
Abstract
Nonadherence to inhaled therapies is a major problem in the treatment of cystic fibrosis that can influence lung function and health outcomes. Potential contributors to nonadherence have been identified, including demographic and psychosocial factors, time and convenience of inhaled therapy, and treatment beliefs. Additional research is clearly needed to clarify the contributors and to determine which interventions and technological advances will enhance adherence to inhaled therapies in patients with cystic fibrosis. Nurses and allied health professionals are ideally positioned to assist patients and families with adherence to inhaled therapies through monitoring, communication, and education about the available therapies and their proper use. This review briefly summarizes the available evidence about contributors to nonadherence, potential interventions, novel delivery devices for inhaled therapies, and opportunities for additional research.
Scope of the problem
Cystic fibrosis (CF) is a chronic progressive genetic disease that affects primarily the respiratory and digestive systems. For the majority of patients, respiratory treatments can occupy hours every day [Hunter, 2003] and pancreatic enzymes must be taken with all food to aid in digestion. The treatment burden of this disease often leads to missed doses and therapies; therefore, nonadherence to CF therapy has long been recognized as a major problem [Lask, 1994]. The research of treatment adherence in CF is a high priority in nursing and allied health professions. In one survey, it received the highest ranking for all research priorities in CF [Bradley et al. 2012].
Compliance, persistence, and adherence are related, but different, terms. Compliance generally refers to the extent that a patient ‘complies’ with the prescribed treatment. Persistence refers to the extent that a patient ‘persists’ with the treatment over a given period. Adherence refers to the extent that a patient has ‘adhered’ to the prescribed therapy over a given period, and thus it usually considers both compliance and persistence. Adherence in CF varies by the specific treatment and is difficult to accurately measure. Patients are more likely to be adherent to enzyme therapy or exercise than they are to be adherent to vitamin therapy or airway clearance [Abbott et al. 1996]. Patients also tend to overestimate adherence. In a study of children with CF, parents and patients each reported approximately 90% adherence to enzyme therapy, but the actual adherence rate from electronic monitoring was only 43% [Modi et al. 2006]. In a study of adults with CF, median self-reported adherence to nebulized treatments was 80%, but data downloaded from an electronic nebulizer monitor revealed median adherence of only 36% [Daniels et al. 2011].
Patients are also more likely to be adherent to simpler therapies, such as oral medications, than they are to more burdensome time-consuming therapies, such as nebulization treatments and airway clearance techniques [Chappell and Williams, 2002; Abbott et al. 2009]. Although a majority (57%) of patients with CF who are prescribed a nebulized antibiotic use it at least once daily, only 32% are fully adherent to the prescribed treatment of two to three times a day [Latchford et al. 2009]. Clearly there is a need for additional efforts to understand and address the factors that contribute to poor adherence to inhaled therapies in patients with CF.
Adherence and outcomes
Adherence to standard CF therapies is known to improve lung function. A study dating back to 1993 demonstrated that compliance with airway clearance and routine clinic visits is associated with better forced expiratory volume in 1 second (FEV1) trends [Patterson et al. 1993]. Other studies have correlated outcomes in patients with CF, such as reduced need for intravenous antibiotic therapy, with adherence to inhaled medications [Eakin et al. 2011]. In controlled clinical studies [Fuchs et al. 1994; Quan et al. 2001; Konstan et al. 2011b], dornase alpha treatment reduced respiratory exacerbations compared with placebo or standard care, but in an adherence study conducted by Nasr and colleagues in 2013, increase adherence to dornase alpha treatment did not reduce respiratory exacerbations significantly [Nasr et al. 2013]. This study did show that adherence to dornase alpha leads to a shorter length of hospital stay. High adherence with tobramycin inhalation solution, defined as at least four cycles per year where each cycle includes 28 days on and 28 days off therapy, is associated with a decreased risk of hospitalization and lower outpatient service costs compared with low adherence, or two or fewer cycles per year [Briesacher et al. 2011]. Thus, it is likely that patients will experience better FEV1 outcomes with increased adherence to prescribed inhaled therapies. Identifying and addressing factors affecting adherence could lead to better health outcomes for the CF population.
