
Abstract
Asthma and chronic obstructive pulmonary disease (COPD) are different disease entities. They are both clinical diagnoses, with diagnostic tools to discriminate between one another. However, especially in older patients (>55 years) it seems more difficult to differentiate between asthma and COPD. This has led to the definition of a new phenotype called asthma COPD overlap syndrome (ACOS). However, our understanding of ACOS is at a very preliminary stage, as most research has involved subjects with existing diagnoses of asthma or COPD from studies with different definitions for ACOS. This has led to different and sometimes opposing results between studies on several features of ACOS, also depending on the comparison with COPD alone, asthma alone or both, which are summarized in this review.
We suggest not using the term ACOS for a patient with features of both asthma and COPD, but to describe a patient with chronic obstructive airway disease as completely as possible, with regard to characteristics that determine treatment response (e.g. eosinophilic inflammation) and prognosis (such as smoking status, exacerbation rate, fixed airflow limitation, hyperresponsiveness, comorbidities). This will provide a far more clinically relevant diagnosis, and would aid in research on treatment in more homogenous groups of patients with chronic airways obstruction. More research is certainly needed to develop more evidence-based definitions for this patient group and to evaluate biomarkers, which will help to further classify these patients, treat them more adequately and unravel the underlying pathophysiological mechanism.
Introduction
Patients with chronic airflow limitation are mostly diagnosed with chronic obstructive pulmonary disease (COPD) or asthma. COPD is characterized by persistent airflow limitation that is usually progressive and associated with an enhanced chronic inflammatory response in the airways and lung to noxious particles or gases. Exacerbations and comorbidities contribute to the overall severity in individual patients [Global Initiative for Chronic Obstructive Lung Disease (GOLD), 2015]. Asthma, however, is a heterogeneous disease with a history of respiratory symptoms, such as wheezing, shortness of breath, chest tightness and cough that vary over time and in intensity, together with variable expiratory airflow limitation and usually with chronic airway inflammation [Global Initiative for Asthma (GINA), 2015]. With regard to aetiology, different hypotheses have been generated, some postulating that asthma and COPD are diseases with the same aetiology, whereas others suggest that they are different diseases [Orie, 1961; Vermeire and Pride, 1991]. Still, more recent data suggest that there is no common genetic component to asthma and COPD, and this further confirms the opinion that these diseases should be regarded as pathophysiologically different [Postma and Rabe, 2015; Smolonska et al. 2014]. In clinical practice, some patients depict characteristics from both diseases which makes it hard to diagnose these patients as having either asthma or COPD.
It has been well recognized that specific phenotypes exist in patients with COPD and asthma. These patients fulfil the diagnosis of either COPD or asthma, but have specific characteristics that determine symptoms, exacerbations and disease progress. In addition, it has been known that patients who have been previously diagnosed with COPD can have features of asthma, and patients with asthma can develop more persistent airflow limitation similar to COPD. This is called the asthma COPD overlap syndrome (ACOS) and many studies have been performed to establish prevalence, risk factors, comorbidities and factors that determine disease progression in patients who could be referred to as having ACOS. It has been shown that patients with ACOS have increased reversibility of airflow, more exacerbations and more severe dyspnoea. Identifying patients with ACOS seems therefore relevant for the management of their disease. But is it wise to determine all patients with asthma or COPD and overlap characteristics as one phenotype, or could that induce too much overlap? In this review we discuss the difficulties in the definition of ACOS and with that the differences in outcomes of studies on ACOS.
