
Abstract
Pneumocystis is an opportunistic fungal pathogen that causes an often-lethal pneumonia in immunocompromised hosts. Although the organism was discovered in the early 1900s, the first cases of Pneumocystis pneumonia in humans were initially recognized in Central Europe after the Second World War in premature and malnourished infants. This unusual lung infection was known as plasma cellular interstitial pneumonitis of the newborn, and was characterized by severe respiratory distress and cyanosis with little or no fever and no pathognomic physical signs. At that time, only anecdotal cases were reported in adults and usually these patients had a baseline malignancy that led to a malnourished state. In the 1960–1970s additional cases were described in adults and children with hematological malignancies, but Pneumocystis pneumonia was still considered a rare disease. However, in the 1980s, with the onset of the HIV epidemic, Pneumocystis prevalence increased dramatically and became widely recognized as an opportunistic infection that caused potentially life-treating pneumonia in patients with impaired immunity. During this time period, prophylaxis against this organism was more generally instituted in high-risk patients. In the 1990s, with widespread use of prophylaxis and the initiation of highly active antiretroviral therapy (HAART) in the treatment of HIV-infected patients, the number of cases in this specific population decreased. However, Pneumocystis pneumonia still remains an important cause of severe pneumonia in patients with HIV infection and is still considered a principal AIDS-defining illness. Despite the decreased number of cases among HIV-infected patients over the past decade, Pneumocystis pneumonia continues to be a serious problem in immunodeficient patients with other immunosuppressive conditions. This is mostly due to increased use of immunosuppressive medications to treat patients with autoimmune diseases, following bone marrow and solid organ transplantation, and in patients with hematological and solid malignancies. Patients with hematologic disorders and solid organ and hematopoietic stem cell transplantation are currently the most vulnerable groups at risk for developing this infection. However, any patient with an impaired immunity, such as those receiving moderate doses of oral steroids for greater than 4 weeks or those receiving other immunosuppressive medications are at also at significant risk.
Introduction
Pneumocystis encompasses a genus of opportunistic fungal pathogens that cause potentially lethal pneumonia in immunocompromised hosts. Although the organism was discovered in the early 1900s, the first cases of Pneumocystis pneumonia in humans were initially recognized in Central Europe after the Second World War, in premature and malnourished infants. This unusual lung infection was known as plasma cellular interstitial pneumonitis of the newborn, and was characterized by severe respiratory distress and cyanosis with little or no fever and no pathognomic physical signs [Baar, 1955]. At that time, only anecdotal cases were reported in adults. Usually these patients had an underlying malignancy that led to a malnourished state. In the 1960–1970s, additional cases were described in adults and children with hematological malignancies, but Pneumocystis pneumonia was still considered a rare disease. However, in the 1980s, with the onset of the HIV epidemic, the prevalence of Pneumocystis increased dramatically and became widely recognized as an opportunistic infection that caused often-lethal pneumonia in patients with impaired immunity. During this time period, prophylaxis against this organism was more generally instituted in high-risk patients [Fischl et al. 1988]. In the 1990s, with widespread use of prophylaxis and the initiation of highly active antiretroviral therapy (HAART) in the treatment of HIV-infected patients, the number of cases in this specific population decreased. However, Pneumocystis pneumonia still remains an important cause of severe pneumonia in patients with HIV infection and is still considered a principal AIDS-defining illness [Kaplan et al. 2000; Jones et al. 1999].
Despite the decreased number of cases among HIV-infected patients over the past decade, Pneumocystis pneumonia continues to be a serious problem among other immunosuppressed patients. This is mostly due to the increased use of immunosuppressive medications to treat patients with hematological and solid malignancies, bone marrow and solid organ transplantation, and patients with autoimmune diseases [Dungarwalla et al. 2007; Harigai et al. 2007; Kalyoncu et al. 2007; Kaur and Mahl, 2007; Kolstad et al. 2007; Lahiff et al. 2007; Yale and Limper, 1996]. This article summarizes the current knowledge about the biology, pathogenesis, and diagnosis of Pneumocystis infection as well as prophylaxis and treatment recommendations, as used by our group and as supported by the existing guidelines.
Historical considerations and taxonomy
Current concepts propose that Pneumocystis species have likely co-evolved and co-existed with their respective mammalian hosts for thousands of years (as reviewed by Aliouat-Denis et al. [2008]). However, it was not until 1909 that Carlos Chagas first described members of this genus when working in a guinea-pig model of trypanosome infection. Chagas initially believed that he had found a new type of trypanosomal organism or life form. Antonio Carini came to the same conclusion 1 year later when he identified similar organisms in the lungs of his rat colony. It was not until 1912 that the Delanoës working at the Pasteur Institute in Paris recognized that Pneumocystis in rat represented a unique species and christened this organism Pneumocystis carinii in honor of Antonio Carini.
Despite the knowledge of its existence in animals, the first human cases were not described until 1942 by two Dutch investigators, Van der Meer and Brug [Van der Meer and Brug, 1942]. In 1952, Vanek and Jírovec reported that Pneumocystis “carinii”, later renamed Pneumocystis jiroveci, was the cause of interstitial pneumonia in neonates [Vanek and Jírovec, 1952]. The persisting belief of that era was that Pneumocystis was a protozoan and was classified as such for many years. This was likely due to the existence of two life forms that are morphologically parallel to other protozoan organisms, as well as its response to the antiprotozoan medication pentamidine. Despite this prevailing theory, Giese is first credited with proposing that Pneumocystis may be a yeast and that the foamy material described in the airway of these patients were spores [Giese, 1953]. However, it was not until 1988 when Edman and colleagues sequenced the small ribosomal RNA subunit that Pneumocystis species were correctly classified as ascomycetous fungi [Edman et al. 1988].