Demographic and psychosocial factors
Numerous factors may contribute to medication nonadherence in pediatric patients [Modi et al. 2012], and this does not improve as the patient ages. Unfortunately, patients with CF become less adherent as they get older [Masterson et al. 2011], and by the time they are over 15 years of age they are approximately three times as likely as younger children to be noncompliant (69% versus 24%) [Arias Llorente et al. 2008]. This is often the time when care responsibilities are transitioned from parent to young adult, which may be a contributing factor to this decrease in adherence [Williams et al. 2007; Modi et al. 2008; Van Staa et al. 2011]. Gender may or may not affect adherence. Some research suggests that adolescent girls are less adherent to CF treatment than adolescent boys [Patterson et al. 2008], while other research has not found an effect of gender on adherence to CF treatment [Masterson et al. 2011].
Studies also are inconclusive about psychological associations with adherence in CF. In one study, optimistic acceptance and hopefulness were associated with greater treatment adherence in CF [Abbott et al. 2001]. Conversely, other studies conclude that patients who worry about their condition have greater adherence [Abbott et al. 1996] and children with an anxiety disorder are more likely to be adherent to CF treatment [White et al. 2009]. Data are inadequate to identify direct causality between psychological factors and adherence. However, poor psychological wellbeing can be harmful to physical wellbeing and affect disease progression [Abbott et al. 2001]. Avoidance and denial worsen treatment adherence in CF; however, the reality of the disease and its progressive nature can be a motivating factor towards adherence. A balance between psychological wellbeing and disease progression should be the target for adherence strategies [Abbott et al. 1996]. Older children and adolescents in families experiencing unhappy and conflicted relationships are at greater risk of nonadherence to CF treatment [Delambo et al. 2004; White et al. 2009].
Collectively, these findings suggest that adherence may be optimized when patients have a healthy home environment in which they can balance worry about the negative consequences of nonadherence and hopefulness about the positive outcomes of adherence. A skilled CF care team that includes nurses and allied health professionals can delicately communicate the realistic potential of disease progression without causing increased anxiety. The CF care team is instrumental in assessing patient/family understanding of the CF disease process and the need for adherence to prescribed therapies, and should assess and identify psychosocial factors that may be affecting the ability of a patient to adhere to prescribed therapy. Referral to appropriate care providers or counseling should be made available to patients and families to assist with appropriate coping skills.
Time and convenience
The total treatment regimen for CF typically requires 2–3 hours each day [Sawicki and Tiddens, 2012], and nebulized inhaled medications are a key contributor to these lengthy treatments [Hunter, 2003]. Pulmonary treatment is complex in patients with CF, particularly as they age, and the complexity of treatment has only increased over time as new life-sustaining therapies have been developed and approved [Sawicki et al. 2013]. Adolescents and children with CF report that lack of time is a leading barrier for adherence to nebulized therapy [Modi and Quittner, 2006; Dziuban et al. 2010; Bregnballe et al. 2011]. However, adolescents are significantly more adherent to nebulized therapy on school days than on weekends or holidays, when they would be expected to have more free time [Ball et al. 2013]. A possible explanation is that adolescents forget to take treatments, which is another leading reason for nonadherence in this age group [Dziuban et al. 2010; Bregnballe et al. 2011]. People are more likely to forget to perform tasks when it is not part of their daily routine. Patients should be encouraged to identify and utilize various strategies for organization, such as written schedules, behavior modification charts, or electronic reminders, to help maintain their daily treatment regimen. The importance of time and convenience is reflected by higher reported rates of adherence to oral antibiotics (80–95%) than to nebulized medications (65–80%) [Abbott et al. 1994; Conway et al. 1996; Kettler et al. 2002]. Therefore, if daily therapies were less time consuming, patients would theoretically be more likely to adhere to the prescribed regimen.
Treatment beliefs
The Health Beliefs Model, in which patient perception of disease severity is associated with treatment adherence, may not apply in patients with CF [Abbott et al. 1996]. In contrast, patient beliefs about the utility of treatment (i.e. questioning the necessity of therapy) may have a substantial effect on adherence [Kreps et al. 2011]. Adolescents are less likely to use inhaled antibiotics if they question the necessity of the treatment [Bucks et al. 2009; George et al. 2010]. Many (30%) adolescents with CF report it is acceptable to miss treatments every few days or when they are busy [Dziuban et al. 2010]. In one study, patients stated they believed respiratory therapy is important (8.0 on a scale from 0 to 10) and 62% reported they were compliant with daily respiratory medications, but 15% of patients said they only took their respiratory medications when they felt worse [Arias Llorente et al. 2008]. As CF disease progresses, adolescent patients who perceive themselves to be less healthy may be particularly nonadherent during times of decreased symptoms [Dziuban et al. 2010]. Thus, patients need to be educated about the importance of preventive and suppressive treatment of Pseudomonas aeruginosa infection in CF [Davies and Bilton, 2009] instead of treating the symptoms. Many physicians are not convinced that inhaled treatments improve lung function and reduce exacerbations [Glauser et al. 2012]. If they convey these doubts to the patient, it could worsen nonadherence to inhaled antibiotic treatment.