Definition
A broad variety of definitions have been used to define ACOS and clearly patient numbers and characteristics are very much dependent on the criteria used. In 2007, the Canadian guidelines for COPD stated that in some patients with COPD early introduction of inhaled corticosteroids (ICS) might be justified. These were patients with COPD with features of asthma [large short-acting bronchodilator improvement in forced expiratory volume in 1 s (FEV1) (e.g. greater than 0.4 liter), marked diurnal variability of peak expiratory flow rates or significant fluctuations over time in any measure of airway obstruction, large spirometric improvements following treatment with inhaled or oral steroids) [O’Donnell et al. 2007]. Bronchodilator reversibility is a criterion often used. For example, ACOS has been defined as a not completely reversible airflow obstruction accompanied by symptoms or signs of variable airways obstruction [Gibson and Simpson, 2009], or as the diagnosis of COPD in a patient with a previous history of asthma before the age of 40 [Hardin et al. 2011]. But also, ACOS has been defined as two clinical phenotypes: asthma with partially reversible airflow obstruction, with or without emphysema or reduced carbon monoxide diffusion capacity (DLCO) to less than 80% predicted; and COPD with emphysema accompanied by reversible or partially reversible airflow obstruction with or without environmental allergies or reduced DLCO [Louie et al. 2013]. A document from Global initiative for chronic obstructive lung disease (GOLD) and GINA described ACOS as persistent airflow limitation with several features usually associated with asthma and several features usually associated with COPD [GINA-GOLD, 2015]. When a patient has similar numbers of features of both asthma and COPD, the diagnosis of ACOS should be considered. The Spanish guidelines proposed four clinical phenotypes of COPD, one of them being mixed COPD–asthma phenotype. This was defined as an airflow obstruction that is not completely reversible accompanied by symptoms or signs of increased reversibility of obstruction [Miravitlles et al. 2014b]. In a consensus document from Spain, major and minor criteria were formulated. For the diagnosis of ACOS a patient must meet two major or one major and two minor criteria: major criteria included a very positive bronchodilatory test (increase in FEV1 > 15% and > 400 ml), eosinophilia in sputum and personal history of asthma. Minor criteria included high total immunoglobulin E, personal history of atopy and positive bronchodilator test (FEV1 > 12% and > 200 ml) on two or more occasions [Soler-Cataluna et al. 2012]. From the perspective of asthma, Lee and colleagues defined the overlap phenotype as patients with asthma and fixed airflow obstruction [Lee et al. 2014] in combination with other features of asthma (positive response to bronchodilator: >200 ml FEV1 and >12% baseline, or positive methacholine or mannitol provocation test).
Thus there are differences and similarities between the definitions of ACOS used so far. This can be explained by the fact that no diagnostic tool is available and more importantly the underlying mechanism is not clear. In Table 1 multiple studies on ACOS have been summarized with the definitions used for asthma, COPD or overlap syndrome.
Definition of asthma, COPD and asthma COPD overlap syndrome per study.
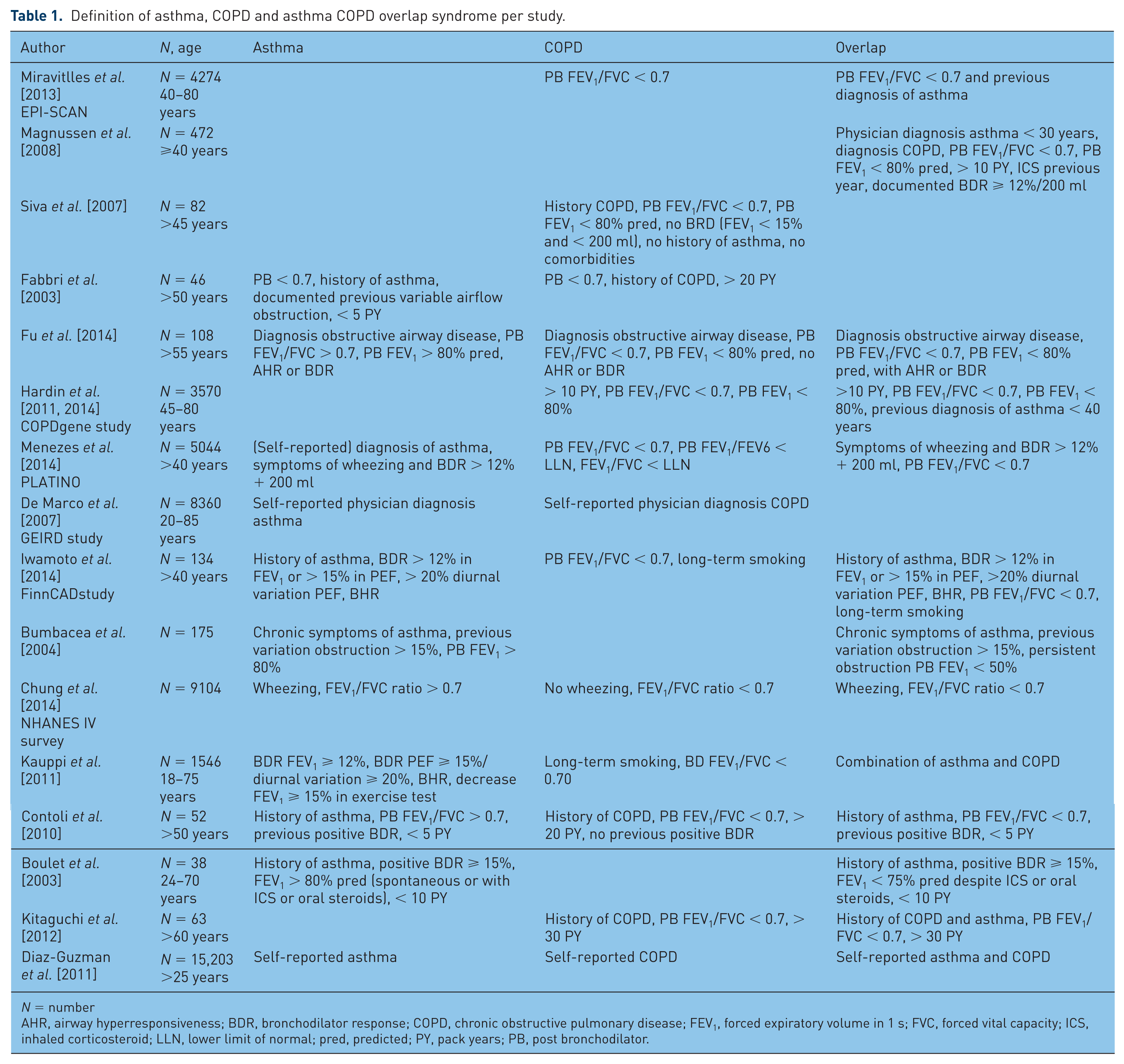
N = number
AHR, airway hyperresponsiveness; BDR, bronchodilator response; COPD, chronic obstructive pulmonary disease; FEV1, forced expiratory volume in 1 s; FVC, forced vital capacity; ICS, inhaled corticosteroid; LLN, lower limit of normal; pred, predicted; PY, pack years; PB, post bronchodilator.
Prevalence
Understandably, studies on prevalence differ in results since different definitions were used, different types of cohorts examined (patients with COPD, patients with airway obstruction or general population) and different study forms used. Database studies show higher prevalence compared with clinical studies, ranging from 52% to 55% [Marsh et al. 2008; Rhee et al. 2014; Soriano et al. 2003]. In the general population of Italy, the prevalence of ACOS was 4.5% in the 65–84 age group [De Marco et al. 2013]. In Latin America (PLATINO study) it was 1.8% [Menezes et al. 2014]. In comparison, the prevalence of ACOS among patients with COPD ranges from 5% to 17% [Golpe et al. 2014; Miravitlles et al. 2014a]. For example, data from the COPDgene study USA showed that 13% of patients had ACOS [Hardin et al. 2011], defined as more than 10 pack years, postbronchodilator FEV1/forced vital capacity (FVC) less than 0.7 plus FEV1 less than 80% predicted, and a physician diagnosis of asthma before the age of 40. Another study from Spain in a cohort of 3885 subjects identified 10% as having COPD (FEV1/FVC ratio < 0.7), of which 17.4% could be classified as having ACOS (FEV1/FVC ratio < 0.7 plus previous diagnosis of asthma) [Miravitlles et al. 2013]. In the PLATINO study the prevalence of ACOS in patients with COPD was 11.6%, with ACOS defined as postbronchodilator FEV1/FVC less than 0.7 and asthma diagnosis [Menezes et al. 2014].
