
Abstract
Asthma and gastroesophageal reflux disease (GERD) are both common conditions and, hence, they often coexist. However, asthmatics have been found to have a much greater prevalence of GERD symptoms than the general population. There remains debate regarding the underlying physiologic mechanism(s) of this relationship and whether treatment of GERD actually translates into improved asthma outcomes. Based on smaller trials with somewhat conflicting results regarding improved asthma control with treatment of GERD, current guidelines recommend a trial of GERD treatment for symptomatic asthmatics even without symptoms of GERD. However, recently a large multicenter trial demonstrated that the treatment of asymptomatic GERD with proton-pump inhibitors did not improve asthma control in terms of pulmonary function, rate of asthma exacerbations, asthma-related quality of life, or asthma symptom frequency. These data suggest empiric treatment of asymptomatic GERD in asthmatics is not a useful practice. This review article provides an overview of the epidemiology and pathophysiologic relationships between asthma and GERD as well as a summary of current data regarding links between treatment of GERD with asthma outcomes.
Introduction
Asthma and gastroesophageal reflux disease (GERD) are very common conditions that affect millions of patients. The prevalence of asthma is estimated to be approximately 20–25 million people in the United States [National Heart Lung and Blood Institute Expert Panel, 2007] and gastroesophageal reflux symptoms occur daily in approximately 10–20% of the US adult population [Dent et al. 2005]. Owing to the high prevalence rates of both diseases, one would expect many asthmatics would also have GERD. However, asthmatics have been found to have a much greater prevalence of GERD symptoms than the general population. Some studies that have utilized symptoms questionnaires have found nearly 80% of asthmatics may experience GERD symptoms such as heartburn, regurgitation, and/or swallowing difficulties. [Field et al. 1996] A large Veterans Administration study of over 100,000 veterans found that veterans with GERD were 1.15 times more likely to have asthma than veterans without GERD and several studies utilizing pH probe testing have found a prevalence of GERD among asthmatics of 30–65% [Mastronarde et al. 2009; Leggett et al. 2005; Kiljander and Laitinen, 2004; Harding et al. 1999; Sontag et al. 1990]. Thus, it appears that no matter which definition of GERD one uses, symptom based or objective testing, there is an increased prevalence of GERD among asthmatics. This has raised the question of whether GERD and asthma are just common diseases that overlap in patients or whether there is a pathophysiologic link between the two disease states.
Pathogenesis
There have been several theories put forth in an attempt to explain how GERD and asthma may be linked in a causal fashion.
Asthmatic patients often have lung hyperinflation. Descent of the diaphragm in the setting of lung hyperinflation and increased work of breathing increases the pressure gradient between the abdomen and chest and may cause the lower esophageal sphincter (LES) to herniate into the chest where its barrier function is impaired [Zerbib et al. 2002; Choy and Leung, 1997]. This could therefore allow more reflux of gastric contents among asthmatics with hyperinflation.
Some asthma medications aimed at reducing hyperinflation may promote acid reflux. Both beta-agonists and theophylline may decrease LES tone, which again potentially could foster acid reflux. One study of theophylline showed that symptoms of GERD increased by 170% in the theophylline group compared with placebo [Ekstrom and Tibbling, 1988]. Beta-agonists have been shown to cause reductions of LES tone in a dose-dependent fashion [Crowell et al. 2001]. This suggests the potential for a vicious cycle of GERD-induced asthma symptoms resulting in increased use of bronchodilators, which in turn promotes more GERD.
There are also some GERD-related pathogenic factors which could worsen asthma.
The parasympathetic nervous system, specifically the vagus nerve, highly innervates both the esophagus and the tracheobronchial tree and may be a common pathogenic pathway for GERD and asthma. In animal studies, instillation of acid into the esophagus was shown to increase respiratory resistance with effects ablated by bilateral vagotomy [Mansfield et al. 1981].
In humans, instillation of acid in the esophagus has been shown to decrease peak expiratory flow rates and increase overall airway resistance [Harding et al. 1995]. Both of these consequences are blunted by pretreatment with atropine. In contrast, others have found no relationship between the instillation of acid and methacholine reactivity or lung function [Araujo et al. 2008]. Some data seem to suggest that acid refluxed from the stomach into the esophagus may ‘prime’ the lung to have subsequent and more severe episodes of bronchospasm when exposed to another trigger. Vincent and colleagues showed that the dose of methacholine which caused the forced expiratory volume in one second (FEV1) to fall by 20% (PD20) was significantly correlated with the number of acid reflux events as documented by pH-probe analysis over a 24-hour period [Vincent et al. 1997]. The dose of methacholine required to provoke the patients with more significant reflux tended to be a lot lower, suggesting an increase in airway hyper-responsiveness.