The genus Pneumocystis encompasses a variety of ubiquitous fungi that can colonize and infect almost every species of mammalian hosts. In addition, nucleic acids from Pneumocystis carinii, one of the species that infects rats, have been found in ambient air and pond water [Wakefield et al. 1998]. However, a true environmental reservoir of viable Pneumocystis organisms has not been established. Pneumocystis species are also quite different in their unique specificity for a particular mammalian host. For example, the human-specific species Pneumocystis jiroveci is only capable of infecting humans and is unable to infect other animals and vice versa. The host specificity of Pneumocystis across respective host species was further investigated by Dr Wakefield using a polymerase chain reaction (PCR) approach. She developed a set of primers from the mitochondrial large subunit rRNA of all known species of Pneumocystis and showed that when the nonhuman primers were used in human samples no amplification was detected and conversely human primers failed to amplify Pneumocystis from nonhuman samples (as reviewed by Stringer [2002]). Interestingly, human Pneumocystis jiroveci was found to be closest in homology to primate-derived Pneumocystis organisms. However, infection of a Pneumocystis species into its nonnative mammalian host has never been documented conclusively.
As a result of this absolute host species specificity, Pneumocystis organisms have been speciated, in part, according to the mammalian host that it infects. For instance, rats are infected with P. carinii and P. wakefieldiae, mice are infected by P. murina, and humans are susceptible to P. jiroveci, in honor of Dr Jírovec, who first associated this organism with human disease. For the purpose of this review we use the term Pneumocystis as the general genus name, unless otherwise specified.
Life cycle and pathogenesis
The study of the Pneumocystis life cycle has been challenging for many years due to both the fact that an environmental niche is still unknown, and that a long-term in vitro culture system has remained elusive. Transient proliferation has been achieved on lung epithelial and other feeder cells [Limper et al. 1997b; Cushion et al. 1985]. However, despite isolated reports of short-term in vitro culture in the absence of feeder cells [Merali et al. 1999], sustained cultures have not been consistently observed. Thus, the Pneumocystis scientific community remains without a reproducible and valid culture system to study this organism. Despite these challenges, considerable advances have been made over the years using molecular techniques. Immune-suppressed animal models of Pneumocystis pneumonia continue to serve as a reliable source of organisms for study. More recently, the analysis of the P. carinii genome project, begun in 1997 by Cushion and Arnold, has been of considerable benefit to the Pneumocystis research community. It is important to note that all of the currently available agents used to treat P. jiroveci pneumonia in humans, were initially derived from study of P. carinii and other species in rodents.
Ultrastructural studies of animal and human derived organisms have provide some insight into the life cycle of Pneumocystis and have established that there are at least two different life forms, the trophic form and the cyst. The trophic form generally measures about 2 µm, possesses a single nucleus, and is surrounded by a plasma membrane. In contrast, the cyst is significantly larger, approximately 8–10 µm in size, contains up to eight intracystic bodies and is surrounded by a characteristic thick cyst wall. Upon rupture of the wall, known as excystment, the intracystic bodies are released to become new trophic forms of the organism. The Pneumocystis cyst wall is formed largely of β-glucans, a complex branching polysaccharide, but other components such as mannoproteins, chitins, and other proteins are also present. The main function of this wall is to confer rigidity and support for the organism, and putatively, to protect the organism from harsh environmental conditions outside the host. The maintenance of the cyst wall is a dynamic process of formation and degradation. While the cyst wall is essential to provide rigidity and viability of the organism, degradation of this wall is also necessary during excystment for the organism to complete its life cycle. To facilitate this dynamic process, β-glucan synthetases facilitate formation of the β-1,3-glucan homopolymers that comprise the cysts wall, and β-glucanases and other proteins drive the active process of degradation and restructuring of the wall. Our group first described the Pneumocystis PcGsc1 gene responsible for glucan synthesis, and recently characterized the PcEng2 β-1,3-endoglucanase that participates in cell wall remodeling [Villegas et al. 2009; Kottom and Limper, 2000]. Such enzymes responsible for cell wall integrity are essential to the Pneumocystis life cycle, and may represent attractive targets for future therapeutic strategies. This is noteworthy, since emerging resistance to current therapeutic agents has been described recently (see the treatment section for further details).
Other important activities of Pneumocystis cell wall β-glucans have recently been described by a number of investigators. Multiple lines of evidence indicate that Pneumocystis β-glucans have the capacity to induce multiple inflammatory pathways in the host. Thus, it has been proposed that cell wall β-glucans contribute to the exaggerated inflammatory responses elicited by alveolar macrophages and respiratory epithelial cells, promoting respiratory failure in patients with severe Pneumocystis pneumonia [Carmona et al. 2006; Lebron et al. 2003; Vassallo et al. 1999a, 1999b; Limper et al. 1989]. In addition, Pneumocystis β-glucans have also been shown to activate dendritic cells and modulate T-cell responses [Carmona et al. 2006], crucial for Pneumocystis clearance. Moreover, β-glucans have been demonstrated to prime dendritic cells in a manner that they polarized T cells toward Th17 differentiation, which further promotes host antifungal immune resistance [Zelante et al. 2007]. Several excellent reviews of host defense and immunity during Pneumocystis pneumonia have been published recently [Goodridge et al. 2009; Thomas and Limper, 2007; Gigliotti and Wright, 2005].
