
Abstract
Elevated levels of plasma pentraxin 3 (PTX3), a marker of inflammation, are associated with the risk of developing cardiovascular diseases in the general population, as well as in patients with type 2 diabetes (DM2). In this study, we aimed to determine factors associated with PTX3 serum concentrations in men and women with DM2. The study included 116 consecutive patients (67 men and 49 women) with DM2 from an outpatient diabetic clinic. Men were characterised by lower age and higher uric acid, creatinine and bilirubin concentrations and waist/hip ratio than women. In women, low-density lipoprotein cholesterol (LDL-C) levels were higher than in men. In men, median (interquartile range) values of PTX3 concentration were 4.02 (1.99), and in women they were 4.53 (3.31) ng/ml (NS). In men, PTX3 concentrations correlated with total cholesterol (TC), triglycerides, apolipoprotein (Apo) C3, Apo B48, Glc and creatinine levels. In women, PTX3 correlated significantly with TC and LDL-C and Apo B100. Partial regression analysis revealed that after adjusting for age, PTX3 concentrations in men were significantly associated with TC, LDL-C, triglycerides, creatinine, Apo C3 and Apo B48, while in women they were associated with TC, LDL-C and Apo B100. The results could be of importance in sex-specific prevention of vascular complications in DM2 patients.
Introduction
Cardiovascular complications are the main cause of morbidity and mortality in diabetes patients, being two to three times higher than in the non-diabetic population.1,2 Women with diabetes have greater increases of cardiovascular risk, myocardial infarction and stroke mortality than men compared to non-diabetic subjects.1,2 Diabetes appears to attenuate the protective effect of the female sex in the development of cardiac diseases and nephropathy. 3
There is growing evidence that vascular changes in type 2 diabetes (DM2) are associated with subclinical inflammatory status and insulin resistance/metabolic syndrome features. Inflammatory markers, such as C-reactive protein and pentraxin 3 (PTX3), are prognostic factors of cardiovascular events and are also involved in the pathogenesis of vascular changes.4,5 PTX3 is an essential component of innate immunity and a member of the long pentraxin superfamily, which are soluble proteins induced by various inflammatory stimuli.6,7 Several clinical investigations have demonstrated that elevated plasma PTX3 levels are associated with the risk of developing cardiovascular diseases (CVD).5,8 PTX3 represents a specific and sensitive marker connecting inflammation with CVD being expressed and released by most cell compartments (macrophages and vascular cells) involved in the onset and progression of CVD. 8
The reasons that diabetes is a stronger risk factor for vascular disease in women compared to men are not clear. Several possible mechanisms, such as genetic and epigenetic as well as sex hormones effects, influencing body composition, vascular function and inflammatory responses, may be involved in sex differences in vascular complications in patients with diabetes. Another interesting mechanism is the role of immune system activation during obesity which links adiposity to subclinical inflammation and metabolic syndrome.3,9 Data from animal studies suggest that sex differences also exist in immune responses. 10 The elucidation of mechanisms of sex difference in DM2 vascular complication, regarding the novel inflammation marker risk factor PTX3, could potentially contribute to more personalised diabetes care. The aim of this study was to assess factors associated with the inflammatory cardiovascular marker PTX3 in men and women with DM2.
Material and methods
In this cross-sectional study conducted between 2014 and 2017, we enrolled consecutive patients with DM2, treated in the outpatient diabetic clinic of the Department of Metabolic Diseases, Jagiellonian University Medical College (Krakow, Poland). All consecutive patients referred to the clinic due to poor glycaemic control were invited to participate. In each patient standardised questionnaire, including data on past history, treatment, presence of diabetes complication, diabetes duration, family history and habits were evaluated. Data regarding patient medical history were collected by patient interviews and were also checked in medical files. All patients underwent physical examinations, and anthropometric measurements were performed. Central obesity was defined as a waist circumference > 94 cm in men and > 80 cm in women. Arterial hypertension was defined as blood pressure values >140/80 or taking hypertensive treatment; hyperlipidaemia was defined as low-density lipoprotein cholesterol (LDL-C) > 2.6 mmol/l or triglyceride >1.7 mmol/l or taking hypolipidaemic drugs. Smoking habit was assessed by questionnaire.
