
Abstract
Background:
The aim of this study was to describe the antibiotic prescribing rate in patients with acute exacerbation of chronic obstructive pulmonary disease (AECOPD), to analyse predictors for antibiotic prescribing and to explore the influence of the use C-reactive protein (CRP) rapid test.
Methods:
A cross-sectional study was carried out in January and February 2008 in primary care. General practitioners (GPs) from six countries (Denmark, Sweden, Lithuania, Russia, Spain and Argentina) registered all patients with AECOPD during a 3-week period. A multilevel logistic regression model was estimated using two hierarchical levels, (i) patients and (ii) physicians, and was used to analyse the association between antibiotic prescribing and potential predictors for antibiotic use: patients’ age and gender, duration and symptoms and signs of exacerbations (fever, cough, dyspnoea, sputum volume and purulence) and the results of the CRP test.
Results:
A total of 617 GPs registered 1233 patients with AECOPD. A total of 970 patients (79%) were prescribed antibiotics, varying from 49% (Denmark) to 93% (Russia). The presence of purulent sputum was the strongest predictor for antibiotic treatment (odds ratio [OR] 8.7; 95% confidence interval [CI] 5.9–12.8). CRP determination was carried out mainly in Denmark and Sweden and its use was the strongest protective factor for antibiotic therapy (OR 0.3; 95% CI 0.2-0.6). GPs that used CRP testing weighted purulent sputum lower than GPs who did not use CRP testing. CRP values had a strong influence on the antibiotic prescribing rate.
Conclusions:
Antibiotic treatment for AECOPD is very high. This study shows that GPs performing CRP rapid tests prescribe fewer antibiotics than those who do not.
Keywords
Introduction
Acute exacerbation of chronic obstructive pulmonary disease (AECOPD) is a common cause of consultation in general practice. Approximately 4% of the general population in Europe consults a general practitioner (GP) at least once a year for acute respiratory disease, and up to 20% of those visits are due to AECOPD [MacFarlane et al. 1993]. The effect of antibiotics in patients with AECOPD is limited and there is no consensus about the criteria to use them [Bach et al. 2001; Rohde, 2010]. Recent data suggest that approximately 70% of exacerbations are infectious in origin [Celli and Barnes, 2007] and viruses are considered as major triggers [Rohde et al. 2003]. However, the cause of exacerbations is often unidentifiable [Gruffydd-Jones and Loveridge, 2011].
Currently, there is no diagnostic test available for general practice that can reliably distinguish between bacterial, viral and other origins of AECOPD. Uncertainty about the infectious origin may lead to increased antibiotic prescribing [Gruffydd-Jones and Loveridge, 2011]. The Anthonisen criteria, increased dyspnoea, increased sputum volume and increased sputum purulence, have been used to identify patients that should be treated with antibiotics [Anthonisen et al. 1987]. International guidelines recommend that patients with two or more criteria should be prescribed an antibiotic [Global Initiative for Chronic Obstructive Lung Disease, 2011].
In order to reduce the inappropriate overprescribing of antibiotics several countries have initiated practice intervention programmes focusing on both professionals and patients [Arnold and Straus, 2005]. In 2007, the European Community awarded a grant to the project Health Alliance for Prudent Prescribing, Yield and Use of Anti-microbial Drugs in the Treatment of Respiratory Tract Infections (Happy Audit) with the aim of reducing inappropriate antibiotic use in patients with respiratory tract infections. In this paper we describe the findings about the antibiotic prescribing rate and type of antibiotic used in patients with AECOPD. In addition, we test the association of potential predictors for antibiotic prescribing and explore the influence of the use of C-reactive protein (CRP) rapid test on the prescribing.
Methods
A cross-sectional study was carried out in general practice in the winter months of 2008 in five European countries (Denmark, Spain, Sweden, Lithuania and Russia) and Argentina. The material and method for this study have been published elsewhere [Bjerrum et al. 2010]. Briefly, GPs from six countries registered all patients with respiratory tract infections during a 3-week period, covering a total of 15 work days. The data were registered according to the methodology of the Audit Project Odense (APO) described by Munck [Munck, 1995], which follows a prospective self-registry methodology. The following variables at patient level were registered: age, gender, number of days with symptoms, character of symptoms and signs, chest X-ray, result of CRP, assumed aetiology, and antibiotic treatment. Physicians were instructed not to use CRP as a standalone test but rather to use it as an additional test in case of doubt, withholding antibiotic therapy with CRP values < 20 mg/l and prescribing an antibiotic with values >100 mg/l. The CRP rapid test was also performed in capillary blood using Nycocard CRP® analyzers (Axis-Shield, Dundee, UK). This rapid test is feasible and easy to perform in the community setting since it takes approximately three minutes to obtain the result. Patients with AECOPD were identified by a worsening of symptoms beyond normal day-to-day variations. A type I exacerbation was defined by the occurrence of all three Anthonisen criteria. A type II exacerbation referred to a patient with two of these symptoms, while a type III exacerbation occurred when a patient had only one symptom [Anthonisen et al. 1987].