Another question raised has been whether GERD-induced aspiration or microaspiration could worsen asthma, as tracheal microaspiration of acid has been found to be a very potent stimulus for bronchospasm [Jack et al. 1995]. In addition, microaspiration may trigger bronchospasm indirectly by inducing chronic inflammatory changes which subsequently can lead to increased airway reactivity. Animal models have shown that instillation of acid into the esophagus can trigger an inflammatory cascade. One study showed that esophageal acid led to significantly increased levels of Substance P, a tachykinin that leads to smooth muscle contraction and increased vascular permeability [Hamamoto et al. 1997]. Acid provocation has also been shown to lead to increased lung resistance in a dose-dependent fashion which is mediated by release of tachykinins from peripheral nerves [Ricciardolo et al. 2004]. Aspiration of acid may also cause injury directly to the epithelial lining of the upper airway which has been shown to result in a release of cytokines and increased inflammation [Stein, 1999].
All of these data afford biologic plausibility to the theory that asthma and medications used for treatment may increase GERD and GERD may subsequently induce asthma symptoms either by direct effects on airway hyperresponsiveness or via increases in airway inflammation. The question then becomes is there any outcome data demonstrating that these theories have clinical relevance?
Relationship between treatment of GERD and asthma outcomes
Initial studies focused on the effects of treatment of GERD on asthma outcomes revealed inconsistent results, but in general seemed to suggest an overall improvement in some asthma symptoms [Kiljander et al. 1999; Boeree et al. 1998; Levin et al. 1998; Teichtahl et al. 1996; Ford et al. 1994; Meier et al. 1994; Gustafsson et al. 1992; Larrain et al. 1991; Ekstrom et al. 1989; Nagel et al. 1988; Goodall et al. 1981; Kjellen et al. 1981]. These data resulted in recommendations by the National Asthma Education and Prevention Program’s Expert Panel Report 3 (EPR-3) that ‘gastroesophageal reflux treatment may benefit patients who have asthma and complain of frequent heartburn or pyrosis, particularly those who have frequent nighttime asthma symptoms. Even in the absence of suggestive GERD symptoms, consider evaluation for GERD in patients with poorly controlled asthma’ [Busse and Lemanske, 2007]. However, these initial studies all had significant limitations: the sample sizes of the populations were small; inconsistent definitions of asthma and GERD were utilized for inclusion; variable outcome measures were recorded; multiple GERD treatment regimens including histamine-2 receptor (H-2) antagonists and proton-pump inhibitors (PPIs) were used for relatively short durations (<3 months) in groups of patients with varying degrees of asthma severity.
These limitations were highlighted in a 2003 systematic review of the currently available literature by the Cochrane Collaboration examining the utility of GERD treatment for asthma [Gibson et al. 2000]. The analysis included 12 randomized controlled trials with a combined total of 432 subjects in whom the effects of GERD therapy on asthma outcomes were reported [Kiljander et al. 1999; Boeree et al. 1998; Levin et al. 1998; Teichtahl et al. 1996; Ford et al. 1994; Meier et al. 1994; Gustafsson et al. 1992; Larrain et al. 1991; Ekstrom et al. 1989; Nagel et al. 1988; Goodall et al. 1981; Kjellen et al. 1981]. Treatment with antireflux therapy did not consistently improve any one measure of pulmonary function in patients with asthma, but some studies did report objective improvement in single measurements of lung function such as FEV1 [Meier et al. 1994; Larrain et al. 1981], morning peak expiratory flow rates (PEF) [Levin et al. 1998] and evening PEF [Teichtahl et al. 1996; Goodall et al. 1981]. The variability in reporting of asthma symptoms in the included studies prevented detailed analysis of any parameter except for nocturnal asthma symptoms which were noted to be improved by some authors in patients treated with histamine antagonists [Ekstrom et al. 1989; Goodall et al. 1981] or omeprazole [Kiljander et al. 1999]. However, others failed to show improvement in nocturnal asthma symptoms with GERD therapy [Boeree et al. 1998; Ford et al. 1994; Gustafsson et al. 1992]. From these data, the Cochrane group concluded that ‘in asthmatic subjects with gastroesophageal reflux, there was no overall improvement in asthma following treatment for gastroesophageal reflux’, and the authors called upon researchers to develop larger randomized controlled trials using longer courses of treatment to better evaluate the role of antireflux therapy in these patients [Gibson et al. 2000].