Blood was taken after an overnight fast. Laboratory tests, including fasting serum lipids, Glc, glycated haemoglobin A1c (HbA1c), PTX3 and apolipoproteins (Apo) A1, B100, B48 and C3, were performed. Serum fasting lipids concentrations were determined by enzymatic methods (Cobas 8000 Analyzer; Roche Diagnostics, Mannheim, Germany), HbA1c by HPLC (Bio-Rad Laboratories, Inc., Hercules, CA) and PTX3 by sandwich ELISA using a commercial reagent kit following the manufacturer instructions (#SEK411Hu; Cloud-Clone Corp., Houston, TX). Apo A1 was determined by immunoturbidimetry (APTEC Diagnostics NV, Sint-Niklaas, Belgium), and Apo C3, Apo B100 and Apo B48 by sandwich ELISA kits (human Apo C3: # KA0465, Abnova Co., Taipei City, Taiwan; human Apo B100: SEA603Hu, Cloud-Clone Corp., Houston, TX; and human Apo B48: #AKHB48, Shibayagi Co., Shibukawa, Japan) according to the manufacturers’ instructions.
Serum fasting lipids concentrations were determined by enzymatic methods: HbA1c by HPLC, and PTX3 by ELISA using Cloud-Clone Corp. reagents. Apo A1 serum concentrations were determined by immunoturbidimetry, and Apo B100, Apo B48 and Apo C3 by ELISA.
Descriptive statistics, correlation and regression analyses were performed. Statistical analysis included calculations of means (X) and standard deviations (SD) for normally distributed variables and medians (Me) and (interquartile range (IQR)) for not normally distributed variables and calculations of Pearson’s and Spearman’s correlation coefficients. Regression analysis with PTX3 as the dependent variable was performed after logarithmic transformation of PTX3 because of large skewness of its distribution. The independent variables in regression analysis were: body mass index (BMI), waist/hip ratio (WHR), serum concentration of total cholesterol (TC), triglycerides (TG), high-density lipoprotein cholesterol (HDL-C), LDL-C, Glc, creatinine, HbA1c, activity of alanine and asparagine aminotransferases (AST, ALT) and γ-glutamyltranspeptidase (GGTP) for each variable separately. The regression analysis adjusted for age had been calculated in the whole examined group and in the subgroups divided according to sex. Five models of backward stepwise regression analysis with PTX3 as the dependent variable were performed after logarithmic transformation of PTX3 (logPTX3). The independent variables in regression analysis were: Apo C3, Apo B100 and, depending on the model, HDL-C and BMI for model 1, HDL-C and waist circumference for model 2, BMI and Apo A1 for model 3, Apo A1 and waist circumference for model 4 and Glc and creatinine for model 5. The analysis adjusted for age had been calculated separately in men and women.
Written informed consent was obtained from each patient included in the study. The study protocol conforms to the local ethical guidelines and was approved by the Jagiellonian University Collegium Medicum ethics committee on research on humans.
Results
We examined 116 patients (67 men and 49 women) with DM2 from a diabetes outpatient clinic. Clinical and biochemical characteristics of the examined patients are presented in Table 1. Of these, 59.8% of patients were treated with statins, and 55.7% were on insulin therapy. The mean age of the patients was 59.1 yr (11.07 yr), and the mean diabetes duration was 9.3 yr (7.49 yr). Glc control, measured by glycated HbA1c, was similar in both men and women. Men were younger (P = 0.0153) and were characterised by significantly higher uric acid (P = 0.0283), creatinine (P < 0.001) and bilirubin (P = 0.0179) concentrations, and higher WHR (P < 0.001) than women. In women, LDL-C levels were higher than in men (P = 0.0228). In men, median (IQR) values of PTX3 were 4.02 ng/ml (1.99 ng/ml), and in women they were 4.53 ng/ml (3.31 ng/ml; NS; Table 1).
