
Abstract
Introduction:
Bodily isomerism, or heterotaxy is a unique entity on which there is mirror imagery in various organ systems, leading to a deviation from the normal lateral arrangements of the viscera. Adults with such isomerism and associated congenital malformations of the heart are now reaching adulthood and developing long-term complications. This study investigates the prevalence and characteristics of pulmonary hypertension in adults with isomerism.
Methods:
The 2012 iteration of the Nationwide Inpatient Sample was utilized and patients were identified as having or not having bodily isomerism and having or not having pulmonary hypertension. Univariate analysis utilizing Chi-square tabulation was done to assess characteristics associated with pulmonary hypertension. Next, a multivariate analysis was done on all patients to identify predictors of pulmonary hypertension followed by a multivariate analysis of patients with only isomerism to identify predictors of pulmonary hypertension specific to this subset.
Results:
A total of 6,907,109 admissions were included in the analysis. Of these, 861 had isomerism (0.01%). Of those with isomerism, 5.6% were found to have pulmonary hypertension. When all patients were included in the multivariate analysis, isomerism was found to be an independent risk factor for pulmonary hypertension with an odds ratio of approximately 1.79. When only patients with isomerism were included in the multivariate analysis, advanced age, obesity, and history of anomalous pulmonary venous connection were independent risk factors of pulmonary hypertension.
Conclusion:
Pulmonary hypertension is more common in those with isomerism, with isomerism being an independent risk factor for pulmonary hypertension. The prevalence of pulmonary hypertension is 5.6% in the setting of isomerism. Independent risk factors for pulmonary hypertension in patients with isomerism include age, obesity, and history of anomalous pulmonary venous connection.
Keywords
Introduction
Bodily isomerism (hereafter simply ‘isomerism’) affects approximately 1 in 10,000 live births [Lin et al. 2014; Evans et al. 2015; Lopez et al. 2015]. Characterized by mirror imagery of viscera in several different organ systems, the cardiac, central nervous, pulmonary, gastrointestinal, genitourinary and immune systems may be affected to different degrees [Jacobs et al. 2007; Loomba et al. 2015a]. Previously segregated by splenic anatomy, isomerism is now understood to be more appropriately segregated on the basis of atrial appendage morphology [Uemura et al. 1995; Loomba et al. 2015b]. Left isomerism is associated with bilaterally acute angled and long main stem bronchi, bilaterally bilobed lungs, and the presence of multiple spleens. Right isomerism is associated with bilaterally obtuse angled and short main stem bronchi, bilaterally trilobed lungs, and absence of a spleen [Uemura et al. 1995]. The conduction system of the heart may also be abnormal with absence or presence of dual, sinoatrial or atrioventricular nodes. Isomerism of visceral structures is not simply an anatomic finding and can have various functional implications, although precise mechanisms for such findings is not entirely understood [Smith et al. 2006]. Those with multiple spleens may have functional asplenia while those with left bronchopulmonary isomerism are more likely to have recurrent otitis media and need for supplemental oxygen. Those with abnormal conduction systems are also more likely to develop arrhythmias [Loomba et al. 2015c; Loomba et al. 2015d].
With improvements in the care of infants and children with congenital malformations of the heart, there is an increasing number of adults with congenital heart disease, some of whom have isomerism [Loomba et al. 2016]. Pulmonary hypertension may be a consequence of congenital malformations of the heart, particularly in those with more complex malformations such as those requiring functionally univentricular palliation [McRae, 2013; Hsu, 2015; Krieger et al. 2015]. While anecdotally it has appeared that those with isomerism have an increased risk of pulmonary hypertension, formal studies explicitly investigating this are scarce. We used data from the Nationwide Inpatient Sample to determine the prevalence of pulmonary hypertension in adults with and without isomerism in the United States. We also used these data to determine whether or not isomerism is an independent risk factor for development of pulmonary hypertension.
Methods
Institutional review board approval was waived as this cross-sectional study utilizes de-identified data from a national database. These data are collected from community hospitals in the United States and the dataset captures 20% of discharges in the United States. Community hospitals, as per inclusion in the database, can also include some academic centers. This study is in compliance with the Helsinki declaration.
