
Abstract
Abernethy malformation, also known as congenital extrahepatic portosystemic shunt, is an extremely rare vascular anomaly that alters systemic hemodynamics and may lead to progressive liver dysfunction, portal hypertension, and, in advanced stages, malignant transformation or hepatic encephalopathy. The condition is frequently associated with other congenital anomalies, most notably cardiac malformations such as septal defects, patent foramen ovale, Tetralogy of Fallot, and valvular regurgitation as well as skeletal abnormalities. We report the cases of two patients—one with type Ib and the other with type II Abernethy malformation. Both patients were asymptomatic, with the diagnosis established through contrast-enhanced computed tomography and magnetic resonance imaging. Clinical, laboratory, and imaging data were collected. Given the absence of overt clinical manifestations, both patients are being managed with semiannual follow-up. Abernethy malformation is difficult to diagnose based on clinical presentation alone; however, characteristic imaging features can facilitate a definitive diagnosis. Recognition of this rare entity and its potential comorbidities is essential for timely diagnosis and appropriate management.
Keywords
Introduction
Abernethy malformation, a rare vascular anomaly of the portal venous system, orchestrates the redirection of splenic and superior mesenteric vein (SMV) blood, effectively bypassing the portal vein and liver. It diverts blood flow into the inferior vena cava through aberrant communicating branches. After being initially described by Abernethy in 1793, Morgan classified this anomaly into two types in 1994 based on the presence of an intrahepatic portal vein. With advancements in imaging technology and a better understanding of this condition, Blanc proposed a refined classification system in 2014 that identifies the precise location of the anomalous communicating branches joining the venous system. 1 The malformation causes significant alterations in the overall hemodynamics and physiology of the organism, resulting in varied clinical manifestations. Diagnosis based solely on clinical presentation is challenging, and imaging modalities provide distinct and reliable indicators that improve diagnostic accuracy. Herein, we present one case each of type Ib and type II Abernethy malformation to enhance clinicians’ proficiency in diagnosing and managing this condition. This study aimed to mitigate the impact of misdiagnosis and its potential consequences on treatment strategies and disease progression.
The reporting of this study conforms to the Case Report (CARE) guidelines. 2
Case presentation
Case 1
A man in his late 20s was incidentally found to have hepatic masses during a routine chest computed tomography (CT) examination and was admitted 1 month later for further evaluation. The patient remained asymptomatic throughout the study. Laboratory evaluation revealed a total bilirubin level of 33.2 μmol/L, with direct and indirect bilirubin levels of 7.6 and 25.6 μmol/L, respectively.
Contrast-enhanced chest CT demonstrated an increased anteroposterior diameter of the left hemithorax, a mild leftward mediastinal shift, cardiomegaly, and an aberrant right subclavian artery. A well-defined, dome-shaped soft tissue mass (approximately 44 × 29 mm) was identified in the left posterior superior mediastinum, exhibiting mild-to-moderate enhancement. Additional findings included right first-rib hypoplasia and a neurogenic tumor in the same region (Figure 1).
