
Abstract
Objectives:
Acute viral respiratory illnesses are associated with acquisition of Pseudomonas aeruginosa infection in cystic fibrosis (CF) patients. This study aimed to pilot a protocol for a randomized controlled trial to determine whether oral antipseudomonal antibiotics used at the onset of such episodes might delay onset of infection with this organism.
Methods:
A total of 41 children with CF aged 2–14 years, without chronic Pseudomonas infection, were randomized to receive ciprofloxacin (n = 28) or placebo (n = 13) at the onset of acute viral respiratory infections on an intention to treat basis, during a study period of up to 32 months.
Results:
There were no unexpected adverse events believed related to the use of the study medication. The rate of withdrawal from the study was low (approximately 7%) and did not differ between groups. Randomization was effective and acceptable to participants. Primary and secondary outcome measures all favoured active treatment, but there were no significant between group differences. The median rate of Pseudomonas isolates was 0/patient/year (interquartile range 0–0.38) in both the active and placebo groups. Kaplan–Meier survival curves showed no significant difference in time to first Pseudomonas isolate between groups.
Conclusions:
This study demonstrated the clinical feasibility of using oral ciprofloxacin in CF patients at times of viral infection. Within this sample size, no significant association was found between active treatment and decreased growth of Pseudomonas in follow-up microbiological samples. A definitive study would require at least 320 children to demonstrate significant differences in the rate of pseudomonal isolates.
Introduction
Cystic fibrosis (CF) disease-related morbidity and mortality are most commonly a result of progressive lung disease. This is characterized by a self-perpetuating cycle of bacterial infection and airway inflammation [Koehler et al. 2004]. Studies have characterized the involvement of a range of bacterial, viral and fungal species in the pathogenesis of CF lung disease [Rogers et al. 2003], but Pseudomonas aeruginosa remains the most common organism causing chronic endobronchial infection associated with deteriorating respiratory health.
Current concepts of care include the early use of antipseudomonal antibiotics after the initial detection of P. aeruginosa in respiratory samples [Tacetti et al. 2012; Gibson et al. 2007]. This approach has been successful in temporarily eradicating P. aeruginosa and thus delaying the onset of chronic infection, but eradication attempts typically become less successful over time and most patients eventually become chronically infected [Spilker et al. 2004]. Preventive strategies using regular inhaled antipseudomonal antibiotics [Tramper-Stranders et al. 2010] and routine bronchial lavage sampling to improve early identification and treatment of P. aeruginosa infection [Wainwright et al. 2011] have not been shown to be effective.
Laboratory studies have characterized the synergistic role of viruses as co-infecting respiratory pathogens predisposing to the onset of infection with P. aeruginosa [Avadhanula et al. 2006; van Ewijk et al. 2007]. In a prospective study of 38 children with CF, for six of the seven children in whom P. aeruginosa was first isolated during the study period, first isolates of P. aeruginosa were identified during, or within 3 weeks of, a viral upper respiratory tract infection [Collinson et al. 1996]. More recently, during 1 winter period, six of 20 prospectively studied children with CF (age range 0.1–7.4 years) had at least one P. aeruginosa positive culture from specimens collected at the time of acute viral respiratory infection [van Ewijk et al. 2006]. Initial onset of pseudomonal infections have been shown to have a seasonal pattern of occurrence temporally related to winter months when viral infections with pathogens such as RSV and influenza are more common [Johansen and Hoiby, 1992; Abman et al. 1988; Oritz et al. 2010; Smyth et al. 1995].
These data suggest that, for individuals with CF, episodes of viral respiratory tract infection might increase the risk of infection with P. aeruginosa during or immediately following these episodes. However, there are no randomized controlled trials of antipseudomonal prophylaxis during viral infections. We investigated the feasibility of using a randomized controlled trial protocol to investigate the hypothesis that the oral antipseudomonal antibiotic ciprofloxacin, used at the onset of viral upper respiratory tract symptoms, can prevent the subsequent growth of P. aeruginosa from follow-up respiratory tract cultures.