Patient identification
Data regarding hospital admissions were obtained from the 2012 iteration of the Nationwide Inpatient Sample which is the most recent iteration of the database. This database was developed for the Healthcare Cost and Utilization Project and was developed in partnership with the Agency for Healthcare Research and Quality. We acknowledge the Agency for Healthcare Research and Quality as well as the Nationwide Inpatient Sample for use of the database. Patients with isomerism were identified using the International Classification of Diseases, Ninth Revision (ICD-9) code 746.87. Patients with situs inversus totalis (complete mirror imagery) were not included in this group as situs inversus totalis does not portend isomerism. Admissions associated with pulmonary hypertension or a history of pulmonary hypertension were identified using a variety of ICD-9 codes: 416.0 for pulmonary hypertension and 416.8 for secondary pulmonary hypertension.
Data identification and collection
Demographic information including gender and race were collected for each admission. Admission characteristics such as admission month, length of stay, and cost of stay were also collected. Information regarding comorbid conditions was also collected. Hyperlipidemia was identified using ICD-9 codes 272.0, 272.1, 272.2, and 272.3 hypertension using 401.0, 401.1 and 401. Overweight or obese patients were identified using 278.00, 278.01, and 278.02 with current smokers being identified by 305.1.
Data of interest in regards to isomerism included cardiac anatomy as well splenic anatomy. The following congenital cardiac malformations commonly associated with isomerism were collected: functionally univentricular hearts using ICD-9 code 745.6, double outlet right ventricle using 745.11, atrioventricular septal defect using 745.6, partial anomalous pulmonary venous connection using 747.42, and total anomalous pulmonary venous connection using 747.41. Splenic abnormality, either absence of a spleen or presence of multiple spleens, was collected using 759.0. It was not possible to distinguish between those with absence of a spleen or multiple spleens due to the ICD-9 coding scheme.
Statistical analysis
Continuous variables were reported using mean and standard deviation while categorical variables were reported using absolute frequency and percentages. Continuous variables were analyzed using a Student’s t-test or Mann–Whitney test as appropriate with categorical variables being analyzed using Chi-square analysis. Baseline characteristics such as age, gender, race, and comorbid conditions were compared between those with and without isomerism. A univariate cross tabulation analysis was conducted to determine the odds of having pulmonary hypertension in patients with and without isomerism.
An aggregate of primary pulmonary hypertension and secondary pulmonary hypertension, was created and labeled as pulmonary hypertension. A multivariate logistic regression was then conducted with pulmonary hypertension as the dependent variable and age, gender, race, body habitus, and various congenital cardiac malformations as the independent variables. This regression included all patients with and without isomerism. Another multivariate logistic regression was then conducted with the same variables but only in patients with isomerism. All statistical analysis was done utilizing SPSS Version 20.0 (Chicago, IL).
Results
A total of 6,907,109 admissions of unique admissions, not patients, were included in the analysis. Of these, 861 (0.01%) had isomerism. Baseline characteristics did differ between those with and without isomerism. Isomerism admissions had a higher percentage of congenital malformations of the heart, tended to be male, and had a different distribution of race. Isomerism admissions also were less likely to have hyperlipidemia, hypertension, diabetes mellitus, and chronic kidney disease. Those with isomerism also tended not to be current smokers and were less likely to be overweight or obese. Age of admission did differ between the groups with isomerism admissions having a lower age of admission (Table 1).
Characteristics of hospitalizations for those with and without isomerism.

Pulmonary hypertension was present in 48 (5.6%) of those with isomerism and 176,306 (2.6%) of those without. This resulted in a 2.54 odds ratio of having pulmonary hypertension with isomerism (95% confidence interval 1.684 to 3.015, p < 0.0001) (Table 1).
Binomial logistic regression demonstrated that isomerism remained an independent risk factor after adjustment for other covariables. After multivariate analysis the resulting odds ratio was 1.789 (95% confidence interval 1.248 to 2.566, p = 0.002). Other independent risk factors for pulmonary hypertension, identified by multivariate analysis, were advanced age, female gender, smoking status, diabetes mellitus, obesity, double outlet right ventricle, atrioventricular septal defect, tetralogy of Fallot, ventricular septal defect, secundum atrial septal defect, anomalous pulmonary venous connection, functionally univentricular heart, and absence of a spleen (Table 2).
Risk factors of pulmonary hypertension.