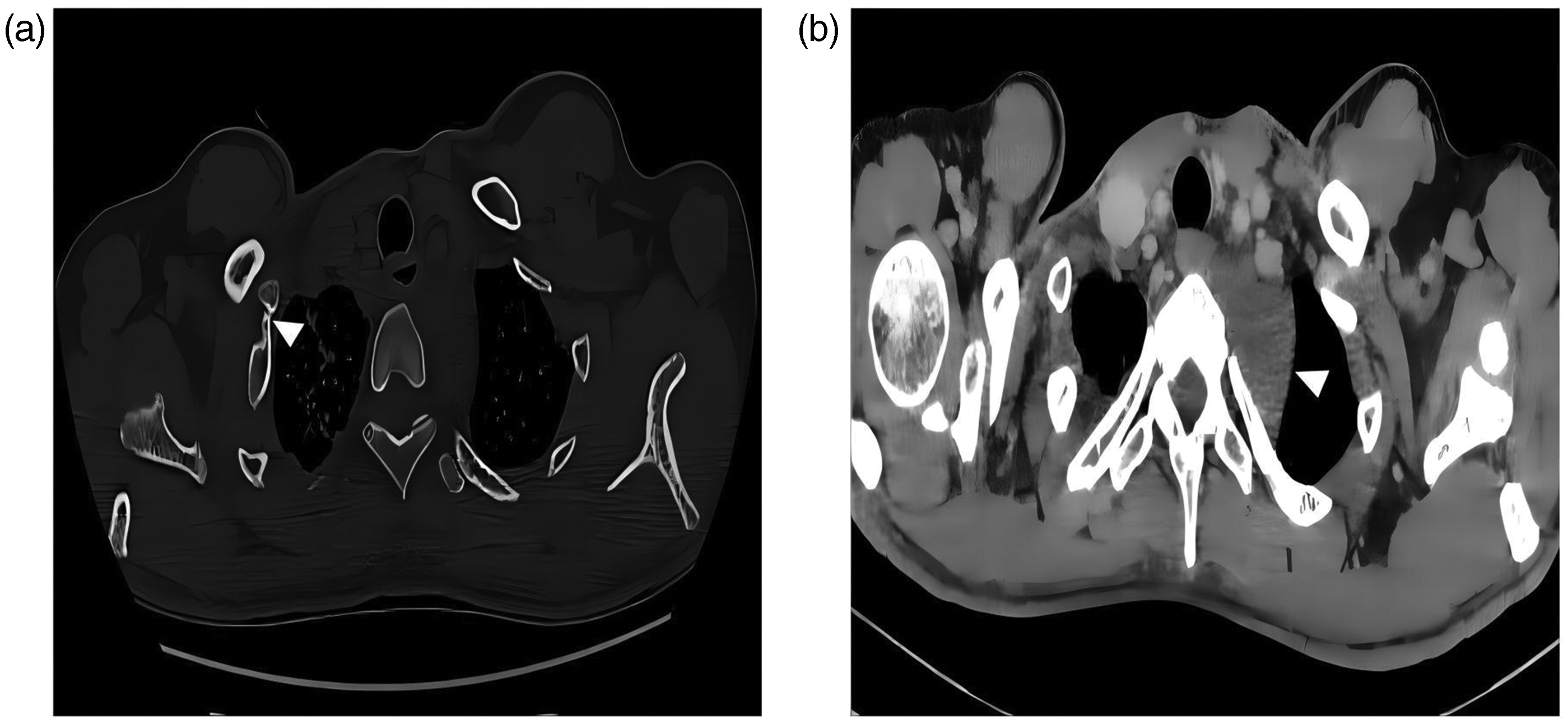
(a) Thoracic CT bone window displayed asymmetry in both thoracic structures, with underdeveloped and shortened right first rib, connecting to the second rib, and absence of the distal rib (arrow) and (b) thoracic CT mediastinal window revealed a flattened and elevated soft tissue mass in the left posterior superior mediastinum, demonstrating mild enhancement after contrast administration (arrow). CT: computed tomography.
Abdominal contrast-enhanced CT and magnetic resonance imaging (MRI) revealed the absence of intrahepatic portal vein branches. The hepatic artery was thickened, and an anomalous shunt formed by the confluence of the SMV and splenic vein (SV) drained directly into a dilated inferior vena cava. Hepatic veins were clearly visualized. A hypervascular lesion (10 × 9 mm) was observed in the distal splenic artery. Multiple small, fat-containing hepatic nodules demonstrated mild-to-moderate enhancement, suggestive of benignity. The left hepatic lobe exhibited regional enhancement patterns compatible with focal nodular hyperplasia (FNH) (Figure 2). According to the Blanc classification criteria, the patient was diagnosed with type Ib Abernethy malformation.