Patients and methods
Following UK NHS Ethics Approval (08/H0504/110), all children aged 2–14 years with a confirmed diagnosis of CF and attending either the regional CF service for full care or shared care with one of two referral hospitals were screened for study inclusion. Those with negative Pseudomonas enzyme-linked immunosorbent assay (ELISA) serology and judged not to be chronically infected with P. aeruginosa [Lee et al. 2003] or any other Gram-negative organism, and who had not received regular antipseudomonal antibiotics in the previous 6 months, were invited to participate. A recruitment period of 12 months was chosen to determine a recruitment rate independent of seasonal effects. Parents of all participating children gave informed written consent and children aged over 11 years were asked to provide written assent.
Children were randomized in blocks of nine (six active versus three placebo; Figure 1). Restricted randomization was used with stratification by clinic in a double-blind manner. Participants received ciprofloxacin syrup or placebo treatment for viral infections for 32 months or until study end if this was sooner. Very low rates of infective episodes were reported during late spring and summer months, and for this reason the study was stopped earlier than had originally been planned and before all study participants had been followed up for 32 months. The first patient was recruited into the study in December 2009 and the last in January 2011; the study ended in March 2013.

Flow diagram of study participants (Consort 2010).
Parents were instructed to contact the CF research nurses if their child experienced symptoms suggestive of acute viral respiratory illness including a runny nose, nasal congestion, sore throat and sneezing with or without fever. Parents also received fortnightly reminder texts from the research nurse to make contact in the event of these symptoms. When acute symptoms were reported, within 48 hours these were verified by the research team and the participant given, according to randomization group, a 2 week course of either ciprofloxacin syrup (Bayer plc; dose according to the British National Formulary for Children 20 mg/kg/day twice daily aged >5 years; 15 mg/kg/day twice daily age 2–5 years) or a placebo of the syrup suspension alone prepared by the clinical trial pharmacy at University Hospital Southampton NHS Foundation Trust. If cough persisted for more than 48 hours, children were assessed and treated with additional oral antibiotics by the CF clinical team according to regional protocols.
Microbiological specimens were obtained at outpatient clinic visits every 2 months and when clinically indicated. Separate to the study procedures, all positive isolates of P. aeruginosa were treated according to local clinical guidelines with 3 months inhaled colomycin plus oral ciprofloxacin (3 weeks for first isolates and 3 months for subsequent isolates) or a combination of two intravenous antibiotics. Study medication was discontinued during these treatment periods. Children who became chronically infected with P. aeruginosa were no longer eligible for inclusion in the trial.
The predetermined primary clinical outcome was the annual rate of positive isolates of P. aeruginosa. Secondary outcome measures included time to first detection of P. aeruginosa, change in pseudomonal serology, and annual rates of nebulized and intravenous antibiotic prescription.
Statistical considerations
All data were analysed on an intention to treat basis. We aimed to recruit 45 children into the study and used a 2:1 asymmetrical study design favouring active treatment to maximize safety and efficacy data for the study intervention. Based on published epidemiological studies [Kosorok et al. 2001] and review of PortCF data, we anticipated that P. aeruginosa would be detected in approximately one third of the control group. The number of children becoming chronically infected, according to the definition of >50% of samples positive for Pseudomonas over 12 months, was anticipated to be small [Lee et al. 2003]. However, the overall isolation rate was judged to be a clinically significant outcome of direct relevance to chronic colonization. Given the absence of trial data relating to antipseudomonal prophylaxis during viral infection, the likely size of any between-group difference in overall isolation rate was unknown. This study was designed to provide important safety and feasibility data for this treatment approach, and to inform the design and sample size of further trials in this age group.
Many of the outcomes were positively skewed, so nonparametric tests were used for between group comparisons. Bonferroni correction was considered overconservative as the analyses were designed a priori to test a limited number of hypotheses and not all the tests were independent [Bland, 2000]. We focused our interest on results with p < 0.05 and considered consistency of the findings in our interpretation. Stata® 11 (Stata Corp., College Station, TX, USA) was used for all analyses.
