under bronchoscopy and no epithelialization in the entire open bracket in the airway surface; and (5) the stent could be placed by pulling gently up and down under bronchoscopy. The retrieval of a placed stent may be necessary for infants with CTS.
The long-term effectiveness of balloon-expandable metallic stents in infants is still unknown at this time. Metallic stents have been reported to be well in place for a mean period of 12 years (range: 6 months to 13 years) in four children after insertion without complications [Nicolai, 2008]. The long-term effect of balloon-expandable metallic stents in infants needs to be studied further. FFB is a safe interventional tool in the management of CTS in children with CHD. The long-term effects of FFB-directed stents are not predictable and need to be explored further.
Conclusions
Airway stenting under fiberoptic bronchoscopy may provide an important therapeutic option for CTS in children. This method would be preferred in relieving airway obstruction in CTS associated with CHD, and is proven safe and effective. Expandable metallic airway stents can be left in place as long as 24 months to relieve the airway obstruction. Formation of granulation tissue after stent placement is a treatable complication.
Footnotes
Acknowledgements
We would like to thank the colleagues in the department who participated in and supported this study.
Funding
This work was supported by the National Science and Technology Projects in the 12th Five-year of China (grant number 2012BAI04B01).
Conflict of interest statement
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.