Characteristics of selected variables in the patients with type 2 diabetes according to sex.
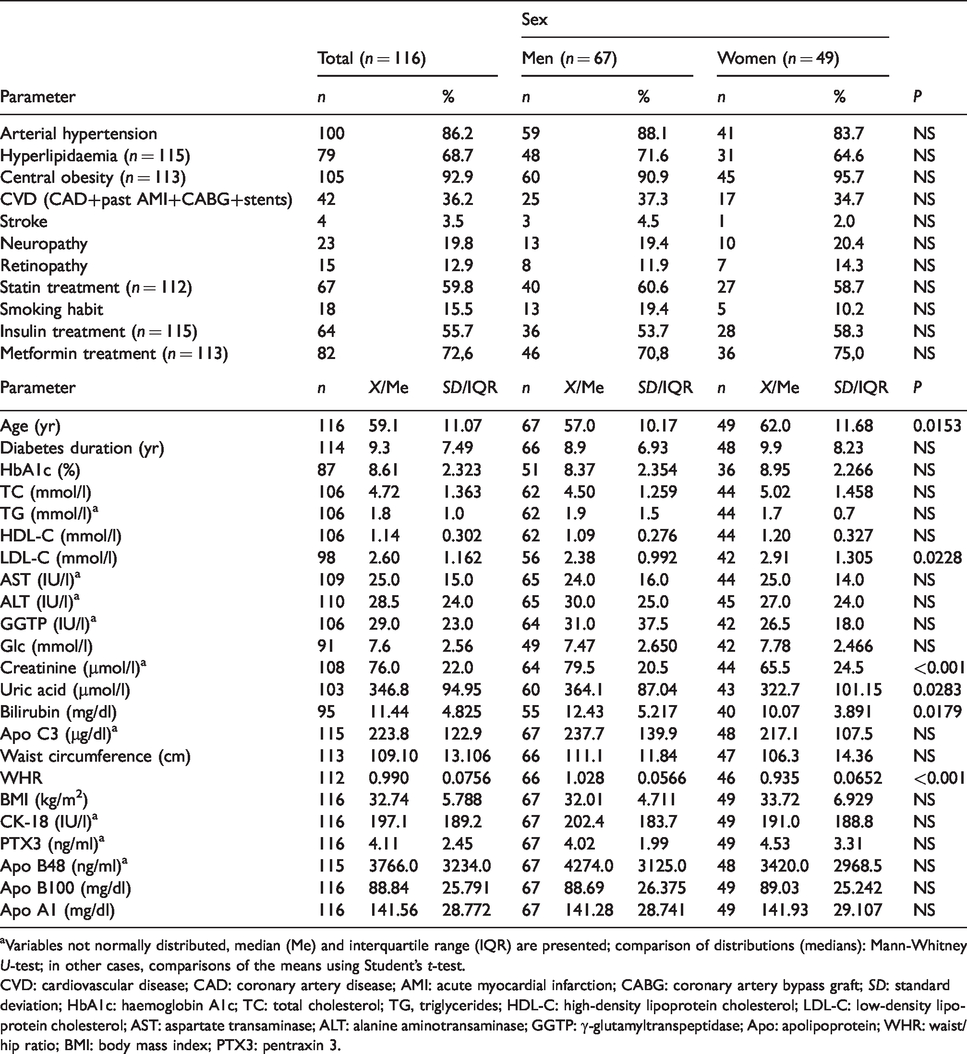
aVariables not normally distributed, median (Me) and interquartile range (IQR) are presented; comparison of distributions (medians): Mann-Whitney U-test; in other cases, comparisons of the means using Student’s t-test.
CVD: cardiovascular disease; CAD: coronary artery disease; AMI: acute myocardial infarction; CABG: coronary artery bypass graft; SD: standard deviation; HbA1c: haemoglobin A1c; TC: total cholesterol; TG, triglycerides; HDL-C: high-density lipoprotein cholesterol; LDL-C: low-density lipoprotein cholesterol; AST: aspartate transaminase; ALT: alanine aminotransaminase; GGTP: γ-glutamyltranspeptidase; Apo: apolipoprotein; WHR: waist/hip ratio; BMI: body mass index; PTX3: pentraxin 3.