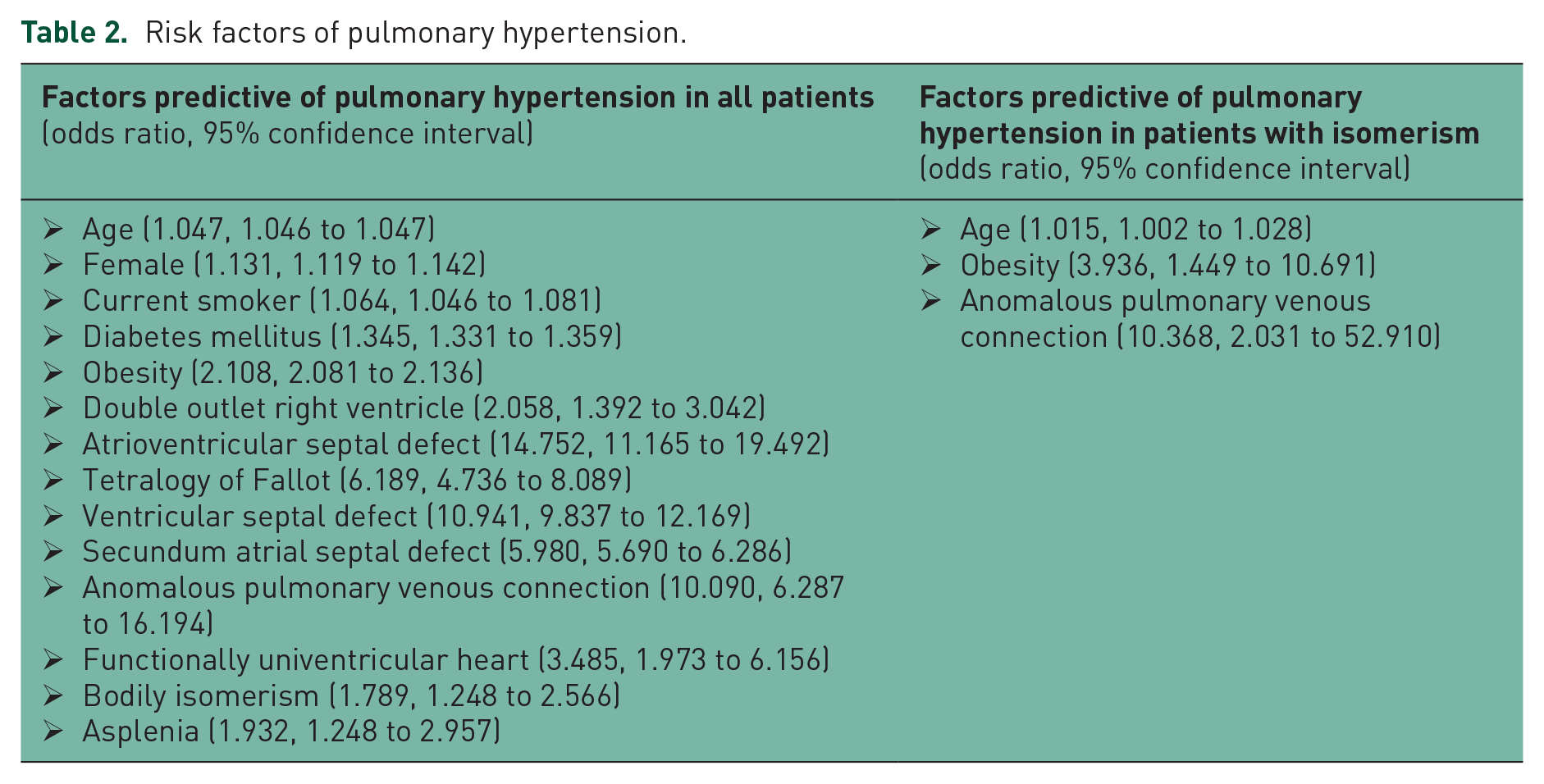
Binomial logistic regression of only patients with isomerism demonstrated the following independent predictors of pulmonary hypertension: advanced age (odds ratio 1.015, 95% confidence interval 1.002 to 1.028), obesity (odds ratio 3.936, 95% confidence interval 1.449 to 10.691), and anomalous pulmonary venous connection (odds ratio 10.368, 95% confidence interval 2.031 to 52.910) (Table 2).
Discussion
Pulmonary hypertension is a known sequelae of congenital malformations of the heart. While often associated with unpalliated cardiac defects, pulmonary hypertension is associated with even small residual defects in the setting of complex defects and after successful repair of defects without any residual lesions. This current study investigated the prevalence of pulmonary hypertension in adults with isomerism and demonstrated a higher prevalence of pulmonary hypertension in those with isomerism. The prevalence of pulmonary hypertension in those with isomerism was found to be 5.6%, with isomerism found to be an independent predictor of pulmonary hypertension. There was a 1.79-fold increase in the odds of pulmonary hypertension associated with isomerism when accounting for congenital malformations of the heart as covariables.