Relevance of identifying ACOS
Defining a specific subgroup or phenotype such as ACOS is of relevance if such patients present with differential (clinical) characteristics, with different treatment options or prognosis, compared with either asthma or COPD alone. It has been recognized that some patients with COPD respond better to ICS than others, and that some patients with asthma develop fixed airflow obstruction with worse prognosis. Also, patients with chronic airflow obstruction with both features of asthma and COPD experience more frequent exacerbations, have worse quality of life, more rapid decline in lung function and a higher mortality than asthma or COPD alone. However, up till now, it is unclear whether the presence of features of both asthma and COPD in one patient arises from the same pathophysiological mechanism and which characteristics of this subgroup determine differences in disease severity and prognosis. Research on new treatments in such a heterogeneous group can lead to negative results for the whole group, whereas a subgroup can indeed benefit from this treatment. This has been the case in the past for anti-interleukin-5 treatment in asthma if patients are not defined according to specific features (e.g. eosinophilic inflammation), but defined as an overall group [Leckie et al. 2000]. From the literature so far on ACOS we have derived features of patient characteristics, disease burden, inflammation, and prognosis and summarized them in Table 2. First, ACOS has not always been compared with both asthma and COPD, giving different results on the same measures. Second, opposing results have been shown between studies on the same measures due to differences in definitions used (Table 1). We will discuss some of these features from Table 2.
Summarization of characteristic features of ACOS, derived from studies from Table 1.

ACOS, asthma COPD overlap syndrome; AT, antitrypsin; COPD, chronic obstructive pulmonary disease; CRP, C-reactive protein; IgE, immunoglobulin E; IL, interleukin; MPO, myeloperoxidase; MWT, minute walk test; NGAL, neutrophil gelatinase associated lipocalin; NO, nitric oxide; NOx, nitrite/nitrate; SNP, single-nucleotide polymorphism; SP-A, surfactant protein A; sRAGE, soluble receptor for advanced glucation end product; TNF, tumour necrosis factor.
Influence of smoking
We know that FEV1 declines continuously and slowly during life, but nonsmokers almost never develop clinically significant airflow obstruction [Fletcher and Peto, 1977]. This is also the case for many smokers. However, smokers who are more susceptible demonstrate an accelerated lung function decline and develop various degrees of airflow obstruction, which in some ultimately becomes disabling or fatal. Also, a susceptible smoker who stops smoking will not recover lost FEV1, but the subsequent rate of loss of FEV1 will revert to normal. These findings have since then been the cornerstone of COPD management, namely to advise smoking cessation.
Several studies have also shown that smoking accelerates loss of lung function in asthma [Anthonisen et al. 2002; James et al. 2005; Lange et al. 1998], and reduces the effectiveness of ICS [Lazarus et al. 2007]. Perret and colleagues studied the interaction between current asthma, atopy and smoking in a group of middle-aged (40–44 years) subjects with fixed airflow obstruction [Perret et al. 2013]. Fifty-seven percent of the cohort were ever smokers, with 9.5% having a smoking history of more than 30 pack years. About 26% of patients with current asthma were current smokers. The combination of atopy, smoking and current asthma related to worse postbronchodilator FEV1/FVC levels. In another study, the interaction between asthma, bronchial hyperresponsiveness and smoking related to a faster decline in postbronchodilator FEV1 [Tashkin et al. 1996]. Furthermore, patients with asthma who smoke have more symptoms compared with those who do not smoke [Thomson et al. 2004]; strangely though asthma is a risk factor for starting smoking and becoming a regular smoker [Van De Ven et al. 2009].
Different results have been found for smoking history in patients with ACOS compared with asthma or COPD alone. Mostly, smoking status of ACOS is between that of patients with asthma or COPD (Table 2). However, smoking is a risk factor for both diseases, reduces treatment response to ICS and accelerates lung function decline in asthma and COPD. Smoking status should therefore be defined in research on ACOS.
Biomarkers
The role of biomarkers in the diagnostics and management of asthma or COPD is somewhat controversial. Indeed, several markers such as number of eosinophils in sputum or blood, exhaled nitric oxide and different markers in serum such as periostin or interleukin (IL)-6 have been investigated for asthma or COPD. In ACOS, the role and function of these markers is unclear but it can be speculated that biomarkers could help us to better diagnose and classify patients. In addition, they could benefit current research and improve our understanding of the pathophysiological mechanism of ACOS. In the COPD gene cohort single-nucleotide polymorphisms (SNPs) in the GPR65 gene were associated with ACOS in a population of smokers or ex-smokers with COPD [Hardin et al. 2014]. GPR65 is a member of the G2A G protein coupled family and plays a role in eosinophil activation in asthma. GRP65 knockout mice have attenuated airway eosinophilia [Kottyan et al. 2009]. Presence of this SNP could identify patients with COPD with eosinophilic inflammation, and with that, better treatment response to corticosteroid treatment.