Results
A total of 41 children were randomized (Figure 1) [Schulz et al. 2010]; 26 completed 32 months, three were withdrawn (7%) and 12 (six active treatment and six placebo group) had completed less than 32 months (26–31 months) at study end. A total of two children withdrew from the intervention group, after 22 and 28 months, respectively, due to their families relocating out of region and 1 was withdrawn from the placebo group after 8 months because they were commenced on long-term nebulized antibiotics for clinical indications. There were no withdrawals attributable to no longer wishing to take the study medication or due to dissatisfaction with any other element of the study protocol. Withdrawal rate did not differ between groups. At recruitment, there were no significant between group differences in demographic or clinical features (Table 1). Participants did not demonstrate a better than chance ability to guess their group allocation.
Comparison of baseline data between intervention and placebo groups.

Binary outcomes were compared by Fisher’s exact test, categorical outcomes by a χ2 test for trend, and continuous variables using rank sum test.
ELISA, enzyme-linked immunosorbent assay; FEV1, forced expiratory volume in 1 second; IQR, interquartile range; SDS standard deviation score (Z-score).
The median number of occasions when a child was judged to require study medication was two in both groups. A total of 12 children in the placebo group received at least 1 course of oral ciprofloxacin during the study period. These individuals each received between one and eight courses. Despite this, the total number of courses of ciprofloxacin prescribed according to the study protocol, combined with those prescribed at the discretion of the clinical care team, was significantly higher in the treatment group (p = 0.0002). Each child in the active treatment group received between 1 and 11 courses (Table 1).
A total of 946 samples were collected during the study period of which 22 (2.3%) yielded positive cultures for P. aeruginosa. Although there was an almost 50% reduction in the mean annual rate of P. aeruginosa isolates (0.17 versus 0.30), this difference was not significant (Table 2). A total of nine of the 28 children in the active treatment group (32%) had at least one positive isolate of P. aeruginosa. For seven children, this occurred on one occasion. One child had two positive isolates and one child had positive isolates on three occasions. A total of six out of 13 children receiving placebo (46%) had at least one positive isolate of P. aeruginosa, 1 child isolated P. aeruginosa on five occasions and five children had one positive isolate each. A post hoc power calculation based on the annual rates of Pseudomonas isolates estimated that 80% power would require approximately 300 participants. Therefore to account for a withdrawal rate of approximately 7%, at least 320 children would need to be recruited.
Outcome data (1): between group comparisons of rate of pseudomonas isolates, treatment, ELISA serology, growth and lung function.
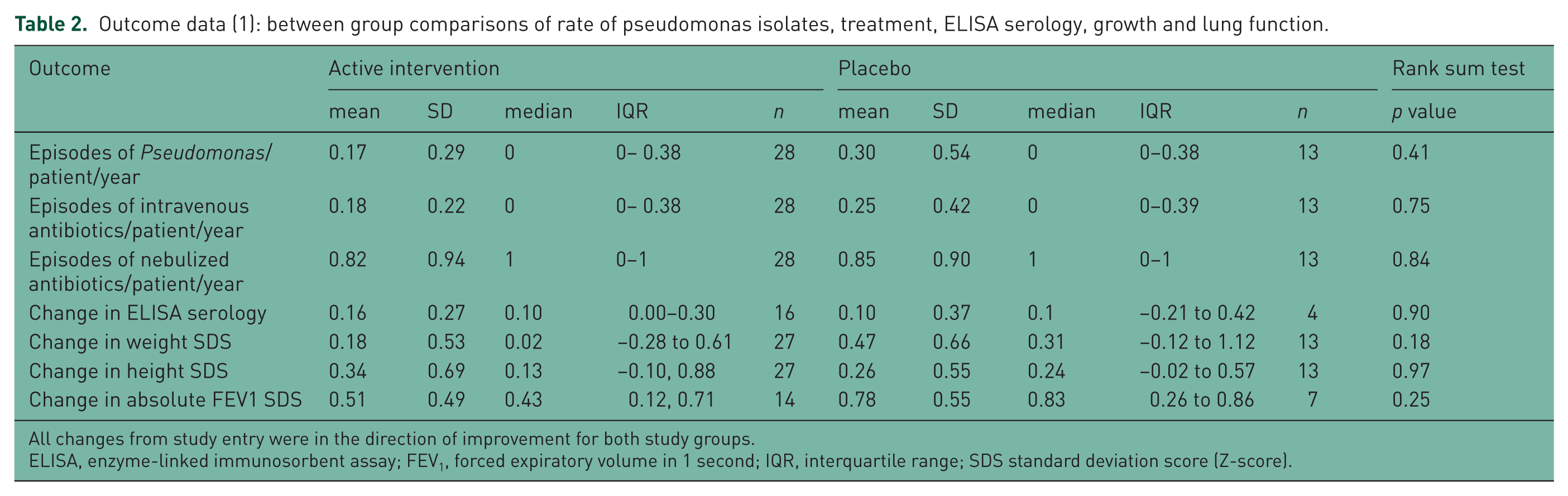
All changes from study entry were in the direction of improvement for both study groups.