Data were analysed with the statistical program Stata v. 11. Chi-squared and Student’s t tests were used to compare proportions and means, respectively. A multilevel logistic regression model was estimated using two hierarchical levels: (i) patients and (ii) physicians. Statistical significance was considered if p value <0.05.
Results
A total of 617 GPs from six countries participated in the study. The GPs registered a total of 1233 patients with the diagnosis AECOPD. Table 1 shows the participation rate in the different countries. The mean age of the subjects was 64.5 ± 16 years and 722 (58.6%) were men. A chest X-ray was requested in 241 patients (19.5%), mainly in Russia (63.7%). CRP was performed in only 7.5% of all patients, most frequently in the Nordic countries, Denmark (65.6%) and Sweden (39.4%). The mean duration of symptoms was 6.3 ± 9 days. A total of 311 (25.2%) patients had a type I exacerbation, 478 (38.8%) a type II and 371 (30.1%) a type III.
Number of physicians participating in the Happy Audit study and number of patients with acute exacerbations of chronic obstructive pulmonary disease.

Bacterial aetiology was suspected in 883 (71.6%) patients. Antibiotics were prescribed in 970 (78.7%) patients with AECOPD, being higher in patients with type I exacerbations (94.2%), followed by those with type II (84.1%) and type III exacerbations (65.8%). A total of 73 patients did not have any Anthonisen criteria, but in spite of the lack of Anthonisen criteria 31 (42.5%) of these patients received an antibiotic prescription.
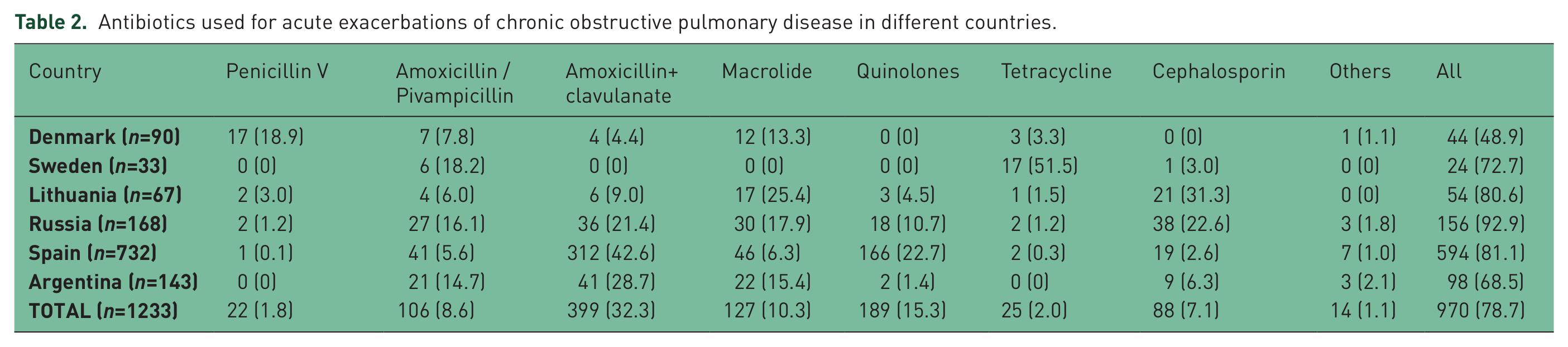
Table 2 shows prescribing rates for different antibiotics by countries. The highest prescribing rate was found in Russia (92.9%) followed by Spain (81.1%) and Lithuania (80.6%). Conversely, antibiotic therapy was only given to 48.9% of patients in Denmark. Overall, the most preferred antibiotics were amoxicillin and clavulanate followed by quinolones, even though the leading antibiotics were penicillin V in Denmark, cephalosporins in Lithuania and tetracyclines in Sweden.
Antibiotics used for acute exacerbations of chronic obstructive pulmonary disease in different countries.