In men, PTX3 concentrations correlated significantly positively with TC (r = 0.40, P = 0.0012), TG (r = 0.51, P < 0.001), Apo C3 (r = 0.48, P < 0.001), Apo B48 (r = 0.34, P = 0.0048), Glc (r = 0.35, P = 0.0128) and creatinine (r = 0.32, P = 0.0092) levels. In women, PTX3 correlated significantly with TC (r = 0.53, P = 0.0002), LDL-C (r = 0.50, P = 0.0008) and Apo B100 (r = 0.41, P = 0.0033; Table 2).
Spearman’s/Pearson’s correlation coefficients between selected variables and PTX3 serum concentrations in patients with type 2 diabetes according to sex.
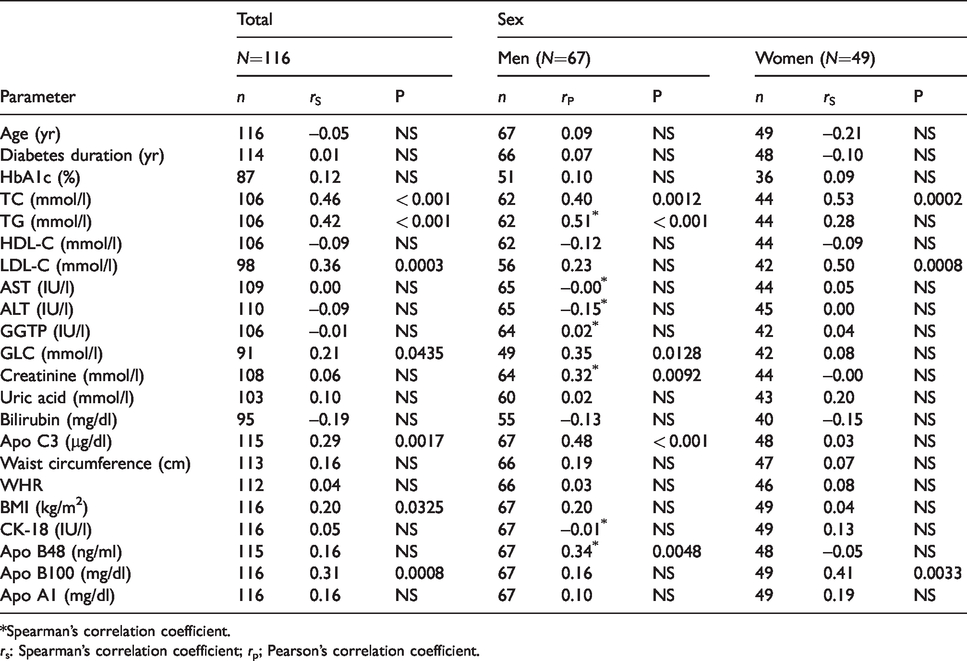
*Spearman’s correlation coefficient.
rs: Spearman’s correlation coefficient; rp; Pearson’s correlation coefficient.
Regression analysis, examining the associations of selected variables with logPTX3, adjusted for age and statin use revealed that in men, apart from observed associations, there was borderline statistically significant association with Apo B100 (P = 0.0487), while after adjustment for age and metformin use, the association between PTX3 and LDL-C was not significant (P = 0.0665; adjustment for age only: P = 0.0498, borderline significance).
In women, we did not observe any changes in statistical associations after adjusting for statin and metformin treatment.