Unlike most other fungi, the route of Pneumocystis infection is not completely understood. The most commonly accepted theory is that infectious organisms are transmitted as aerosolized particles from host to host. However, the exact mechanisms of infection continue to be debated. Some investigators propose a model of initial infection in infancy or early childhood, with reactivation later in life during periods of immune suppression. In contrast, other investigators propose that while initial infection is nearly universal in early childhood, the infection is actually re-acquired again, later in life, if the host lacks T-cell-based immune responses necessary for effective defense. Observations that support the first theory are from the fact that it is not unusual to detect the presence of Pneumocystis in otherwise healthy animals [Demanche et al. 2005] implying that otherwise normal healthy hosts may serve as a reservoir for infection. Additional data in both animal models, and humans, indicate that exposure and colonization can occur very early in life, and may further support that reactivation later in life is possible [Icenhour et al. 2002].
In humans, serologic evidence of anti-Pneumocystis antibodies or positive PCR in healthy children supports early exposure to this organism. Additional data indicate that adults with chronic obstructive pulmonary disease (COPD) may be colonized with subsequent reactivation during periods of immune suppression. In addition, a recent study by Vargas and colleagues demonstrated that over 60% of individuals who underwent a legal autopsy in Santiago, Chile, were colonized with Pneumocystis. The cause of death in these cases was unrelated to active Pneumocystis infection, and was either a violent cause or other indications that required legal autopsy. Unfortunately, prior medical histories of the autopsied cases were not available [Ponce et al. 2010]. Nonetheless, these data further support the notion of colonization of otherwise healthy individuals. In contrast, however, other studies have failed to detect Pneumocystis organisms in postmortem evaluation of immunocompetent adults [Peters et al. 1992b; Peglow et al. 1990; Wakefield et al. 1990a, 1990b; Pifer et al. 1978]. This contradictory data may be explained by a state of transient colonization of otherwise healthy individuals or by different sensitivities of the methodologies used in these studies. However, the fact that some individual are at least transiently colonized supports the concept of possible reservoirs of Pneumocystis within immune-competent humans. Whether Pneumocystis pneumonia itself is due to reactivation of latent colonization or newly acquired infection or a combination of the two ultimately remains a matter of debate at the present time.
Once inhaled, Pneumocystis has considerable tropism for the lung and rarely disseminates to other organs, although occasional cases of extrapulmonary dissemination have been reported, specifically in patients with advanced HIV infection [Panos et al. 2007; Hagmann et al. 2001; Bartlett and Hulette, 1997; Ruggli et al. 1997; Guttler et al. 1993; Dieterich et al. 1992]. When the infective form is inhaled it reaches the alveoli. Trophic forms bind tightly to alveolar epithelial cells and extracellular matrix proteins [Walzer, 1986]. Several studies have shown that interactions with the extracellular matrix proteins and in particular with fibronectin facilitate binding of Pneumocystis to lung epithelial cells [Limper et al. 1993]. More recently, our laboratory has identified a novel integrin-like extracellular matrix adhesion receptor, PcInt1, expressed only on the trophic form, which mediates attachment of the organism to fibronectin [Kottom et al. 2008]. Adhesion of Pneumocystis to the epithelium triggers several signaling pathways, which mediate mating, morphological changes and proliferation. It is hypothesized that a sexual conjugation-mating phase takes place followed by meiosis and mitosis resulting in generation of the mature cyst [Burgess et al. 2008]. Attachment to the alveolar epithelium also has several consequences for host such as suppression of the lung epithelial cell growth and repair and initiation of multiple inflammatory pathways.
Risk factors
It is important to emphasize that while the underlying condition that may have lead to the infection has clinical and prognostic implications to the host, the degree of the impaired innate and acquire cellular immunity are critical predicting factors for lung function and survival during Pneumocystis pneumonia. For instance, CD4 lymphocytes are essential for the clearance of the organisms and patients with a CD4 count of less than 200 cells per cubic meter have been shown to be at higher risk for infection [Phair et al. 1990; Shellito et al. 1990]. The Pneumocystis-infected SCID mice model have provided evidence that Pneumocystis clearance is impaired due to a lack of CD4 and CD8 cells [Wright et al. 1999]. Interestingly, these animals do not present gas exchange abnormalities until the very late phase of the infection suggesting that T cells may also play a role in oxygenation. Immune reconstitution of these mice with normal spleen cells results in significant deterioration of their lung function as a result of an intense CD8 T-cell-mediated inflammatory response [Wright et al. 1999; Beck et al. 1991]. Similar findings have been observed in HIV-infected patients during immune reconstitution while on HARRT treatment or bone marrow transplant patients during engraftment [Wislez et al. 2001]. Other findings such as prolonged neutropenia, impaired macrophage activity, inhibition or neutralization of tumor necrosis factor (TNF)-α responses and other factors are also considered important [Lasbury et al. 2006; Thomas and Limper, 2004; Fishman, 2001; Koziel et al. 1998; Kolls et al. 1997; Limper et al. 1997a; Hoffman et al. 1993; Chen et al. 1992]. These studies indicate that a balance immune response is necessary to successfully defend against Pneumocystis infection.