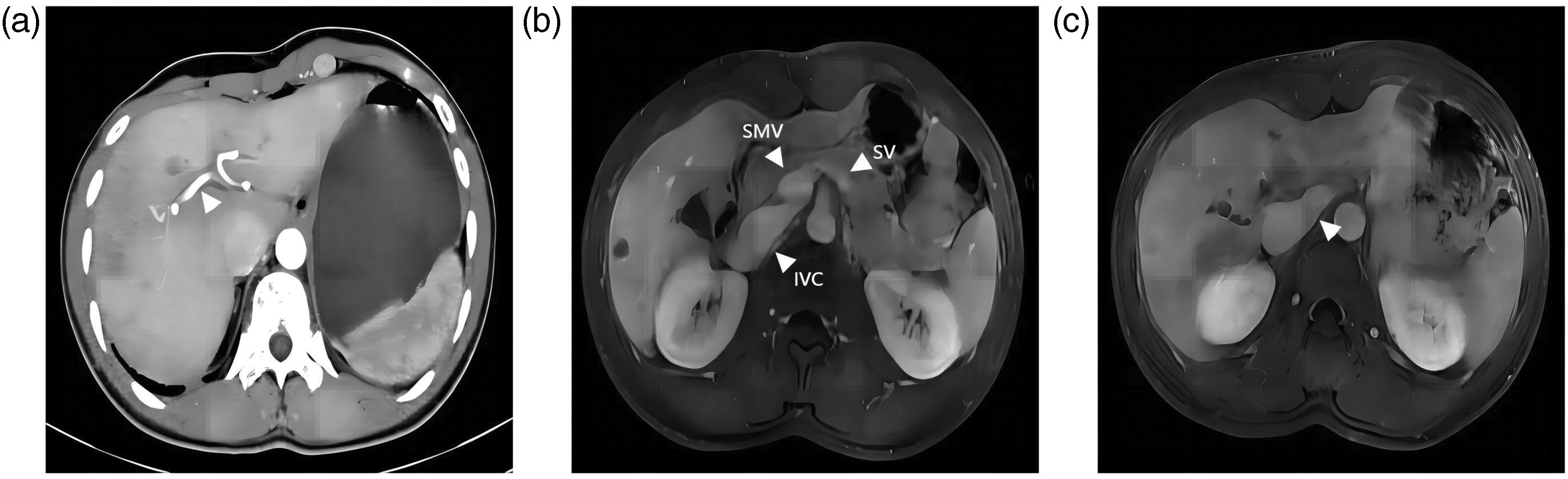
(a) Contrast-enhanced CT revealed the absence of the hepatic portal vein, with a tortuous and dilated hepatic artery within the portal vein course (arrow). (b) Contrast-enhanced MRI indicated the confluence of the SV with the mesenteric vein and (c) contrast-enhanced MRI highlighted the confluence of the SV and mesenteric vein forming a common trunk directly draining into the inferior vena cava (arrow).
The patient had a history of a congenital ventricular septal defect that was surgically corrected in early childhood. On physical examination, the patient was found to have a rib deformity. In the absence of symptoms, surgical intervention was deferred. The patient is currently undergoing semiannual follow-up with contrast-enhanced abdominal MRI (from 2021 to the present) and remains clinically stable.
Case 2
A boy in his early teens was referred for further evaluation following the incidental detection of multiple hepatic lesions on ultrasound performed at an outside facility. The patient was asymptomatic and exhibited no apparent clinical signs. Both physical examination and laboratory investigations were unremarkable.
Contrast-enhanced MRI of the liver revealed multiple abnormal signal foci of varying sizes. The largest lesion measured approximately 38 × 25 mm and demonstrated hyperintensity on T1-weighted imaging and slight hyperintensity on T2-weighted imaging. Some lesions exhibited heterogeneous internal signal characteristics. Postcontrast sequences showed mild-to-moderate enhancement with well-defined borders (Figure 3).

(a–d) Multiple rounded and patchy anomalous signals were observed in the liver. T1-weighted images exhibited high signals, while T2-weighted images showed slightly elevated signals. The signals within the lesions were uneven, and post–contrast enhancement images revealed sustained and nonuniform intensification of the lesions, with clear borders.
Although the main portal vein was present, its intrahepatic branches were absent, suggesting partial portal vein development or hypoplasia. Notably, the main portal vein directly communicated with a prominently dilated middle hepatic vein (MHV) (Figure 4). According to the Blanc classification criteria, the patient was diagnosed with type II Abernethy malformation.

(a, b) Enhanced MRI revealed the absence of branching in the hepatic portal vein. The enlarged main trunk of the portal vein connects directly to the MHV. MRI: magnetic resonance imaging; MHV: middle hepatic vein; PV: portal vein.