Partial regression analysis revealed that after standardisation by age, PTX3 concentrations in men were significantly associated with TC, LDL-C, TG, creatinine, Apo C3 and Apo B48, while in women they were associated with total and LDL-C and Apo B100 (Table 3). In men, an increase of TC and TG by 1 mmol/l and an increase of Apo C3 by 1 μg/dl were related to an increase of PTX3 by 1.1620 ng/ml, 1.1612 ng/ml and 1.0018 ng/ml, respectively. In women, an increase of LDL-C by 1 mmol/l and of Apo B100 by 1 mg/dl were related to an increase of PTX3 by 1.2671 ng/ml and 1.0081 ng/ml, respectively (Table 3).
Partial regression coefficients (b) and partial correlation coefficients (r) between selected variables and logPTX3 in patients with type 2 diabetes mellitus according to sex, after adjusting for age.
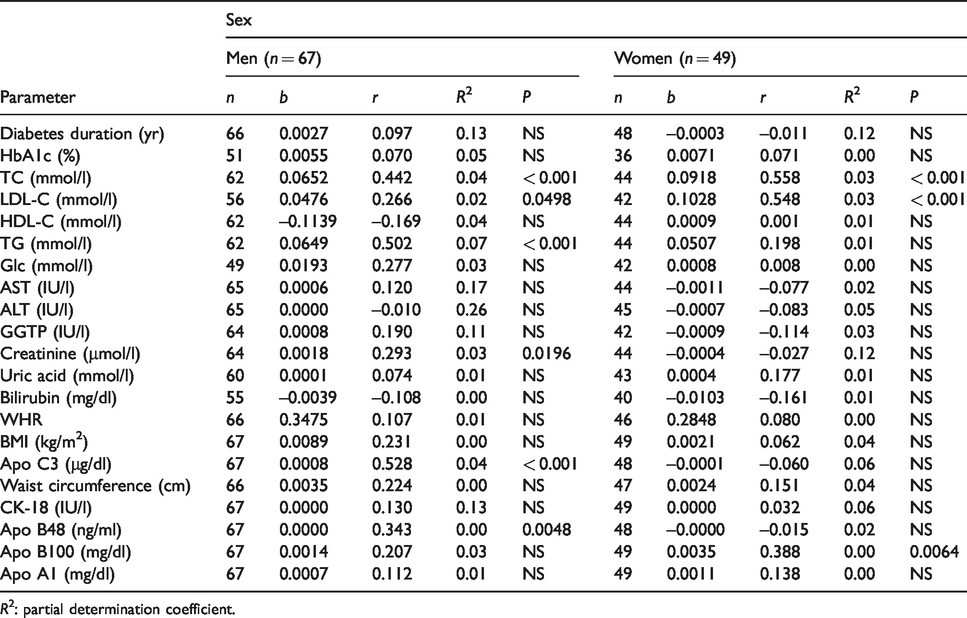
R2: partial determination coefficient.
Five models of backward stepwise regression analysis, with logPTX3 as the dependent variable, were performed. Regardless of which variables were introduced into the model, in men, a significant relationship occurs only between Apo C3 and logPTX3, and in women between Apo B100 and logPTX3. In men, in each model, the partial regression coefficient was 0.001, which means that an increase of Apo C3 by 1 μg/dl was related to an increase of PTX3 by 1.0023 ng/ml (P < 0.001). In women, in each model, the partial regression coefficient was 0.004, which means that an increase of Apo B100 by 1 mg/dl was related to an increase of PTX3 by 1.0093 ng/ml (P < 0.01).
We did not find any correlations between PTX3 and glycaemic control, transaminases, GGTP or obesity parameters.
Discussion
In this study, we found that PTX3, an inflammatory cardiovascular risk marker, in DM2 patients was strongly associated with lipid and apolipoprotein risk factors. Interestingly, PTX3 associations were different in men and women with DM2. In both sexes, significant correlations were observed with TC. However, in men, serum PTX3 correlated with TG, Apo C3 and Apo B48, apolipoproteins involved in triglyceride metabolism, while in women it was correlated with LDL-C and Apo B100 concentrations. Backward stepwise regression analysis confirmed that in men, a significant relationship occurs only between Apo C3 and logPTX3, and in women between Apo B100 and logPTX3.