The challenge faced by CF care teams is to effectively change patients’ belief systems so they appropriately see the effect of their daily treatment regimen on their long-term health outcomes. If a patient does not perceive the benefit of therapy to outweigh the risk, improving the convenience is unlikely to enhance treatment adherence [Abbott et al. 2009]. At each patient visit, the potential benefits of therapy and the importance of adherence should be reinforced.
Strategies to enhance adherence in cystic fibrosis
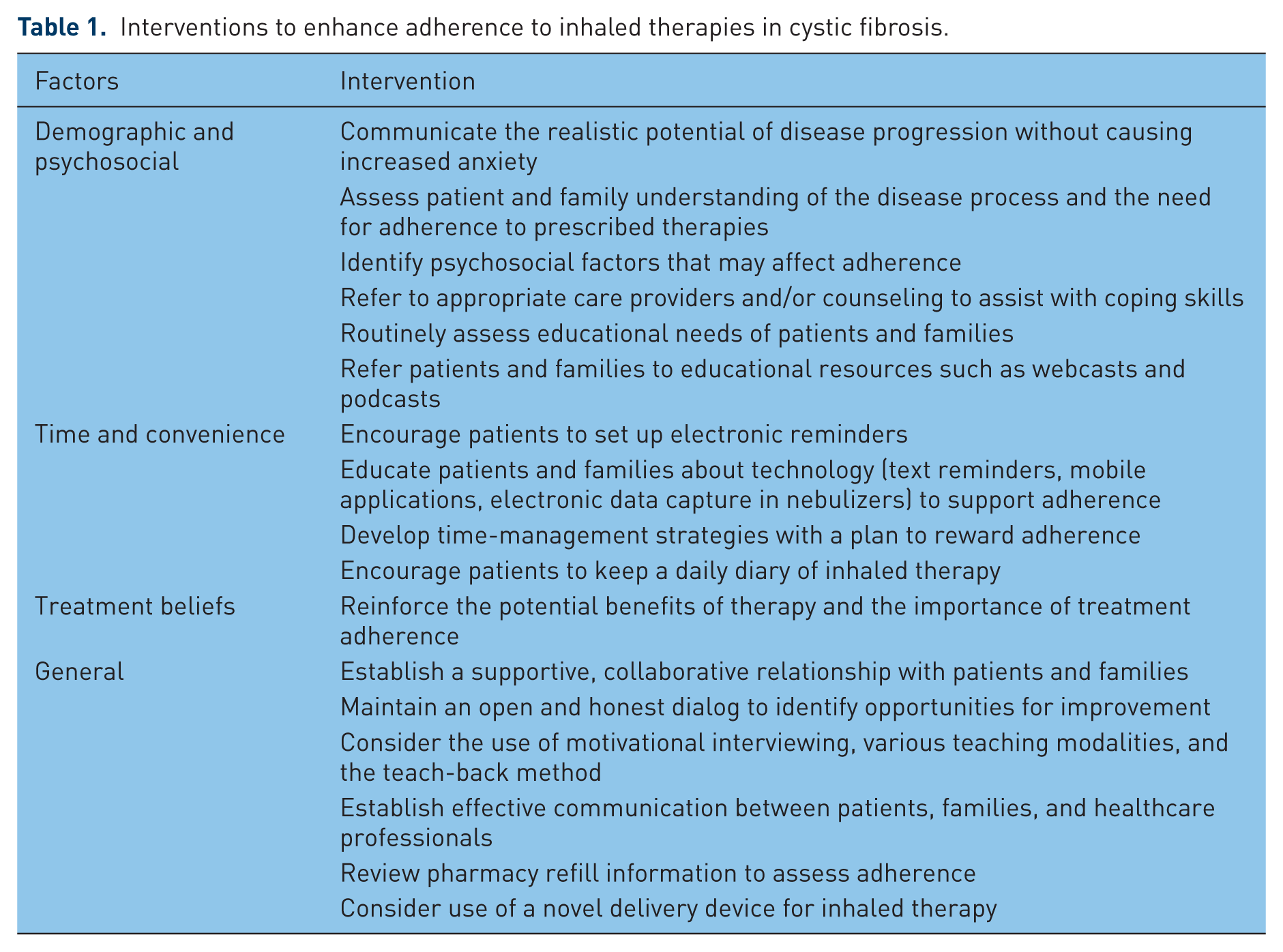
Opportunities for interventions to improve adherence to inhaled therapy in CF are summarized in Table 1. It is important to establish a supportive, collaborative relationship with patients and families to make it clear that when they report their adherence honestly and accurately, it helps improve their care and is not a time for them to be reprimanded. Open and honest dialogue may reveal barriers to nonadherence, such as financial, psychiatric, or social stressors that may require referral to an outside agency, psychologist, or team social worker for assistance.