As mentioned earlier in this review, the classical groups affected by Pneumocystis pneumonia have been patients with HIV infection and hematological malignancies. However, the incidence of Pneumocystis pneumonia is increasing in other groups such as posttransplant patients (including bone marrow transplant) and those with autoimmune and other inflammatory conditions; especially if they are receiving prolonged corticosteroid therapy as demonstrated in a retrospective case series from the Mayo Clinic. In that study, 116 consecutive non-HIV patients with a new diagnosis of Pneumocystis pneumonia were investigated. Interestingly, more than half of the patients (57%) in the study did not have an underlying malignant process. Some of these individuals were transplantation patients (25%), but the majority had an inflammatory or autoimmune condition. Most of the patients received systemic corticosteroids within a month of diagnosis with an equivalent dose of prednisone that averaged 30 mg/day. However, for 25% of the individuals, the averaged prednisone dose was as little as 16 mg a day. The mean duration of corticosteroid therapy was 12 weeks, but one quarter of the patients developed Pneumocystis pneumonia after 8 weeks or less [Yale and Limper, 1996]. Overall, these data suggested that not only patients on high-dose steroids are at risk, but, in fact, doses of prednisone between 16 and 20 mg/day for at least 4–6 weeks are great enough to increase the risk of Pneumocystis pneumonia in these patients. Interestingly, the study also indicated that up to 10% of the patients affected with Pneumocystis pneumonia were not on systemic steroids. Unfortunately, no concomitant or past use of other immunosuppressant agents was reported in the study [Yale and Limper, 1996]. Although, it is possible that these patients had significant immune impairment due to their baseline condition, it is likely that they were receiving other immunosuppressant agents or even had prolonged impaired immunity from past immunosuppressive therapy.
Immunosuppressive agents associated with the development of Pneumocystis pneumonia.

Monoclonal antibodies
TNF, tumor necrosis factor.
Main indicators for Pneumocystis prophylaxis.

Prednisone (or dose equivalent) of at least 16–20 mg for >4 weeks.
COPD, chronic obstructive pulmonary disease; TNF, tumor necrosis factor; MTX, methotrexate, AZA, azathioprine; RT, radiotherapy; Tx, transplant.
Clinical manifestations and radiological findings
Clinical presentation of patients affected with Pneumocystis pneumonia differs among HIV and non-HIV immunosuppressed patients. For instance, HIV patients tend to present with subacute onset of progressive dyspnea, nonproductive or minimally productive cough, low-grade fever and malaise. However, up to 7% of these patients can be asymptomatic. In contrast, patients that are immunocompromised but HIV-negative usually present more acutely, with substantial dyspnea, fever, chills and some may initially present in urgent need of mechanical ventilation. Respiratory failure in this group carries an overall mortality of up to 40% [Festic et al. 2005]. Interestingly, HIV patients usually have significantly more organisms in the bronchoalveolar lavage (BAL) than non-HIV patients, but this does not seem to correlate with worse oxygenation. Indeed, the opposite has been demonstrated, in that patients with HIV-associated Pneumocystis pneumonia tend to have higher arterial oxygen tension and a lower alveolar-arterial oxygen gradient than non-HIV patients [Limper et al. 1989]. In contrast, neutrophil and inflammatory cell numbers, rather than organism burden, appear to correlate with the degree of oxygenation during Pneumocystis pneumonia, suggesting that patients that mount a more robust inflammatory response are at higher risk of developing respiratory failure compared with those who exhibit lower levels of lung inflammation [Limper et al. 1989].
The lung exam can also vary depending of the degree of illness, ranging from an essentially normal examination to diffuse crackles on auscultation. Extrapulmonary manifestations are not common. However, retinitis, thyroiditis, bone lesions and pneumocystosis of brain, liver, spleen and kidney have all been described rarely [Panos et al. 2007; Hagmann et al. 2001; Bartlett and Hulette, 1997; Guttler et al. 1993; Dieterich et al. 1992; Edelstein and McCabe, 1990]. These findings tend to occur more frequently in patients who have been on prophylaxis with aerosolized pentamidine or who were extremely immunocompromised, generally from advanced AIDS.
Radiological findings of Pneumocystis pneumonia are generally not specific and may range from a normal or near normal chest X-ray to different degrees of bilateral and usually symmetrical pulmonary infiltrates (Figure 1A). However, other less-common patterns have been reported, including: lobar infiltrates, pulmonary nodules, pneumatoceles and other cystic changes, and pneumothorax. These are more frequently found again in very severely immunocompromised individuals and those treated with aerosolized pentamidine [Edelstein and McCabe, 1990]. At times clinical symptomatology, specifically in the absence of significant chest X-ray findings, initiates more sensitive radiological approaches such as high-resolution chest CT. The most typical findings on chest CT are bilateral ground-glass opacities (Figure 1B). Less-common features can include reticular, granular, and cystic lesions (Figure 1C) [Hidalgo et al. 2003; Crans and Boiselle, 1999].