The patient is currently under regular follow-up. Surgical intervention will be considered if clinical symptoms emerge or if hepatic lesions demonstrate significant progression. The patient had no additional personal or family medical history.
Discussion
Abernethy malformation, also known as congenital extrahepatic portosystemic shunts (EHPS), is an exceedingly rare pathology. Its principal mechanism involves the diversion of partial or complete splenic blood and superior mesenteric venous blood, bypassing the portal vein and liver and flowing directly into the inferior vena cava through anomalous communicating branches. Type I Abernethy malformation is characterized by the absence of the intrahepatic portal vein and end-to-side portal vein shunting, whereas type II Abernethy malformation is characterized by the underdevelopment of the intrahepatic portal veins and side-to-side portal vein shunting. Type I is further subdivided into two forms—type Ia, in which the SMV and SV do not converge and independently drain into the inferior vena cava, and type Ib, in which the SMV and SV form a common trunk before joining the inferior vena cava. Blanc classification includes the EHPS type, portal caval (PC) type, portal hepatic type, and persistent ductus venous type, providing guidance for surgical planning and treatment strategies. The PC type, based on anatomical distinctions, is further divided into three subtypes: end-to-side type, side-to-side type, and H-type. 3
Embryologically, the portal venous system develops between the 4th and 10th gestational weeks from the vitelline venous system. Abernethy malformation is believed to result from excessive involution of the vitelline veins or failed anastomosis between the vitelline and umbilical venous systems.4,5 Abnormal persistence or regression of these embryonic channels contributes to the development of either type I or type II Abernethy malformation. Some authors have also speculated the potential involvement of genetic mutations. 6 However, the limited number of reported cases had precluded the establishment of definitive causative links, highlighting the need for further molecular and developmental studies.
Abernethy malformation frequently coexists with other congenital anomalies. It is most frequently associated with cardiovascular malformations, including atrial and ventricular septal defects, patent foramen ovale, Tetralogy of Fallot, and valvular insufficiencies.1,7,8 In the present study, patient 1 had a history of a congenital ventricular septal defect surgically corrected 26 years earlier. Skeletal anomalies, including thoracic deformities, digit abnormalities, and pelvic asymmetry, have also been reported.9–11 Notably, patient 1 exhibited a chest wall deformity characterized by the absence of the right first rib and its costal cartilage—a finding consistent with that of prior case reports—supporting the hypothesis that Abernethy malformation may represent a broader spectrum of developmental dysmorphogenesis.
Abernethy malformation substantially alters splanchnic hemodynamics and hepatic perfusion, leading to considerable variability in clinical presentation. In early stages, patients may remain asymptomatic; however, as the disease progresses, complications such as hepatic decompensation, portal hypertension, hepatopulmonary syndrome, splenomegaly, pulmonary hypertension, or nephrotic syndrome may develop. In advanced stages, benign hepatic nodules may undergo malignant transformation, resulting in hepatocellular carcinoma or hepatic encephalopathy.12–14 Literature indicates that approximately 40% of patients develop hepatic nodules, most commonly FNH, followed by nodular regenerative hyperplasia and hepatoblastoma.15,16 In this study, both patients exhibited imaging-confirmed FNH, with patient 1 showing progressive enlargement and an increasing number of lipid-rich nodules over a 5-year follow-up period (from 2021 to the present). Diagnosis of Abernethy malformation primarily relies on imaging. Abdominal CT and MRI are essential for delineating anomalous vascular anatomy and classifying shunt type. In patient 1, imaging revealed the complete absence of intrahepatic portal venous branches, with a common SMV–SV trunk draining directly into a dilated inferior vena cava, consistent with type Ib Abernethy malformation. In patient 2, the main portal vein was visualized with distal communication to the MHV, while the right and left portal branches were poorly defined—hallmarks of type II Abernethy malformation. Additionally, patient 1 was found to have an incidental neurogenic tumor in the left upper mediastinum (Figure 1). However, given the limited number of reported cases, it is not currently possible to perform an in-depth investigation into the potential association between Abernethy malformation and neurogenic tumors. Furthermore, there are certain limitations in our two cases. First, we did not perform genetic testing to explore potential genetic associations of Abernethy malformation. Second, as contrast-enhanced abdominal MRI was sufficient to establish a presumptive diagnosis, the clinicians did not pursue additional detailed investigations, such as balloon occlusion testing, and ultrasound examination was not performed in case 2.