Select randomized, placebo-controlled studies of proton-pump inhibitor therapy and asthma control.
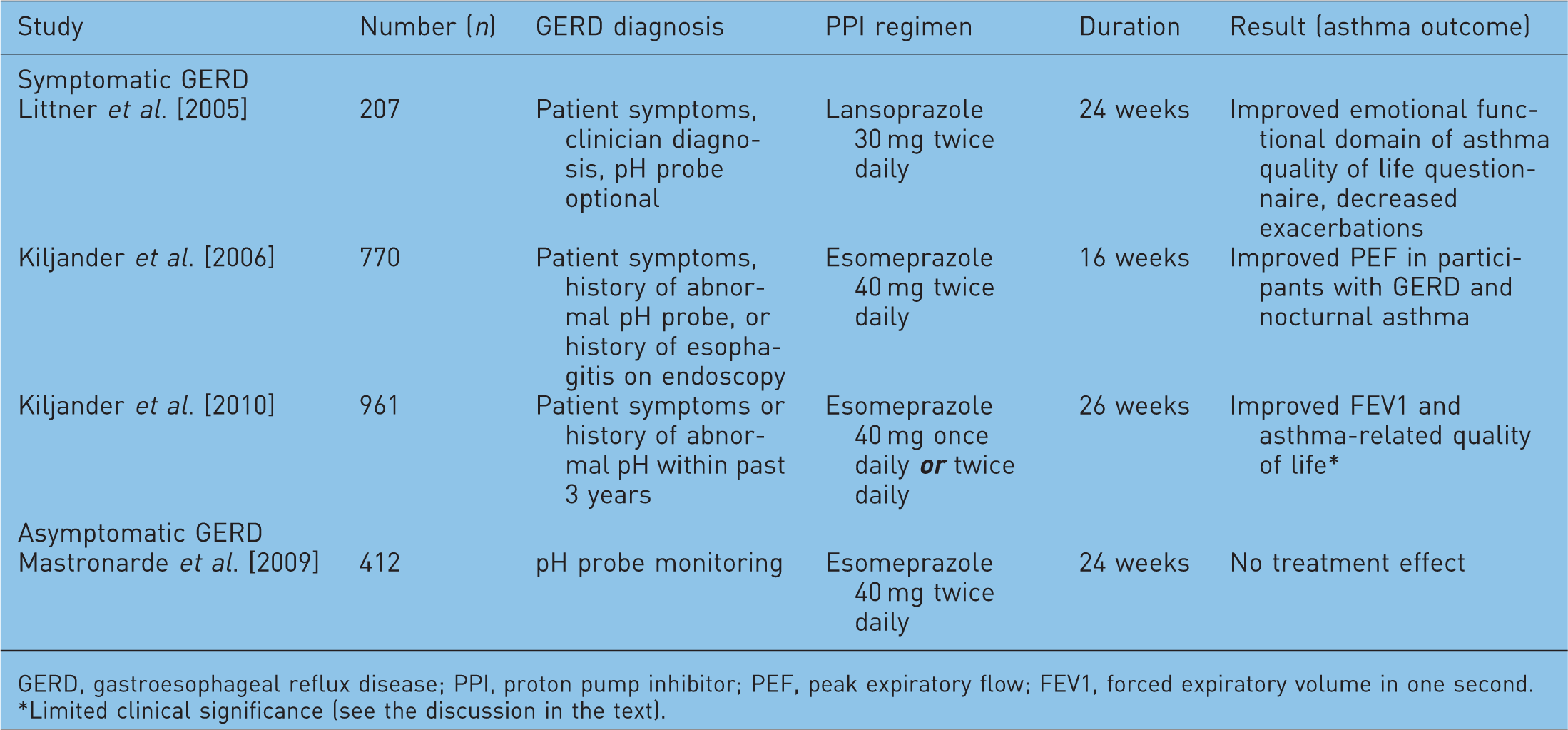
GERD, gastroesophageal reflux disease; PPI, proton pump inhibitor; PEF, peak expiratory flow; FEV1, forced expiratory volume in one second.
Limited clinical significance (see the discussion in the text).