(A) Posteroanterior chest radiograph showing diffuse bilateral predominantly interstitial opacities in a 71-year-old male with Pneumocystis pneumonia in the setting of diffuse large B-cell lymphoma on R-CHOP therapy. (B) Selected noncontrast CT axial image revealing bilateral diffuse ground-glass opacities and associated interlobular and intralobular septal thickening. (C) Selected contrast CT axial image revealing diffuse ground-glass pulmonary infiltrates and innumerable cystic changes predominantly in the upper lobes in a 53-year-old male with Pneumocystis pneumonia in the setting of recently diagnosed HIV.
Other radiological techniques such as 18-fluorodeoxyglucose positron emission tomography (FDG-PET) and Ga-67 scintigraphy have been reported as potential tools to assist in the early diagnosis of Pneumocystis pneumonia [Zhuang and Alavi, 2002; Tumeh et al. 1992]. However, these techniques have been most commonly applied for the evaluation of other concomitant problem, with incidental or unexpected uptake in the lung prompting further diagnostic approaches, such as BAL to document Pneumocystis pneumonia. In the past, Ga-67 scintigraphy was proposed as an adjunct for early detection of Pneumocystis. However, with the implementation of more sensitive molecular techniques, the use Ga-67 scintigraphy no longer appears to be justified (see the diagnosis section).
Diagnosis
The single most important diagnostic tool for Pneumocystis infection is a high clinical suspicion. In the right clinical setting, an immunosuppressed patient with new onset of dyspnea or new symptoms of pneumonia, with or without radiological findings, should prompt further evaluation, particularly if they are not receiving chemoprophylaxis. Since Pneumocystis cannot be cultured, the gold standard for diagnosis is microscopic visualization of the organism. Traditionally different stains have been used to identify either the trophic form (Gram–Weigert, Wright–Giemsa or modified Papanicolaou stains) or the cyst forms (calcofluor white, cresyl echt violet, Gomori methenamine silver or toluidine blue) (Figure 2). However, the most common technique used currently in the majority of the laboratories is fluorescein-conjugated monoclonal antibodies. Sensitivity of these assays depends on several factors such as the type and quality of the sample (BAL versus sputum versus tissue), the number of organisms present, and the experience of the laboratory staff with the particular assay. In addition, all of these tests have their own advantages and disadvantages. For instance, calcofluor white has the advantages of being quick, convenient, and can identify the presence of other concomitant fungus. However, the main disadvantage of calcofluor is that this stain requires reviewer expertise for correct interpretation. On the other hand, the immunofluorescent antibody technique is advantageous in that it can detect both life forms of Pneumocystis and is also slightly more sensitive. However, immune fluorescence is more time consuming, and nonspecific staining can also occur [Procop et al. 2004]. Therefore, for those laboratories that use immunofluorescence as first-line test, confirmation with a second method is generally recommended [Procop et al. 2004]. Direct hematoxylin and eosin tissue examination frequently reveals frothy intra-alveolar exudates containing organisms, which can be further confirmed with either methenamine silver stain or immune staining (Figure 3).
Calcofluor white staining of Pneumocystis organisms in a bronchoalveolar lavage (BAL) specimen. A human cell on the right has picked up some of the fluorescent stain. Original size × 1000, scale bar is 20 µm. Histological features of Pneumocystis pneumonia. (A) Pneumocystis pneumonia in a surgical lung biopsy specimen. The characteristic frothy exudates harboring the organisms fills an alveolus (small arrows) lined by reactive type II cells (large arrow). Internal structures of the organisms can be discerned at high magnification (inset). Hematoxylin–Eosin stain; original ×400 and ×1000 (inset), scale bar is 25 µm. (B) Silver stain of Pneumocystis organisms in a surgical lung biopsy. The organisms appear round or cup-shaped, some show intracystic bodies (lower right). Gomori’s Methenamine Silver stain; original size ×400, scale bar is 25 µm. (C) Immunohistochemical stain for Pneumocystis organisms. Surgical lung biopsy; original size ×1000, scale bar is 25 µm. All three images provided courtesy of Dr Frank Schneider, Department of Pathology, Mayo Clinic, Rochester, MN.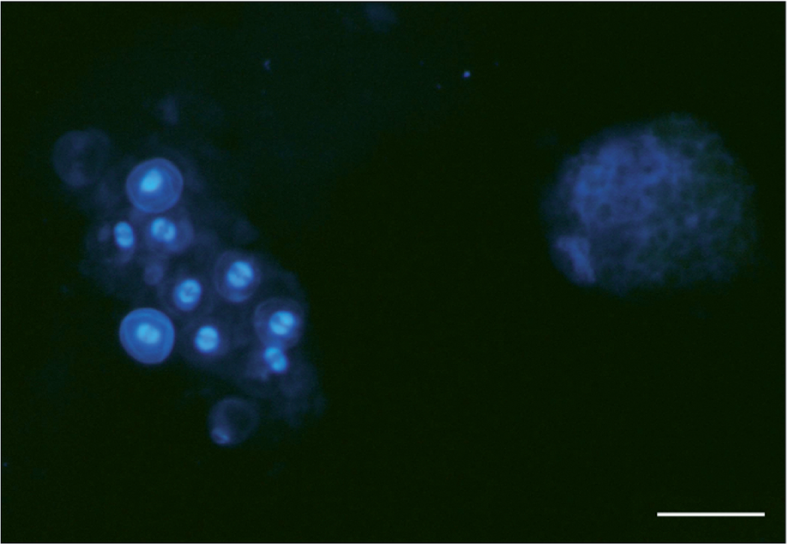