Systemic inflammation is a feature of chronic inflammatory airways disease [De Martinis et al. 2005]. In COPD low-grade elevation of circulating proinflammatory mediators (C-reactive protein, IL-6) have been associated with acute exacerbations [Dickens et al. 2011], hospitalization, and more rapid decline of FEV1 [Dahl et al. 2007]. Also, these markers of systemic inflammation are associated with age, smoking [Pinto-Plata et al. 2006], comorbid disease, such as cardiovascular disease [Danesh et al. 2004], obesity and diabetes [Bastard et al. 2006]. High levels of IL-6 are inversely related to FEV1 [Fu et al. 2014; Walter et al. 2008], a faster decline in FEV1 [Thorleifsson et al. 2009] and with an increased risk of developing COPD [Yanbaeva et al. 2009]. In asthma, Oncostatin M, a member of the IL-6 family of cytokines, was associated with incompletely reversible airflow obstruction [Simpson et al. 2009]. In ACOS, systemic inflammation is frequently present, comparable to COPD, with increased levels of IL-6 compared with healthy controls and asthma, but still lower than COPD. Multivariate logistic regression modelling suggests that age, Co-morbidity Index (CCI) and IL-6 levels were associated with ACOS. Also, IL-6 levels were higher in patients with cardiovascular disease compared with patients without the disease, suggesting that systemic inflammation leads to comorbid disease. Interestingly, in a univariate logistic regression analysis, FEV1 % predicted, sputum neutrophil counts, CCI and IL-6 predicted the risk of having ACOS (not sputum eosinophils) [Fu et al. 2014]. In contrast, in the EPISCAN study several blood biomarkers were evaluated, namely albumin, α1 antitrypsin, fibrinogen, C-reactive protein, tumour necrosis factor (TNF)-α, IL-6, IL-8 and nitrite/nitrate (NOx). No significant differences were found in the level of these biomarkers in blood samples in patients with overlap compared with those with COPD alone, except for NOx [Miravitlles et al. 2013]. Lower NOx might indicate a decrease in oxidant activity compared with COPD alone. Iwamoto and colleagues investigated four potential biomarkers in COPD, asthma and ACOS [Iwamoto et al. 2014]. Compared with asthma, sputum myeloperoxidases and plasma surfactant protein A were significantly elevated in ACOS and COPD and soluble receptor for advanced glycation end products was decreased in ACOS and COPD. Only sputum neutrophil gelatinase associated lipocalin (NGAL) was significantly increased in ACOS compared with COPD and asthma, and was able to differentiate patients with ACOS from those with COPD and asthma. A cluster analysis on severe asthma and COPD revealed a distinct group with higher levels of sputum IL-1β and TNFα, which contained both patients with asthma as well as COPD [Ghebre et al. 2015]. Thus, no specific biomarker for ACOS has been established yet, except for NGAL. Sputum NGAL levels might be related to neutrophilic inflammation or ongoing respiratory epithelium damage [Karlsen et al. 2010; Yan et al. 2001], suggesting that the inflammatory pattern or respiratory damage is different in COPD alone, asthma alone and ACOS.