Interventions to enhance adherence to inhaled therapies in cystic fibrosis.
Motivational interviewing should be considered [Duff and Latchford, 2010b]. It is a means to have a nonjudgmental conversation to coach patients to self identify areas they view as needing change. The patient is empowered to move from ambivalence to change with coaching. The four core counseling principles used in motivational interviewing are express empathy, support self-efficacy, roll with resistance, and develop discrepancy (www.motivationalinterviewing.org) [Levensky et al. 2007]. Conversations can bring the spirit of motivational interviewing to life by using open-ended questions, affirming the patient’s strengths, utilizing reflective listening, and recapping the discussion by summarizing important elements discussed. Healthcare professionals can begin the discussion by stating, ‘Completing all of your therapies every day is difficult. Which therapy are you most successful in accomplishing daily? With which therapy do you have the most difficulty? What would happen if you continue to miss your prescribed therapies?’ As the person with CF identifies their personal goals, motivational interviewing can lead them to realize behavior change is required to meet the goals they have set for themselves. Patients can move from nonadherence to adherence over time as they identify barriers and implement change ideas on their own.
Encouraging patients and families to keep a daily diary of inhaled therapy is often helpful and is a more accurate method than self reporting to measure adherence [Modi et al. 2006]. Patients can then bring that diary with them to the next visit to review and identify specific opportunities for improvement in adherence.
The CF care team should routinely assess the educational needs of their patients and family members. Many parents (up to 32%) of patients with CF have an incomplete understanding of their children’s treatments [Ievers et al. 1999]. Incomplete or incorrect information should be corrected using various verbal and visual teaching modalities, which could include educational brochures or links to online websites. The teach-back method [Kornburger et al. 2013] can be used to assess patient/family understanding of health-related information and instruction.
Educational programs significantly enhance patient adherence to respiratory therapy in CF [Downs et al. 2006]. Due to the infection prevention and control required for patients with CF, group educational meetings are not advisable. Instead, technology such as webcasts or podcasts is a way to safely educate a large number of patients. Patients and families can also reaccess the information if desired. The National Cystic Fibrosis Foundation has archived educational webcasts for patients and families at www.cff.org.
New technology, such as text reminders via cell phones specifically designed for patients with CF, may increase adherence in adolescents and children as young as 5 years of age [Marciel et al. 2010; Johnson et al. 2011]. Free downloadable applications are also available to remind patients with CF to take medications and track treatment adherence. Technology can also be used to monitor treatment adherence through electronic data capture in nebulizers [McNamara et al. 2009; Daniels et al. 2011; McCormack et al. 2012]. Nurses and allied health professionals can be instrumental in making patients aware of the technologies that are available and should encourage patients and parents to utilize appropriate tools.
Psychotherapeutic approaches and behavioral modification have been shown to enhance adherence to diet and airway clearance in patients with CF [Bernard and Cohen, 2004]. Behavioral modification may promote treatment adherence more effectively than education alone. In a meta-analysis of 70 psychological intervention studies to promote adherence among chronically ill youth [Kahana et al. 2008], educational interventions displayed a small effect size, whereas behavioral and multicomponent interventions had medium effect sizes. Fortunately, the average effect of interventions on treatment adherence was shown to be greater for pediatric patients with CF than for patients with other chronic pediatric conditions, such as asthma and diabetes [Kahana et al. 2008].