Antibiotic prescribing rate was highest among GPs who did not use CRP testing (80.6%) compared with those who did (54.3%; p < 0.001). The signs and symptoms most frequently reported by the participants were increased cough (75.9%), increased sputum volume (69.9%) and increased dyspnoea (62.4%), purulent sputum (50.9%) and fever (28.6%). Antibiotic prescribing rate was higher in patients with purulent sputum (93.6%) than in patients without this sign (63.1%; p < 0.001). Correspondingly, patients with increase in sputum volume were prescribed more antibiotics (84.5%) than patients without increased sputum volume (65.2%; p < 0.001).
The strongest predictor for antibiotic prescribing was presence of purulent sputum (odds ratio [OR] 8.7) (Table 3). Use of CRP in the office was associated with a lower probability of antibiotic prescribing (OR 0.34). GPs who did not use point-of-care testing in the office weighted the clinical criteria more than GPs who made use of point-of-care tests. Thus, the OR for purulent sputum was reduced from 8.7 to 5.3 if the GP used CRP testing in the office. GPs that used CRP prescribed fewer antibiotics, mainly in patients with type II and III exacerbations. Furthermore, as shown in Figure 1, no patients without any of the Anthonisen criteria were given antibiotics among GPs who used CRP determination. The use of CRP in the office was the predictor exerting the greatest influence on antibiotic prescribing and the value of CRP had a strong influence on the probability of antibiotic prescribing (Figure 2).
Predictors for antibiotic prescribing in patients with acute exacerbations of chronic obstructive pulmonary disease.

Adjusted for all other potential predictors in multivariate logistic regression model

Antibiotic prescribing rates in patients with acute exacerbations of chronic obstructive pulmonary disease in relation to the number of Anthonisen criteria for general practitioners (GPs) that use C-reactive protein (CRP) testing in the office and GPs that do not use CRP testing.

Relationship between level of C-reactive protein and antibiotic prescribing rate in patients with acute exacerbation of chronic obstructive pulmonary disease (COPD).
Discussion
More than three quarters of patients with AECOPD from the Happy Audit project were prescribed antibiotics, and the prescribing rate is highest in patients with the presence of purulent sputum. In addition, GPs who do not use CRP rapid tests in their offices weighted clinical criteria higher and prescribed more antibiotics compared with GPs who used CRP testing as a supplement to the clinical examination.
The results of this study should be interpreted with caution because of a series of limitations. GPs participated on a voluntarily basis and their prescribing habits were probably different from other GPs in the same country. Studies have shown that GPs who participate in quality intervention initiatives may be more interested in research than other GPs [Lervy et al. 1994]. However, the reliability of the Audit Project Odense methodology demonstrated in different projects carried out in other European countries is very high and well correlated with the real prescription in the medical offices [Munck et al. 2003]. Another limitation which should be regarded in this type of study is the mere fact of performing an audit may influence the prescribing habits.
Another limitation is that we did not take comorbidity of patients into account, which may have influenced the prescribing rate and the type of antibiotics used. The template used by GPs included a limited number of items to make it easier for the physicians to appropriately fill all of the variables out. Other variables, such as smoking status or forced expiratory volume in 1 second, were not included in this template and were therefore not registered. The low number of patients in which a CRP rapid test was carried out could have had an impact in the interpretation of the predictors. CRP determination has been carried out for more than a decade in Scandinavian countries even though not all of the patients attended in Sweden and Denmark did actually undertake this test. Another weakness is the definition of COPD considered by GPs. However, prior to the onset of the study participating GPs were requested to include as COPD patients those who had a spirometric diagnosis. This fact might have explained why the mean number of patients per physician ranged from 0.4 to 4.3 depending on the country. Even though the mean number of COPD patients recruited per physician was low, we were able to recruit 1211 cases because of the high number of GPs participating in this study. Microbiological analysis was not assessed in our study because it is not readily available in primary care centres. Positive cultures are only obtained in 20–60% of sputum samples of patients included in clinical trials with types I and II exacerbations [Daniels et al. 2010; Wilson et al. 2012]. The GOLD guidelines recognize that sputum cultures take too long, at least 2 days, and frequently do not give reliable results for technical reasons [Global Initiative for Chronic Obstructive Lung Disease, 2011]. Thus, we wished to reflect clinical practice in which microbiological examinations are not routinely requested in ambulatory exacerbations of COPD.