When only those with isomerism were further studied, multiple independent predictors of pulmonary hypertension were identified. The most significant of these were found to be age, obesity, and history of anomalous pulmonary venous connection.
It is vital that the increased risk for pulmonary hypertension be kept in mind when evaluating and managing the adult with isomerism. Patients should be screened for clinical symptoms associated with pulmonary hypertension at all follow-up visits. Echocardiography, often routinely obtained in these patients due to history of congenital malformations of the heart, should be done with pulmonary hypertension surveillance in mind to ensure that parameters such as septal wall flattening, right ventricular size and function, pulmonary artery size, and tricuspid regurgitation are all adequately demonstrated to help make a complete assessment for pulmonary hypertension.
The mechanisms of pulmonary hypertension in those with isomerism is yet to be systematically investigated. Pulmonary overcirculation and heart failure certainly may mediate the development of pulmonary hypertension but it is yet to be determined if other factors may also play a role [Gatzoulis et al. 2014; Krieger et al. 2015]. For instance, it is being increasingly understood that those with isomerism are more likely to have sinopulmonary symptoms when there is left bronchopulmonary isomerism. Additionally, those with isomerism are also more likely to have ciliary dyskinesia, the implications of which are not entirely understood in this unique setting. Current data also demonstrate decreased nitric oxide levels in patients with isomerism, secondary to ciliary dyskinesia [Nakhleh et al. 2012]. It is certainly plausible that this may contribute to pulmonary hypertension. Whether or not these factors play a role in the development of pulmonary hypertension, and if so, to what extent is unclear at this time.
As the precise mechanisms by which pulmonary hypertension develops in the setting of isomerism have not been entirely elucidated, the ideal therapy remains unclear. Calcium channel blockers, phosphodiesterase inhibitors, prostanoids, prostacyclin receptor agonists, and endothelin receptor antagonists have all been utilized for the treatment of pulmonary hypertension [Galie et al. 2013; Galie et al. 2015]. Therapies have shown varying efficacy in different patient populations and these differences have yet to be delineated in the setting of isomerism.
Those with isomerism, and their families, should be counseled regarding the risk of developing pulmonary hypertension. In cases where a prenatal diagnosis of isomerism has been made, it is worthwhile to counsel regarding the risk of pulmonary hypertension along with other associated findings such as intestinal malrotation, arrhythmias, and functional asplenia.
The functionally univentricular heart, often found in the setting of isomerism, does require some additional consideration when it comes to pulmonary hypertension. The definition of pulmonary hypertension still consists of a mean pulmonary artery pressure of greater than 25 mmHg. Mean pulmonary artery pressures of greater than 25 mmHg are intuitively not ideally compatible with functionally univentricular hearts due to the passive nature of systemic venous flow ultimately directly to the pulmonary arteries. What does often occur, however, is an increase in pulmonary vascular resistance which at a certain point is, for all extents and purposes, pulmonary hypertension in this population of patients. Medications used for treatment of pulmonary hypertension in those with biventricular hearts are now being utilized and studied in those with functionally univentricular hearts and increased pulmonary vascular resistance.
Some providers may code patients with functionally univentricular hearts and elevated pulmonary vascular resistance as having pulmonary hypertension even if the mean pulmonary artery pressure does not fulfill current criteria. Other providers may not code this as pulmonary hypertension thus making the prevalence obtained in our current study an underestimate. Additional limitations of this study also exist such as the retrospective nature of the study and other coding misclassifications. We also could not distinguish pulmonary hypertension from pulmonary arterial hypertension in this study. The largest limitation of this study is certainly that this analysis is based on billing codes. Another limitation is the fact that the database captures data based on admissions and not patients. Thus, some patients may have been included more than once in both groups.
Conclusion
Bodily isomerism is an independent risk factor for pulmonary hypertension, increasing the odds of developing pulmonary hypertension by 79%. Those with isomerism are more likely to develop pulmonary hypertension if they are older, are obese, or have a history of having anomalous pulmonary venous connections. Counseling regarding pulmonary hypertension should be provided to those with isomerism and evaluation of patients with isomerism should always include elements pertinent to early detection of pulmonary hypertension.
Footnotes
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Conflict of interest statement
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.