Establishing effective communication and interaction between patients, their families, and healthcare professionals may be a simple, yet effective, method to improve treatment adherence [Duff et al. 2010a, 2010b]. Healthcare providers often do not get an accurate representation of what patients are actually doing at home. In recent years, some pharmacies provided refill information to the prescribing care team, which may be a more accurate assessment of what medications patients are not taking as prescribed, but the potential for inaccuracy remains. Evaluation of refill information can be used as a starting point for assessing adherence barriers and spur discussion between healthcare professionals and their patients and families.
The general strategies described here to improve adherence are a good starting point, but it is important to identify the specific barriers to adherence in an individual patient with CF and then target the interventions to that patient’s needs [Abbott et al. 2009]. Information to identify barriers may be collected via personal interview or by survey. Nurses or other team members can then partner with the patient and families to develop time-management strategies with a plan to reward adherence. Strategies to improve adherence also need to be age appropriate and properly balanced between targeting the patient and their caregiver.
Novel delivery devices for inhaled therapies
Clinical guidelines recommend inhaled tobramycin therapy in patients aged 6 years or older with persistent P. aeruginosa infection [Flume et al. 2007]. Inhalation solutions approved for the management of P. aeruginosa in patients with CF in the USA include tobramycin and aztreonam lysine [Ballmann et al. 2011]. Until recently, clinical guidelines concluded that other inhaled antibiotics have less evidence than tobramycin inhalation solution to support their use in this setting [Flume et al. 2007; Ryan et al. 2011]. A recent study of inhaled aztreonam lysine by nebulizer three times daily reported that it improved lung function and reduced pulmonary exacerbations more effectively than tobramycin inhalation solution by nebulizer twice daily [Assael et al. 2013]. The 2013 update to CF pulmonary guidelines from the CF Foundation supported the use of either inhaled tobramycin or inhaled aztreonam lysine [Mogayzel et al. 2013].
Nebulizers for inhalation solutions can be time consuming, not only to administer the drug, but also to clean and prepare the nebulizer [Heijerman et al. 2009]. Technologies such as vibrating-mesh nebulizers, jet nebulizers, and ultrasonic nebulizers may shorten administration time [Heijerman et al. 2009; Coates et al. 2011; Daniels et al. 2013; Govoni et al. 2013], but not all nebulizers are approved for the administration of all inhaled medications. A nebulizer may have a faster delivery time, but the medication will not be delivered properly and thus does not have its optimal affect. Administration of inhaled antibiotics in a dry powder inhaler reduces the time required for administration as compared with nebulizers and is more convenient and portable [Geller and Madge, 2011; Parkins and Elborn, 2011]. A dry powder inhaler for tobramycin that was approved for use in patients with CF with P. aeruginosa infection is more effective than placebo and is not inferior to tobramycin inhaled solution [Geller et al. 2007; Konstan et al. 2011a; Galeva et al. 2013]. Although more rapid administration with a dry powder inhaler has been postulated to improve treatment adherence, this has not been studied directly. Additional research and development of other novel administration devices [Kesser and Geller, 2009; Hofmann, 2012], other antibiotics in dry powder inhalers [Schuster et al. 2013], and combinations of inhaled medications [Trapnell et al. 2012; Pilcer et al. 2013a, 2013b] are ongoing in an effort to enhance delivery of inhaled therapies and improve adherence.
In the course of ongoing communication with patients and families, if the nebulized administration of antibiotic therapy is determined to be likely to interfere with treatment adherence, use of a novel delivery device should be considered.
Conclusion
Despite widespread recognition that nonadherence is a major problem in CF treatment and emerging research about potential contributors to nonadherence, additional research is clearly needed to determine which interventions and technological advances will enhance adherence to inhaled therapies in patients with CF. In the meantime, nurses and allied health professionals are ideally positioned to assist patients with CF and their families with adherence to inhaled therapies, through monitoring, communication, and education about the available therapies and their proper use.
Footnotes
Acknowledgements
The author thanks Jonathan Latham of PharmaScribe, LLC for editorial assistance and styling of the manuscript for journal submission.
Funding
Novartis Pharmaceuticals Corporation (East Hanover, NJ) provided funding for the editorial assistance. The opinions expressed in this manuscript are those of the author. Novartis Pharmaceuticals Corporation had no influence on the contents of the manuscript.
Conflict of interest statement
The author declares that there is no conflict of interest.