Bronchial hyperresponsiveness
Bronchial hyperresponsiveness refers to an exaggerated response to (indirect) stimuli leading to airways narrowing. In the SAPALDIA study the role of bronchial hyperresponsiveness in the development of asthma and COPD was studied. Nine percent of the population had asymptomatic bronchial hyperresponsiveness. However, this was associated with an increased risk of developing newly diagnosed asthma or COPD [Brutsche et al. 2006]. In addition, smoking is a risk factor for developing bronchial hyperresponsiveness, and bronchial hyperresponsiveness is associated with accelerated lung function decline [Rijcken et al. 1993] with a significant interaction with smoking [Betz et al. 2001]. Thus active smokers with asymptomatic bronchial hyperresponsiveness are more prone to accelerated lung function decline leading to COPD, especially with fetal or childhood exposure to smoking leading to incomplete airway growth [Peat et al. 1987]. Bronchial hyperresponsiveness can be demonstrated in 14% of patients with COPD [Nakawah et al. 2013]. In patients with asthma or COPD, more severe bronchial hyperresponsiveness is associated with more severe symptoms and more rapid decline in FEV1. Therefore, assessment of bronchial hyperresponsiveness in a patient with chronic obstructive lung disease is important since it determines prognosis in terms of lung function decline. However, in studies on ACOS a difference in bronchial hyperresponsiveness was only reported in one study [De Marco et al. 2007].
Airway inflammation
Airway inflammation is a common feature of both asthma and COPD; though, as mentioned above, in asthma airway inflammation is predominantly eosinophilic, whereas in COPD the numbers of neutrophils are increased. Older patients (>55 years) with asthma (<5 pack years) with previous variable airflow obstruction who develop fixed airflow obstruction (postbronchodilator FEV1/FVC < 0.7) have a higher percentage of eosinophils in the blood, sputum, bronchoalveolar lavage (BAL) and airways compared with those with COPD (>20 pack years) with fixed airflow obstruction and no previous variable airflow obstruction [Fabbri et al. 2003], and fewer neutrophils in sputum and BAL. In addition, BAL lymphocytes were higher, with more CD4+ cells and a higher CD4+/CD8+ ratio. Finally, exhaled nitric oxide (NO) was higher in patients with asthma compared with those with COPD. Only 1 out of 27 patients with COPD had sputum eosinophilia greater than 4.6%, and 4 out of 27 (14.8%) had sputum eosinophilia greater than 3%. Also, patients with asthma and incompletely reversible airflow obstruction, in the absence of smoking, showed increased exhaled NO and blood eosinophils [Bumbacea et al. 2004].
Smokers with asthma have inflammatory features resembling COPD, namely less eosinophilic inflammation [Chalmers et al. 2001] and are more likely to have neutrophilic inflammation [Boulet et al. 2006]. Patients with severe asthma, fixed airflow obstruction despite high-dose ICS or oral corticosteroids, showed prominent neutrophilia in bronchial biopsies [Wenzel et al. 1997, 1999]. In contrast, in severe asthma the presence of sputum eosinophilia is an important determinant of developing fixed airflow obstruction [Ten Brinke et al. 2001]. Unselected patients with asthma and incomplete reversibility of airways obstruction demonstrate increased airway neutrophilia, related to FEV1 decline [Boulet et al. 2003; Shaw et al. 2007]. Older patients (>55 years] with respiratory symptoms, persistent airways obstruction (postbronchodilator FEV1/FVC < 70% and FEV1 % predicted < 80%) and airway hyperresponsiveness had higher sputum neutrophils compared with patients with asthma alone [Gibson and Simpson, 2009].
In COPD, eosinophilic inflammation has been shown during exacerbations both in induced sputum as well as in bronchial biopsies [Brightling et al. 2000]. In addition, blood eosinophilia was associated with increased mortality [Hospers et al. 1999]. Patients with COPD and eosinophilic inflammation during exacerbation usually have increased concentrations of peripheral eosinophils in stable disease as well [Bafadhel et al. 2011]. Christenson and colleagues identified a set of airway epithelial genes that are altered in asthma, and in some current and former smokers with COPD [Christenson et al. 2015]. This ‘Th2 gene signature’, associated with asthma-like inflammation, is also expressed in COPD and is associated in those patients with eosinophilic inflammation, reversibility and favourable corticosteroid response as reflected by more improvement in hyperinflation. Improvement in hyperinflation in COPD is important since it is related to dyspnoea and exercise tolerance [McDonough et al. 2011].