Our goal is not just reducing the prescription of antibiotics for patients with AECOPD; instead we should give them to patients who may benefit from their utilization. Antibiotics are known to prevent adverse outcomes for some patients with lower respiratory tract infections [Winchester et al. 2009]. The outcome of the COPD patients included in our study was not measured, constituting another limitation of our study. Neither did we check whether patients treated with antibiotics actually took them or those treated without received them in other settings, such as pharmacies, still available in some of the participating countries. We only considered whether or not the GPs prescribed antibiotics in the consultation when a COPD patient was attended with an acute exacerbation. We know that the efficacy of antibiotics is well established in purulent exacerbations of severe COPD [Anthonisen et al. 1987] and recently our group demonstrated the efficacy of antibiotic treatment in purulent ambulatory exacerbations of mild to moderate COPD [Llor et al. 2012]. Furthermore, those treated with an antibiotic had a significantly prolonged time to the next exacerbation.
Notwithstanding, the use of antibiotics in this condition is excessive. One of the reasons for overprescribing of antibiotics may be the difficulty in distinguishing viral from bacterial aetiology based on only clinical criteria. This is reflected in this study as GPs who did not use CRP rapid tests were more liable to prescribe antibiotics if the patient presented signs and symptoms that indicated AECOPD, e.g. purulent sputum (OR 9.8). In fact, the change in the colour of the sputum seemed to be the key sign for identifying bacterial exacerbations in line with the study from Stockley and colleagues [Stockley et al. 2000]. On the other hand, antibiotic prescription was only 5.3-fold greater with the presence of purulence among physicians performing CRP.
The prescription of antibiotics observed in our study is slightly lower than the rates found in other similar studies. In two studies from the United States, antibiotics were prescribed to more than 80% of patients with AECOPD [Lindenauer et al. 2006; Gonzales et al. 2006] and in a study from Australia, the antibiotic prescribing rate reached 87% [Pretto et al. 2012]. Miravitlles and colleagues found that Spanish GPs prescribed antibiotics to 89% of patients with AECOPD [Miravitlles et al. 1999]. In a study carried out across five European countries, the antibiotic prescription in exacerbations of chronic bronchitis ranged between 74% (Germany) and 99% (Spain) [Huchon et al. 1996]. Percentages exceeding 80% have also been observed in the UK [Davey et al. 1994]. According to the medical literature, only those patients exhibiting types I or II exacerbations received demonstrable benefit from antimicrobial therapy, whereas those with a type III exacerbation did not differ from patients receiving placebo [Anthonisen et al. 1987]. Extrapolating these recommendations to our study means that antimicrobial treatment should have been administered in only 64% of the patients.
Very few studies have evaluated the role of CRP as an aid for the physician to make the decision about antibiotic treatment in patients with AECOPD. In a recent survey, normal CRP values were present in nearly 50% of patients admitted due to a COPD exacerbation [Weis and Almdal, 2006]. In patients who had increased sputum purulence, the pattern of increase in CRP was similar to that seen in patients with pneumonia, suggesting that CRP may be used as a marker of significant bacterial infection. The association of the sputum colour with elevated CRP levels has also been observed in other studies [Bircan et al. 2008].
To the best of the authors’ knowledge, this is the first study to demonstrate that GPs who have access to CRP rapid testing use the test result to guide antibiotic prescribing in patients with AECOPD. Another result of the present study was the great variation in antibiotic prescribing rates, first choice of antibiotics, and diagnostic procedures among the different participating countries, as have been observed in other studies [Bjerrum et al. 2004]. Perhaps, the results of our study could lead to the design of clinical trials in different countries which also consider this or other rapid tests.
In summary, this first registry of the Happy Audit study has provided valuable information on the use of antibiotics in AECOPD in different cultural contexts and traditions, etc. Point-of-care testing holds great promise in improving outcome for patients through better targeted treatment. This is particularly true in primary care where most patients receive treatment and where diagnostic options are often limited. AECOPD is a common, important condition that account for considerable health care resources and human suffering. According to the results obtained in this study, new pathways have been opened to implement strategies to achieve a more rational use of antibiotics at primary care level for AECOPD.
Footnotes
Acknowledgements
The authors of this study wish to thank the primary care physicians who participated in this study. We thank Angel Vila for the multilevel analysis.
Funding
This project is a Specific Targeted Research Project (STREP) funded by The European Commission: DG SANCO under the Frame Program 6 (contract number SP5A-CT-2007-044154).
Conflict of interest statement
The authors declare no conflicts of interest in preparing this article. Dr Llor reports receiving research grants from the European Commission (Sixth and Seventh Programme Frameworks), Catalan Society of Family Medicine, and Instituto de Salud Carlos III (Spanish Ministry of Health).