ELISA, enzyme-linked immunosorbent assay; FEV1, forced expiratory volume in 1 second; IQR, interquartile range; SDS standard deviation score (Z-score).
The number of episodes of intravenous or nebulized antibiotic usage did not differ between active treatment and placebo groups, and there were no between group differences in ELISA serology (Table 2). Although the time to first P. aeruginosa isolate was shorter in the placebo group, this difference was not significant (p = 0.1) (Figure 2).

Kaplan–Meier survival estimate: time to Pseudomonas isolation.
There were no between-group differences in the rate of isolation of any other microbial or fungal species (Table 3). Median weight, height and forced expiratory volume in 1 second (FEV1) standard deviation (SD) scores all improved between the beginning and end of the study period, and there were no significant between-group differences. There were no cases of allergic bronchopulmonary aspergillosis, and no reports of arthropathy or any other significant side effects in relation to the use of ciprofloxacin or placebo.
Outcome data (2): between group comparisons of rate of isolation of other bacterial isolates.
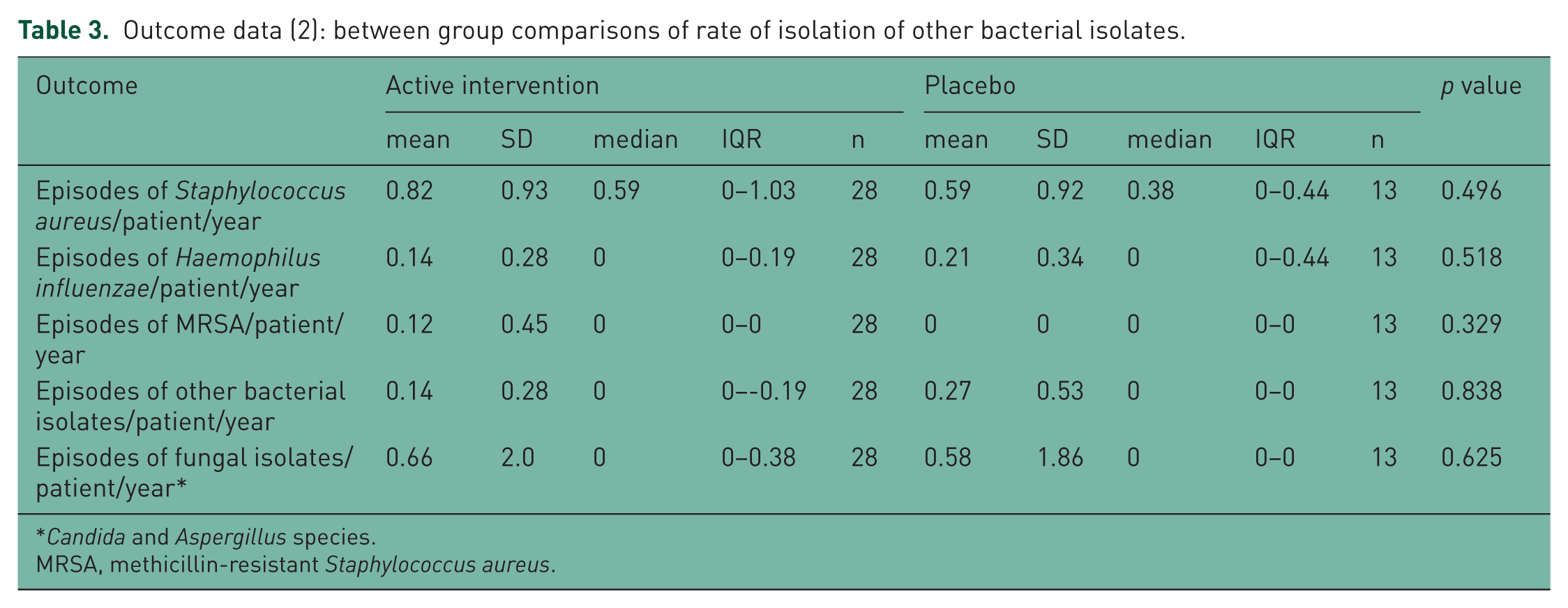
Candida and Aspergillus species.
MRSA, methicillin-resistant Staphylococcus aureus.
Discussion
This study provides data about the safe use of 2- week courses of oral ciprofloxacin at times of acute respiratory infection in children 2 years of age or older who are not yet chronically infected with P. aeruginosa. Within this pilot study, there was no significant between-group difference in the annual rate of P. aeruginosa isolates. Time to first P. aeruginosa isolate was shorter in the placebo group; this difference was nonsignificant, but the power may have been affected by disproportionate right censoring of placebo group data due to early termination of the study.
The study was designed as a pilot and unlikely to have sufficient power to detect a significant difference between groups for any outcome. It is possible, however, that the strong seasonal association found in epidemiological studies [Johansen and Hoiby, 1992] between P. aeruginosa infection and respiratory virus infections might not reflect direct facilitation of P. aeruginosa infection at the time of viral infection. Postviral