Kiljander and associates assessed the effects of esomeprazole 40 mg twice daily versus placebo for 16 weeks among 770 patients with moderate-to-severe asthma [Kiljander et al. 2006]. The study included asthmatics with moderate-to-severe asthma based on FEV1 (50–80% predicted) and evidence of bronchodilator reversibility. The presence of GERD was based primarily on patient reported clinical symptoms. Participants were classified into one of three groups based on the presence or absence of GERD and nocturnal respiratory symptoms (NOC): GERD with NOC, GERD without NOC, and NOC without GERD. Overall, there were no improvements in daily peak expiratory flow rate, asthma symptoms, asthma related quality of life, or asthma exacerbations in those asthmatics treated with esomeprazole. In the subgroup of participants with GERD and NOC, statistically significant improvements in the morning and evening PEF were observed in subjects who received esomeprazole when compared with placebo, suggesting that this subgroup may benefit from PPI therapy. However, these changes in PEF were relatively small (8.7 l/min for morning and 10.2 l/min for evening) and may be of limited clinical significance. Of interest, though, the improvements in PEF were most significant in those asthmatics receiving long-acting beta-agonists. The study was limited by the short duration of therapy for GERD and the use of patient-reported symptoms of acid reflux as the primary basis of diagnosis.
In a follow-up study, Kiljander and colleagues compared the efficacy of 40 mg once daily esomeprazole with 40 mg twice daily esomeprazole in improving asthma control in patients with symptomatic GERD [Kiljander et al. 2010]. They included 961 patients with moderate-to-severe asthma with demonstrated reversibility of airflow obstruction and ≥1 clinically important asthma exacerbation within the preceding 12 months with symptomatic GERD (as determined by the Reflux Disease Questionnaire [Shaw et al. 2001]). After 26 weeks of therapy, there was no improvement noted in the primary endpoint of the study, change from baseline mean morning PEF, in either study group. In addition, no differences were noted in use of rescue bronchodilators, percentage of asthma symptom-free days, or frequency of severe asthma exacerbations. Treatment with esomeprazole at both doses was associated with a statistically significant improvement in FEV1 and asthma-related quality of life throughout the study period. However, the improvement in FEV1 was small and likely of small clinical significance, with an increase of 0.09 l (CI 0.03–0.15; p = 0.0039) or 0.12 l (CI 0.06–0.18; p < 0.0001) for esomeprazole 40 mg once or twice daily, respectively. Significantly more participants treated with esomeprazole reported a significant improvement in asthma-related quality of life than those treated with placebo (esomeprazole once daily, n = 173, 61%; p = 0.016; esomeprazole twice daily, n = 176, 62%; p = 0.001). However, the clinical significance of this finding remains uncertain.
Therefore, in some asthmatics with symptoms suggestive of GERD, the available literature suggests that there may be a small benefit of treatment of GERD on some aspects of asthma-related quality of life and possibly on exacerbations, but no clear evidence supports objective benefits in pulmonary function or overall asthma control. However, one could argue that treatment for symptomatic GERD is warranted in patients with asthma independent of any potential benefit on asthma outcomes if the underlying GERD warrants treatment on its own. The current NIH guidelines recommend an empiric trial of GERD therapy in poorly controlled asthmatics even if they do not have GERD symptoms [Busse and Lemanske, 2007]; however at the time of their publication, no studies had been completed specifically to address this unique clinical situation. Furthermore, these guidelines were based on studies which included participants with symptomatic GERD based primarily on patient-reported clinical symptoms rather than more objective measurements of acid reflux such as 24-hour pH probe monitoring. In these studies, no attempts to correlate episodes of reflux with asthma symptoms were made, nor were investigators clearly able to identify those subgroups of patients who benefited most from PPI therapy.