All of the direct organism visualization methods can lead to false-negative results, particularly in non-HIV patients. This has been attributed to fewer organisms being present in the collected samples [Limper et al. 1989]. Molecular methods are now available which have increased sensitivity and specificity and are particularly useful in these patient populations. In recent years, real-time PCR-based strategies have largely replaced earlier methods of nested PCR for clinical diagnosis, which may be less specific for active infection leading to higher false-positive rates [Helweg-Larsen et al. 1998; Ribes et al. 1997; Tamburrini et al. 1996; Lu et al. 1995; Cartwright et al. 1994; Peters et al. 1992a]. The use of real-time PCR has also reduced interrun contamination increasing the specificity of the assay. Multiple protocols that use various Pneumocystis gene targets have been developed. The main targeted genes include the heat shock protein gene (HSP70) [Huggett et al. 2008], the dihydrofolate reductase gene (DHFR) [Bandt and Monecke, 2007], the dihydropteroate synthase gene (DHPS) [Alvarez-Martinez et al. 2006], and the cell division cycle 2 gene (CDC2) [Arcenas et al. 2006]. In our institution, we utilize the PcCdc2, a single-copy gene target, and have applied the assay on sputum, BAL or tissue samples. On BAL samples the PcCdc2-based real-time PCR assay is 21% more sensitive than calcofluor white staining and has a specificity of 96%, with an analytical sensitivity of 5.6 copies per microliter of positive plasmid control. No cross-reactivity with other pathogens or human DNA was demonstrated using the PcCdc2 target [Arcenas et al. 2006]. False negatives are still possible with PCR-based approaches if fewer copies are present than the lower limit of detection for a given assay.
Despite increased sensitivity and specificity these assays continue to have difficulty discriminating between colonization and infection. Therefore, clinical correlation is always necessary. New techniques that detect messenger RNA (mRNA) have been proposed as surrogate markers for organism viability. The rationale is that mRNA is less stable than DNA. Therefore, if the patient is not actively infected with viable organisms, the mRNA should be largely degraded and no longer detected. In contrast, DNA is far more stable and may still be present even if the organisms are dead. Recent data from HIV patients with suspected Pneumocystis pneumonia using reverse-transcriptase PCR targeting a heat shock protein of Pneumocystis mRNA (Phsb1) have yielded a diagnostic sensitivity and specificity of 100% and 86%, respectively, in BAL specimens [de Oliveira et al. 2007].
The aforementioned methodologies can be applied to either BAL, sputum or to tissue. However, there are other indirect markers that can be potential be detected in serum, and serve as an adjunct for diagnosis. One of these assays is based on the detection of 1→3-β-D-Glucan (BDG) in serum. As mentioned earlier, β-glucans are structural components of the cell walls of most fungi and although this assay is not specific for Pneumocystis, substantially increased BDG levels have been found in patients with Pneumocystis infection [Fujii et al. 2007; Marty et al. 2007; Tasaka et al. 2007; Yasuoka et al. 1996]. In a retrospective case–control study of 295 patients with suspected Pneumocystis pneumonia, BDG was compared with microscopic examination of BAL. With an estimated cut-off level of 31.1 pg/ml of BDG, the sensitivity and specificity of the assay were 92.3% and 86.1%, respectively [Tasaka et al. 2007]. A more recent study of 35 consecutive retrospective cases diagnosed with Pneumocystis pneumonia also indicated that BDG levels might be a reliable diagnostic marker. However, the detection rate of BDG in non-HIV patients was lower than in HIV patients [Nakamura et al. 2009]. This could be attributed to the fact that HIV patients have greater numbers of organisms than non-HIV patients. These preliminary studies suggest that in the right clinical setting serum BGD may provide a useful noninvasive diagnostic adjunct for patients with Pneumocystis infection. However, additional studies are needed to address the general specificity of BGD in diagnosing Pneumocystis pneumonia versus other fungal infections in diverse immune-suppressed patient populations.
Another proposed serological marker for Pneumocystis pneumonia is KL-6, a mucin-like glycoprotein expressed on type II pneumocytes and bronchiolar epithelial cells. Several studies have found elevated levels in patients with Pneumocystis pneumonia. However, the reported false-positive rate and level of detection were not as good as for the DBG assay [Nakamura et al. 2009; Tasaka et al. 2007]. Recent investigations indicate that KL-6 is more a generalized marker for alveolar epithelial injury [Sato et al. 2004] and can also be found detected in nonfungal infections such as Legionella, severe tuberculosis, and respiratory syncytial virus bronchiolitis, and even in noninfectious interstitial lung diseases [Kawasaki et al. 2009; Sukoh et al. 2001; Inoue et al. 1995]; Therefore, KL-6 elevation in Pneumocystis is thought to be related to lung damage and regeneration of epithelium lining and cannot be used as a specific marker of Pneumocystis infection.