effects, such as mucus gland hypertrophy, might play a role in the seasonal associations reported. The study design might therefore have failed to find a significant between-group difference because the period of antibiotic cover was insufficient. Nevertheless, animal model data demonstrate a facilitating effect upon pseudomonal infection during early viral infection, which supports investigation of this hypothesis in humans.[de Vrankrijker et al. 2009]
An important finding of relevance to proceeding to a definitive study was that the overall number of P. aeruginosa isolates in the control group was higher than anticipated, probably reflecting the intensity of microbial surveillance during the study. Despite this, only 1 child receiving placebo became chronically infected with P. aeruginosa and ELISA serology remained <1.00 (not indicative of chronic infection) in all study participants. Up to 11 courses of ciprofloxacin were prescribed to participants in the treatment arm of the study. An important clinical consideration is to weigh reduction of this relatively rare event against possible adverse drug effects or effects upon the microbiome of frequent broad spectrum oral antibiotic administration. The 2:1 randomization design enabled adverse effect data to be collected from a greater number of individuals than a 1:1 design without sacrificing significant power. Given the concerns associated with ciprofloxacin use in children and bone health, we would suggest any definitive study should also consider 2:1 randomization.
One concern about the increased use of ciprofloxacin in young children is the emergence of resistant opportunistic airway pathogens. Our results showed no between-group differences in the annual rate of Staphylococcus aureus isolates or any other known CF pathogens. These results must be interpreted with caution, however, in the absence of sufficient power to detect difference in pathogen isolation. One child in the active intervention group who grew methicillin-resistant Staphylococcus aureus (MRSA) had grown this organism intermittently prior to study entry, as had one of two children who grew atypical mycobacterial species. Close surveillance for changes in the occurrence of other bacterial pathogens would be an important part of similar future studies.