Apo B100 is present in all atherogenic lipoproteins – very-low-density lipoproteins (VLDL), LDL and small-density LDL – and is a strong cardiovascular risk factor. Positive associations between PTX3 and LDL-C were observed by Hudzik et al. in patients at different stages of CAD. 11 However, contrary to our findings, significant negative associations between LDL-C and PTX3 were observed in women who developed gestational diabetes mellitus 12 and in insulin-resistant subjects from the Health 2000 Survey population. 13 Furthermore, in a group of 1747 Korean patients in a community-based cohort study, the PTX3 level was negatively associated with the LDL-C/HDL-C ratio. 14
In our study, women were characterised by higher LDL-C than men, which could promote LDL-C oxidative modification and increase PTX3 expression. Evans et al. found that compared to diabetic men, diabetic women may have greater levels of lipid peroxidation, independent of glycaemic control. 15
The positive association between PTX3 and Apo C3 levels is of importance, especially in the light of the role as an independent predictor of incident CVD in DM2 patients. Apo C3 is found in HDL, VLDL and LDL and is involved in atherosclerosis progression. In the Bruneck Study, lipidomic and proteomic data implicated Apo C3, as component of VLDL, in de novo lipogenesis, Glc metabolism, complement activation, blood coagulation and inflammation.16,17 Some data indicate that Apo C3 is directly involved in stimulation of vascular inflammatory processes by provoking pro-inflammatory responses in vascular cells, including monocytes and endothelial cells.18,19
Our observations that the cardiovascular predictor PTX3 is associated with TG and apolipoproteins found on triglyceride-rich lipoproteins in men is in line with data from the ACCORD lipid trial, in which fenofibrate added to a HMG-CoA reductase inhibitor reduced cardiovascular risk exclusively in men. 20 Also, in the study by Krysiak et al., the effect of simvastatin/fenofibrate combination therapy on IL-6 and MCP-1 was more pronounced than that of simvastatin or ezetimibe administered alone only in men. 21
Apo B48 is a marker of triglyceride-rich lipoproteins of the intestine and is a prognostic factor of vascular risk. Apo B48 containing chylomicron remnants may be responsible for postprandial leucocyte activation in the circulation.22,23
There are some data indicating that prevalence, progression and pathophysiology of both microvascular and macrovascular disease are different in the two sexes: women appear to be at a higher risk for macrovascular complications, while for men, the risk is for diabetic microvascular complications. However, understanding the underlying mechanisms of sex differences in the pathophysiology of diabetic vascular complications raises many controversies.3,24,25 Furthermore, data on inflammation biomarkers and sex in patients with diabetes are scarce. Evidence from animal models and from human studies suggests that sex differences exist in immune responses and therefore could be a possible mechanism leading to sex differences in vascular complications.21,26–29 Opstad et al. found that there is different association between chronic low-grade inflammation and leucocyte telomere length. 26 Some data indicate that sex is a critical factor in obesity outcomes, with men having more metabolic complications compared to women.28,29 The role of obesity in activating the immune system and insulin resistance is an important factor contributing to metabolic syndrome and atherogenic dyslipidaemia.
PTX3 based on the kind of cell phenotype which produce PTX3 could serve as a potential modulator of atherosclerosis. Thus, information on its associates could be of value in personalised and sex-specific treatment for diabetic macro- and micro-vascular disease prevention. Interestingly, in our cohort of DM2 patients, we found significant associations between PTX3 and atherogenic lipids and Apo B100 and Apo C3 levels in patients with non-alcoholic fatty liver disease, further supporting PTX3 as marker of increased vascular risk. 30
Conclusion
The results indicate that PTX3 associations are different in men and women with DM2. In men, the strongest association of PTX3 among examined variables is with Apo C3, while in women it is with Apo B100. In both sexes, there is a significant association between PTX3 and TC, while in men there is also a significant association with TG, Apo B48, Glc and creatinine. The results of our study suggest that there are different correlations between inflammation marker PTX3 and the examined lipids and apolipoproteins in men and women, which could potentially be of importance in the prevention of vascular complications in these patients.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.