In studies on ACOS, different results are found with regard to sputum and blood eosinophils, and exhaled NO, depending on the definition of ACOS (Table 1) and groups compared (Table 2). COPD with concomitant asthma has been associated with more eosinophilic inflammation, as shown by more peripheral and sputum eosinophils [Kitaguchi et al. 2012; Papi et al. 2000], and in addition, these patients responded better to ICS [Brightling et al. 2005; Kerstjens et al. 1993; Kitaguchi et al. 2012; Leigh et al. 2006]. Iwamoto showed increased sputum eosinophilia in patients with asthma and ACOS compared with healthy smokers and those with COPD [Iwamoto et al. 2014]. However, patients with overlap syndrome and COPD had more sputum neutrophilia compared with those with asthma and healthy controls. Sputum eosinophilia or neutrophilia therefore does not seem to be a distinguishing feature for ACOS as defined in these studies compared with asthma or COPD alone.
Remodelling
Airway wall remodelling refers to alterations in the distinct aspects of the airway wall, that is, mucosal oedema, airway smooth muscle hypertrophy and hyperplasia, and thickening of basal membrane. This leads to airway wall thickening and altered airway mechanics. Airway remodelling occurs throughout the whole respiratory tract, including small airways [Skold, 2010]. Both in asthma and COPD there is evidence of airway wall thickening and remodelling, however the degree of changes in specific structures of the airway wall differ between asthma and COPD [Bosken et al. 1990; Fabbri et al. 2003; Hogg et al. 2004; James and Wenzel, 2007; Wright et al. 1983]. In several studies, increased bronchial wall thickening has been demonstrated on high-resolution computed tomography scans in patients with overlap syndromes compared with COPD alone [Bumbacea et al. 2004; Hardin et al. 2014; Kitaguchi et al. 2012], but has not been compared in patients with asthma alone. In a small group of nonsmoking patients with asthma, a decrease in lung elastic recoil was demonstrated, with microscopic centrilobular emphysema in three autopsied patients [Gelb and Nadel, 2015]. However, there are no data yet on whether the specific structures of airway remodelling differ in overlap syndrome compared with asthma and COPD alone.
Exacerbations
Exacerbations in both asthma and COPD can lead to accelerated lung function loss, and thus to incompletely reversible obstruction [Vonk et al. 2003]. Patients with asthma with fixed airflow obstruction have greater lung function decline and more exacerbations compared with reversible airflow obstruction [Contoli et al. 2010]. Patients with ACOS appear to have more frequent exacerbations compared with patients with COPD alone, despite similar lung function and fewer years of smoking [Hardin et al. 2011; Miravitlles et al. 2013], and also have more severe exacerbations compared with patients with asthma alone [De Marco et al. 2013; Menezes et al. 2014], although one study showed no difference in exacerbation frequency between patients with ACOS and those with COPD alone [Izquierdo-Alonso et al. 2013].
Treatment
Data on medical treatment of patients with ACOS is rare because this patient group has been systematically excluded from both COPD and asthma pharmacological trials. As a consequence, there is little information about the response of these patients to most of the current pharmacological therapies.
Response to (inhaled) corticosteroids
In the latest GOLD guidelines, ICS treatment in addition to long-acting muscarinic receptor antagonist (LAMA)/long-acting beta-adrenoreceptor agonist (LABA) is advised in patients with more severe symptoms or in those with more than two exacerbations per year [GOLD, 2015].However, not all patients with COPD respond equally to all drugs (irrespective of the severity of symptoms or level of risks), thus it is important to identify responders and nonresponders [Anderson and Macnee, 2009; Miravitlles, 2011]. In patients with COPD, ICS are effective in treatment [Davies et al. 1999] and prevention [Burge et al. 2000; Paggiaro et al. 1998] of exacerbations. Corticosteroids appear to have a selective inhibitory effect on eosinophilic airway inflammation in patients with COPD [Brightling et al. 2000, 2005]. Despite broad anti-inflammatory effects, ICS do not achieve marked long-term effects on slowing lung function decline in the majority of patients with COPD [Glaab and Taube, 2011; Telenga et al. 2010]. In asthma, treatment aimed to minimize eosinophilic inflammation significantly reduces severe exacerbations (by 68%) and hospitalizations [Green et al. 2002]. Also, in COPD a treatment strategy aimed to minimize eosinophilic inflammation and symptoms results in a significant reduction of exacerbations that require hospitalization, mainly in patients with COPD and eosinophilic airway inflammation at baseline (>3% sputum eosinophils) and sometimes requiring long-term oral corticosteroids. No difference was seen for milder exacerbations that require general practitioner visits only [McDonald et al. 2013; Siva et al. 2007]. Since eosinophilic inflammation has not been repeatedly shown as a distinguisher of ACOS compared with COPD and asthma alone, treatment aimed to reduce eosinophilic inflammation should therefore be performed in patients with proven eosinophilic inflammation instead of in groups assumed to have eosinophilic inflammation.