Patients with Abernethy malformation often present with significant anatomical abnormalities and are prone to developing concomitant hepatic disorders. Routine annual abdominal examinations—such as ultrasonography, CT, or MRI—can facilitate the detection of abnormal vascular courses or atypical lesions, thereby prompting further diagnostic evaluation and enabling a definitive diagnosis. Although noninvasive imaging methods such as ultrasound, CT, and MRI are useful for diagnosis, they may not reliably differentiate type I from type II shunts in ambiguous cases. Misclassification may lead to inappropriate management. Balloon occlusion testing serves as a functional diagnostic tool to evaluate portal venous patency and guide therapeutic decisions. Despite its invasive nature, angiography remains the gold standard for definitive anatomical and hemodynamic assessment, but it is reserved for select cases due to associated procedural risks. Management of Abernethy malformation is individualized according to anatomical classification, clinical presentation, and presence of complications. Currently, no standardized treatment protocol exists; hence, therapeutic decisions are individualized. Asymptomatic patients without overt hepatic dysfunction or complications are typically managed with semiannual clinical and imaging follow-up. In this study, both patients exhibited no apparent clinical symptoms or severe complications and were therefore advised to undergo monitoring at 6-month intervals. Symptomatic patients, particularly those with hepatic tumors, hepatic encephalopathy, or cardiopulmonary comorbidities, require active clinical intervention. Type I Abernethy malformation, characterized by the complete absence of intrahepatic portal flow, is commonly managed with liver transplantation, particularly in the presence of intractable hyperammonemia, hepatic tumors (e.g. hepatocellular carcinoma or hepatoblastoma), or biliary anomalies such as biliary atresia. Patients with type II Abernethy malformation may undergo shunt closure procedures through surgical or transcatheter ligation, using one-stage or two-stage occlusion depending on portal pressure. Balloon occlusion testing with portal vein pressure (PVP) measurement guides the feasibility and timing of shunt closure: PVP <25 mmHg indicates suitability for single-stage occlusion; PVP >30 mmHg suggests consideration of liver transplantation or staged intervention; and a PVP of 25–30 mmHg requires individualized planning based on patient-specific parameters. 17 After successful shunt closure, patients often experience partial restoration of intrahepatic portal perfusion, improvement of hepatic encephalopathy, normalization of serum ammonia, and regression of benign hepatic lesions.18,19
Conclusion
In summary, Abernethy malformation, an exceedingly rare condition, induces alterations in the overall hemodynamics and physiology of the body due to its anomalous nature. This leads to substantial variations in clinical presentation among patients, including liver-related symptoms and those affecting the skeletal and circulatory systems. Diagnosis based solely on clinical presentations is challenging; however, radiologic features are clear, thereby allowing for a conclusive diagnosis. When further therapeutic interventions are considered, balloon occlusion testing may help delineate the shunt subtype and guide treatment planning.
Footnotes
Acknowledgements
None.
Author contributions
Yiqi Ma: Conceptualization, Methodology, Writing–Original Draft; Zhiming Cui: Writing–Original Draft; Jibo Hu: Conceptualization, Methodology, Writing–Review & Editing.
Data availability statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Declaration of conflicting interests
All authors declare no competing interests.
Disclosure
Nothing to disclose.
Ethics
We obtained approval from the Ethics Committee of The Fourth Affiliated Hospital, Zhejiang University School of Medicine, for human research on 8 January 2024 (Approval No.: K2024002). Furthermore, the presentation of the case does not allow for the identification of the patient and thus adheres to the principles of patient privacy and autonomy. The study did not involve any interventions, alterations in patient care, or additional procedures beyond standard clinical care. The study aimed solely at educational purposes, intending to share knowledge and insights without any commercial interests. The report aligns with the institution’s policies regarding the publication of case reports.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Informed consent
Informed consent for publication was not applicable because we have de-identified all patient details.