The study was subject to several limitations. The underlying rate of reported acute upper respiratory tract episodes was much lower than anticipated and varied widely between patients [Ramsey et al. 1989]. In particular, very low rates of infective episodes were reported during late spring and summer months, and for this reason, the study was stopped earlier than had originally been planned and before all study participants had been followed up for 32 months. It is possible that subclinical viral infections were not detected limiting the efficacy of the active treatment. Equally, efficacy might have been improved by rapid diagnostic testing during viral infections to identify infective agents since the risk of pseudomonal infection may reflect the causative virus, respiratory syncytial virus and influenza being particularly implicated in increasing the risk.[van Ewijk et al. 2007; Ramphal et al. 1990]. An unanticipated limitation was that the prescribing of ciprofloxacin as a treatment for respiratory symptoms during the study was higher than anticipated. Our current recommendations are for this to be used as a second-line agent for 2 week courses in children with ongoing cough, poorly responsive to first-line therapies empirically treating Staphylococcus aureus and Haemophilus influenzae. We believe this additional ciprofloxacin prescribing resulted from the CF clinical team and participating families being aware of the information that formed the basis of the study hypothesis, resulting in a lower threshold for ciprofloxacin use in routine clinical practice. This was highlighted and feedback to the clinical team by the trial’s independent data safety monitor.
In general, the clinical diagnosis of upper respiratory tract infection was felt to be accurate. For example, parents were questioned about seasonality of symptoms and contact with other symptomatic individuals in order to distinguish allergic rhinitis from symptoms more suggestive of infective episodes. Nevertheless, viral testing would have both confirmed diagnosis and provided the added advantage of identifying the causative viral agent. Many participants reporting episodes had accompanying cough at the time of initial presentation and the study protocol did not permit the use of study medication for these episodes, which were treated according to recommended guidelines [Wagener et al. 2013]. A better study design might be to treat such episodes with study medication in addition to first-line antibiotics.
Cough swabs were the most commonly used microbial sample in this study, with very few study participants able to expectorate sputum. The sensitivity of these specimens probably underestimates the true rate of infection, but this was partly offset by very frequent sampling at least every 2 months and at times of acute coughing for more than 2–3 days. The negative ELISA assays provided further reassurances that the overall Pseudomonas bacterial load was low.
The optimal approach to treating initial isolates of P. aeruginosa in CF remains unclear and is the subject of ongoing clinical trials [Langton Hewer et al. 2009]. Whilst continuous prevention treatment has not been shown to be effective in preventing Pseudomonas infection, a more targeted use of antipseudomonal antibiotics at times of acute viral illness might be a more effective strategy. On the basis of our data, a larger multicentre clinical trial recruiting at least 320 patients would be needed to further explore this hypothesis.
Footnotes
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was funded by Sparks (![]() ), supported by the Southampton NIHR Wellcome Trust Clinical Research Facility, NIHR Respiratory Biomedical Research Units, and managed by a Trial Steering Committee comprising Professor Graham Roberts (Chair), Dr Jane Lucas (Vice Chair) Judi Maddison (CF nurse specialist), Michelle Casey (Senior Research Sister), Amanda Harris (Lead Study Nurse), Mrs Carol Quiney (lay representative) and Drs Connett and Legg. Independent data safety monitoring was performed by Dr Amanda Bevan PhD (CF Pharmacist). Dr Simon Rees assisted in the preparation of the study protocol. The funders did not contribute to study design, collection or analysis of data or writing or publication of the report.
), supported by the Southampton NIHR Wellcome Trust Clinical Research Facility, NIHR Respiratory Biomedical Research Units, and managed by a Trial Steering Committee comprising Professor Graham Roberts (Chair), Dr Jane Lucas (Vice Chair) Judi Maddison (CF nurse specialist), Michelle Casey (Senior Research Sister), Amanda Harris (Lead Study Nurse), Mrs Carol Quiney (lay representative) and Drs Connett and Legg. Independent data safety monitoring was performed by Dr Amanda Bevan PhD (CF Pharmacist). Dr Simon Rees assisted in the preparation of the study protocol. The funders did not contribute to study design, collection or analysis of data or writing or publication of the report.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.