Long-acting bronchodilators
Thus far, the only placebo-controlled study in ACOS has shown that once daily tiotropium bromide significantly improved FEV1, peak expiratory flow rates and decreased use of rescue medication [Magnussen et al. 2008]. So far, no further clinical studies on long-acting anticholinergics or β sympathomimetics have been performed. However, since reversibility is not constantly different between ACOS and COPD or asthma alone (Table 2), future studies should focus on reversibility of chronic airflow obstruction and hyperinflation regardless of underlying phenotype.
Newly developed specific antieosinophil therapies (anti IL-5, IL-13, IL-33 antibodies) and treatments specifically targeting neutrophils (macrolides, cytokine receptor CXCR2 antagonists, phosphodiesterase type 4 (PD4) inhibitors, p38 mitogen-activated protein (MAP) kinase inhibitors, anti IL-1 and IL-17 antibodies) might be of relevance, especially for patients with ACOS [Barnes, 2015; Reddel, 2015].
Comorbidities
From a cluster analysis in patients with COPD (>40 years, prebronchodilator FEV1 > 50% predicted, FEV1/FVC > 0.7, more than one exacerbation in previous year) three clusters of patients were identified. One of these clusters was ‘patients using diuretics’, suggesting underlying cardiovascular disease [Disantostefano et al. 2013]. In the EPI-SCAN study a higher comorbidity index was seen in patients with ACOS compared with those with COPD alone. No other studies found higher rates of comorbidities in patients with ACOS.
Prognosis
In the EPISCAN study an increase in the St. George’s Respiratory Questionnaire (SGRQ) score of 11 points was found in the overlap group [Miravitlles et al. 2013] compared with the COPD alone group. An increase of 4 points has pre-viously been associated with a 5% increase in overall risk of mortality and 13% in respiratory mortality [Domingo-Salvany et al. 2002]. Also more airway complications needing oral steroids, antibiotics or hospitalizations were seen in patients with ACOS compared with those with asthma and COPD alone [De Marco et al. 2007; Gibson and Simpson, 2009]. In a large study on self-reported asthma or COPD, the combination of self-reported asthma and COPD was associated with increased overall mortality [Diaz-Guzman et al. 2011].
Conclusion
Asthma and COPD are different diseases. They are both clinical diagnoses, with diagnostic tools to discriminate between them. However, especially in older patients (> 55 years), it seems more difficult to differentiate between asthma and COPD. This has led to the definition of a new phenotype called ACOS. However, as is stated in the joint document of GINA and GOLD on asthma COPD overlap syndrome [GINA-GOLD, 2015], our understanding of ACOS is at a very preliminary stage, as most research has involved subjects with existing diagnoses of asthma or COPD from studies with different definitions for ACOS. In this review we have summarized specific features examined in studies on ACOS. For most of these features different, and sometimes even opposing, results have been found between studies, especially if more studies regarding the same features were performed.
We therefore suggest not using the term ACOS for a patient with features of both asthma and COPD, but to describe a patient with chronic obstructive airway disease as completely as possible, with regard to characteristics that determine treatment response (e.g. eosinophilic inflammation) and prognosis (such as smoking status, exacerbation rate, fixed airflow limitation, hyperresponsiveness, comorbidities). This will provide a far more clinically relevant diagnosis, and would aid in research on treatment in more homogenous groups of patients with chronic airways obstruction. More research is certainly needed to develop more evidence-based definitions for this patient group and to evaluate biomarkers, which will help to further classify these patients, treat them more adequately and unravel the underlying pathophysiological mechanism.
Footnotes
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: A. Slats declares no conflict of interest, C Taube is a consultant for Boehringer Ingelheim, GlaxoSmithKline, Novartis, TEVA, Chiesi and AstraZeneca.