The American Lung Association Asthma Clinical Research Centers conducted a multicenter, randomized, placebo-controlled trial of esomeprazole 40 mg twice daily for 24 weeks in patients with poorly controlled asthma and minimal or no symptoms of (silent) gastroesophageal reflux, using ambulatory esophageal pH monitoring to confirm the presence or absence of gastroesophageal reflux in participants [Mastronarde et al. 2009]. Four hundred and twelve patients on moderate or high doses of inhaled corticosteroids with inadequately controlled asthma (defined as either a Juniper Asthma Control Questionnaire [JACQ] [Juniper et al. 2006] of 1.5 or higher or the presence of more than one unscheduled healthcare visit for asthma in the preceding 12 months) underwent pH testing and were randomly assigned to treatment with esomeprazole or placebo independent of pH study results. Investigators and participants were blinded to the results of the pH study and intervention. The diagnosis of asthma was based on physician diagnosis with either a positive methacholine challenge test or evidence of bronchodilator reversibility of the FEV1 with an increase of ≥12% after short-acting bronchodilator administration. The primary objective of the study was to determine whether acid suppression therapy could improve asthma symptoms as determined by frequency of episodes of poor asthma control which were defined as any one of the following: a decrease from a patient’s best morning PEF, an unplanned healthcare visit for asthma, the need for systemic corticosteroids for asthma treatment, or an increase in the use of short-acting beta-agonists of a least four inhalations above baseline. After 6 months of therapy, episodes of poor asthma control occurred with similar frequency in the placebo and esomeprazole groups (2.3 versus 2.5 events per person-year respectively; p = 0.66). Although nighttime awakenings due to asthma occurred on more than one occasion in over half of the subjects, there was no significant difference between groups. Similarly, there was no difference with respect to lung function (including PEF, FEV1, and methacholine responsiveness), asthma symptoms, or asthma related quality of life when patients treated with esomeprazole were compared with those who received placebo. Ambulatory pH monitoring demonstrated acidic gastroesophageal reflux in approximately 40% of both groups of participants, but failed to identify a subgroup of patients that was likely to benefit from therapy with the PPI. From these findings, Mastronarde and colleagues concluded that the empiric use of acid suppression in patients with poorly controlled asthma but minimal or no GERD symptoms should not be routinely recommended [Mastronarde et al. 2009].
To date, this is the only published trial evaluating the effects of treatment of silent GERD on asthma control. It is difficult to compare the results of this study with those examining the effects of treatment of symptomatic GERD in asthma because those trials relied on patient-reported symptoms. It is possible that those subjectively noted symptoms were not related to acid in the esophagus at all and, therefore, would not be expected to change with acid suppression therapy or be expected to alter the measured asthma-related outcomes. Until further studies are undertaken to objectively correlate GERD symptoms with GERD in patients with asthma, it remains impossible to clearly describe the potential differences between symptomatic and silent GERD on asthma outcomes.
The potential importance of the location of reflux in the esophagus (proximal versus distal) has also been considered as a potential important factor in the clinical relationship between asthma and GERD. In a small study (n = 133) of subjects with upper airway symptoms attributed to GERD, dual-probe esophageal pH monitoring demonstrated a significantly higher incidence of nocturnal cough in those participants with acid reflux detected at both the proximal and distal probe than in those in whom reflux was detected at the distal probe alone [Tomonaga et al. 2002]. While the possibility that the participants’ nocturnal cough may have been related to uncontrolled asthma was not specifically addressed by the authors, the study still raises the important issue that symptoms from proximal GERD such as cough may mimic asthma and may confound measurements of asthma control in the clinical and research setting. A subgroup (n = 242) of participants in the American Lung Association’s Study of Acid Reflux and Asthma [Mastronarde et al. 2009] underwent dual-probe pH esophageal monitoring [DiMango et al. 2009]. Thirty-eight percent of participants demonstrated proximal GERD, but concordance between proximal and distal GERD on pH probe was poor. While the presence of proximal GERD was associated with worse asthma-related quality of life, no differences were noted in other the asthma-related clinical outcomes measures described above. It has been hypothesized that nonacidic or alkali reflux may affect asthma control parameters [Asano and Suzuki, 2009], but, to date, this interesting theory remains untested.
Summary and conclusions
The relationship between GERD and asthma control remains unclear. The clinical prevalence of the two conditions in many patients cannot be ignored, and multiple theories highlighting plausible pathogenic explanations for these associations have been described. The treatment of symptomatic GERD in patients with asthma is important to control the underlying GERD and should be undertaken based upon current guidelines for treatment of the GERD. Currently available data have shown limited benefits of treatment of symptomatic GERD on asthma outcomes and no clear benefit on asthma control. However, in a significant percentage of asthmatics, GERD is clinically silent or associated with only mild symptoms. Empiric treatment of clinically silent GERD in patients with uncontrolled asthma does not seem to be an effective therapy for asthma and is not supported by current data. Instead, the clinician should focus on other factors which can affect asthma control such as use of adequate controller medications, patient compliance, proper inhaler technique, and control of other significant comorbid conditions.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest statement
None declared.