Treatment
Historically, the mainstay of treatment for Pneumocystis pneumonia has been trimethoprim-sulfamethoxazole (TMP-SMX). Despite the existence of other drugs to treat Pneumocystis pneumonia, TMP-SMX is still the recommended first-line therapy for patients with mild, moderate, and severe disease [Huang et al. 2006; Benson et al. 2004]. The standard dose for both the pediatric (older than 2 months of age) and adult population is 15–20 mg/kg/day of TMP and 75–100 mg/kg/day of SMX administered in divided doses. For severe cases, the intravenous (IV) form is preferred over the oral formulation. However, IV can be switched to oral once clinical improvement is achieved. Dose adjustments are necessary for patients with renal and liver failure since SMX is extensively metabolized in the liver and renally excreted. We recommend that SMX drug levels should be monitored for all patients receiving IV therapy although the literature is controversial and there are no current guidelines about when or how often the levels should be monitored [Klinker et al. 1998; Joos et al. 1995]. In our experience, levels should be obtained at least once to assure adequate dosage and avoid potential toxicities especially in patients with renal and liver failure. Further monitoring should be individualized according to patient comorbidities and clinical response.
At times, usually due to sulfonamide allergies or other adverse effects, the use of TMP-SMX may not be possible. In past decades, aerosolized pentamidine was an alternative option. However, aerosolized pentamidine has been associated with the development of disseminated disease, likely due to poor systemic levels. Thus, aerosolized pentamidine is now not generally recommended for treatment unless no other drugs are available or the patient has a very mild disease. The IV formulation of pentamidine has better coverage and greater efficacy than the aerosolized route. However, it is at times poorly tolerated due to side effects that include hypotension, hypoglycemia and pancreatitis. A number of alternative regimens have been developed with good success [Colby et al. 1999; Wilkin and Feinberg, 1999; Castro, 1998; Masur, 1992; Hughes, 1991]. For instance, regimens with the combination of primaquine with clindamycin have been shown to be valid and better tolerated than the classical alternative treatment with IV pentamidine [Smego et al. 2001; Toma et al. 1998]. Atovaquone is an orally available agent that can be used as an alternative therapy in mild to moderately severe cases [Madden et al. 2007; Colby et al. 1999]. The main limitation for atovaquone is that an IV formulation is not available restricting its use in severe cases. In addition, the absorption of oral atovaquone can be poor unless taken with fatty meals, which may be challenging for some patients. Recommended regimens are summarized in Table 2.
The current recommendation for the duration of treatment with any of these drugs is approximately 21 days. For those cases in which the disease progresses after 1–2 weeks of apparently adequate therapy, drug resistance should be suspected. Several studies have revealed mutations in the DPHS gene, the target for TMP and pyrimethamine, as well as the genes products that are targeted by SMX and dapsone [Crothers et al. 2005; Huang et al. 2004; Nahimana et al. 2004]. Mutations in the cytochrome B gene that confer resistance to atovaquone have also been reported [Kessl et al. 2004]. Isolated cases of treatment and prophylaxis failure have been associated with such mutations [Hauser et al. 2001; Helweg-Larsen et al. 1999]. However, these associations have not been consistently reported in all cases, and whether or not the detection of molecular resistance results in significant clinical resistance and treatment failure has still not yet been firmly established [Navin et al. 2001].
Controversy exists as to whether Pneumocystis pneumonia responds to echinocandins such as caspofungin. The mechanism of action echinocandins is through the inhibition of a β-1,3-glucan synthase targeting the integrity of fungal cell wall. Several studies in animals have shown that caspofungin has potential activity against P. carinii [Kottom and Limper, 2000; Powles et al. 1998]. More recently, several cases suggesting successful treatment in patients with Pneumocystis pneumonia have been reported as monotherapy or in combination with TMP-SMX [Mu et al. 2009; Hof and Schnulle, 2008; Utili et al. 2007; Annaloro et al. 2006; Beltz et al. 2006]. However, no rigorous preclinical animal data and no human randomized controlled trial clinical data are currently available. Thus, no recommendation on the use of these agents to treat human Pneumocystis pneumonia can be made at this time.
Another important aspect of Pneumocystis treatment is the use of corticosteroids, including prednisone, as adjunctive therapy. This regimen has been shown to be specifically beneficial in HIV patients who are hypoxemic, defined as a partial pressure of arterial oxygen below 70 mmHg or an alveolar-arteriolar oxygen gradient greater than 35 [The National Institutes of Health-University of California Expert Panel for Corticosteroids as Adjunctive Therapy for Pneumocystis Pneumonia, 1990]. A randomized controlled trial of 333 HIV patients with Pneumocystis pneumonia demonstrated that the use of corticosteroids reduced the risk of respiratory failure and death in patients with moderate to severe pneumonia. Despite an increase of localized herpetic lesions in the corticosteroid treatment group, no other infectious complications were detected [Bozzette et al. 1991]. In addition, a systematic review of adjunctive corticosteroid therapy in HIV-infected patients with Pneumocystis pneumonia and hypoxemia that included literature from the early 1980s through 2004 demonstrated a relative risk reduction for overall mortality at 1 month of 44%. It was also shown that the number needed to treat to prevent one death was lower in the period where HAART was not available compared with patients in later time periods that had access to HAART. They concluded that corticosteroid treatment in HIV-patients with moderate to severe Pneumocystis pneumonia was beneficial [Briel et al. 2006].
Treatment options for Pneumocystis pneumonia.

TMP-SMX, trimethoprim-sulfamethoxazole; IV, intravenous; IM, intramuscular.
Recommended duration of treatment is 21 days.
Emerging anti-inflammatory medications for Pneumocystis pneumonia are currently under investigation, especially for those severe cases with rapid progression to respiratory failure. Recent studies in a mouse model of Pneumocystis pneumonia have shown that depletion of T cells using and anti-CD3 antibody improves pulmonary function and survival rate compared with mice receiving the control antibody. This antibody, known as Muromonab-CD3 is currently in clinical use to treat transplant patients with organ rejection [Opelz, 1995]. Other agents such as the glycosphingolipid synthesis inhibitor, PDMP, also have activity as possible anti-inflammatory agents [Hahn et al. 2003]. However, further investigations are needed for these potential new adjunctive anti-inflammatory treatments for severe cases of Pneumocystis pneumonia.
Prophylaxis
Immunosuppressed patients especially those receiving corticosteroids or other immunosuppressive therapy should be considered candidates for Pneumocystis prophylaxis as outlined in the 2006 official American Thoracic Society Workshop on Pneumocystis [Huang et al. 2006]. Other guidelines about the specific use of prophylaxis in cancer and HIV-infected patients were published in 2008 and 2002, respectively [Segal et al. 2008; Kaplan et al. 2002]. A concise synopsis of the main recommendations for prophylaxis is given in Table 2 [Moosig et al. 2009; Mukhtyar et al. 2009; Lapraik et al. 2007; Godeau et al. 1995; Ognibene et al. 1995].
The preferred agent for prophylaxis for those who can tolerate sulfonamides continues to be TMP-SMX [Segal et al. 2008; Huang et al. 2006; Kaplan et al. 2002]. A meta-analysis of 12 randomized controlled trials of patients without HIV demonstrated that TMP-SMX dramatically reduced the number of Pneumocystis cases, up to 91%. The number needed to treat to prevent one infection was estimated at 15. However, no differences were detected in terms of all cause mortality. This differs from HIV patients in which a mean survival of 23 months versus 12 months was seen in patient treated with TMP-SMX compared with untreated patients [Fischl et al. 1988]. This may, in part, be related to effects of TMP-SMX in preventing other infections in this population such as toxoplasmosis [Mermin et al. 2005; Ioannidis et al. 1996; Hirschtick et al. 1995]. A comparison of the efficacy of daily with thrice-weekly regimens does not seem to show statistical differences [Green et al. 2007]. In HIV patients, the most commonly used regimen is a single strength dose daily (SMX 400 mg/TMP 80 mg), but for those patients who are toxoplasma serology positive, a double strength dose daily (SMX 800 mg/TMP 160 mg) offers them added protection against toxoplasma as well [Kaplan et al. 2002].
Prophylaxis options for Pneumocystis pneumonia.

DS tablet contains SMX 800 mg/TMP 160 mg.
SS tablet contains SMX 400 mg/TMP 80 mg.
TMP-SMX, trimethoprim-sulfamethoxazole; D, dapsone; P, pyrimethamine; L, leucovorin, SS, single strength, DS double strength; IV, intravenous.
The duration of prophylaxis varies depending on the underlying risk factors and must be individualized. In the particular case of immune reconstitution after antiretroviral therapy in HIV patients, the recommendation supports discontinuation of therapy when CD4 counts are >200 cells/µl for at least 3 months [Kaplan et al. 2002]. For non-HIV patients, prophylaxis can often be discontinued after the related risk factors, such as significant dose systemic corticosteroid or other immune suppressant agents are no longer exerting their effect. However, it should be kept in mind that the immunosuppressed state can persist for months after discontinuation of some cytotoxic agents such as cyclophosphamide. For non-HIV patients, the data to monitor peripheral CD4 counts does not correlate as convincingly with the risk of developing Pneumocystis pneumonia, as it does during HIV infection. However, many experts do suggest monitoring CD4 counts and discontinuing prophylaxis if the peripheral blood CD4 cells are greater than 200 cells/µl for at least 6 months [Suryaprasad and Stone, 2008].
Conclusions
Pneumocystis pneumonia remains a common problem and a high index of suspicion is necessary for those caring for individuals who are immunocompromised. Pneumocystis pneumonia is a preventable disease if chemoprophylaxis is instituted appropriately and patient remains compliant. It is very important to be aware of the clinical presentation and radiological appearance, since, in the particular case on HIV-infected patients, Pneumocystis can be the first presenting symptom of immune suppression even before the patient is aware of his or her HIV status [Walzer et al. 2008]. If Pneumocystis is suspected, the most widely employed clinical diagnostic approach is tinctorial or antibody staining of sputum or BAL. However, PCR-based assays are becoming increasingly popular and are now available in many institutions. Diagnostic results are rapidly available. If the index of suspicion is high and the initial sputum analysis is negative, BAL is recommended. TMP-SMX is still the preferred drug for treatment and prophylaxis, but other options are available for those individuals that are intolerant. For patients that do not respond to adequate treatment over the first 1–2 weeks of therapy, development of resistance should be suspected. The Pneumocystis research community continues to investigate this fascinating organism. New drugs are under development that may help treat patients with the severe lung disease.
Footnotes
Funding
This work was funded in part by NIH grants to AH Limper, R01HL62150 and R01HL55934.
Conflict of interest statement
AH Limper holds a US patent on a Pneumocystis diagnostic method using real time PCR recognizing the PcCdc2 target gene.