
Abstract
To overcome the lack of availability of fresh human whole blood for pyrogen detection, we explored the feasibility of utilizing cryopreserved pooled human blood to detect the responses of the pro-inflammatory cytokines IL-6 and IL-1β to LPS. Whole blood was obtained from five donors and incubated with LPS. The quantities of pro-inflammatory cytokines were measured using ELISA, and the results were compared among the samples. After the blood was cryopreserved with Dimethyl sulfoxide (DMSO) (10% v/v) and stored for 4 mo at –196℃, the detection limits of the IL-6/IL-1β responses to LPS were 0.2/0.4 endotoxin units (EU)/ml, respectively, and IL-6/IL-1β release increased in response to LPS in a dose-dependent manner. When these experiments were performed in three separate laboratories, the within-laboratory reproducibility of the IL-6/IL-1β responses was 100%/86.7%, 93.3%/100%, and 86.7%/80%, and the inter-laboratory reproducibility was 92.9%/85.7%, 64.3%/63.6%, and 57.1%/66.7%, respectively. The sensitivity (the probability of correctly classifying positive samples) and specificity (the probability of correctly classifying negative samples) of the IL-6/IL-1β tests were 81.7%/82.5% and 100%/100%, respectively. The results of this study suggest that cryopreserved pooled blood is a convenient and viable alternative for evaluating in vitro pyrogenicity. Additionally, maintaining cryopreserved pooled blood promotes safety for the user because it is released only after pretesting for infection parameters and has lower variation than fresh donations from a variety of donors.
Introduction
Pyrogens are a class of chemically heterogeneous, fever-inducing substances that are produced by Gram-negative and -positive bacteria, viruses, fungi and other sources.1-3
As contaminants, pyrogens can stimulate immune cells (e.g. monocytes and macrophages) to release pro-inflammatory cytokines, such as IL-1β, IL-6, and TNF-α, which are often termed endogenous pyrogens, and can transmit fever reactions through an organism to the thermoregulatory centres of the brain.2,4,5
Currently, only two pharmacological tests, including the rabbit pyrogen test and the bacterial endotoxins test (BET), are applied to evaluate pyrogenic contamination in parenteral pharmaceuticals by the Chinese Pharmacopoeia (ChP). 6 Although generally reliable, both of these assays have shortcomings.7-9 The rabbit test is not quantitative but is expensive and involves the use of animals. It can also produce varying responses depending on the strain, age, and housing conditions of the rabbits. The BET, however, does not detect pyrogens other than Gram-negative bacterial endotoxins and is often problematic when used to test solutions with a high protein content. Horseshoe crabs are required to obtain an important reagent for the BET, and horseshoe crab populations are declining as a result of unreasonable use and capture, habitat loss, and pollution.
To overcome these shortcomings and satisfy the growing need for new methods prompted by the constantly increasing production of biological compounds and medical devices by successful ventures in biotechnology and nanoscience, 10 a number of assays have been developed for pyrogen detection that are based mainly on the use of human monocytes and macrophages, such as leucocyte cell lines (e.g. THP1,1,11 MM6,12,13 and 28SC 14 ), human PBMCs10,15,16 and human whole blood.17-21
In some cases, PBMCs (especially when combined with FCS and used to distinguish between vaccines containing penta- and tetra-acylated LPS 22 ) or monocytic cell lines (which express relatively few kinds of specialized PRRs) do not behave the same as whole blood. An assay based on human whole blood could exploit natural human reactions to pyrogens. 23 However, the widespread application of such methods is limited by regulatory and practical restrictions that are related primarily to the use of fresh human blood and associated phlebotomy techniques. 10 We have also identified promising inter-individual variations in fresh blood obtained from single donors. The main aim of the present study was therefore to evaluate the feasibility of utilizing cryopreserved pooled human blood to detect the levels of the pro-inflammatory cytokines IL-6 and IL-1β following stimulation with LPS.
Materials and methods
Reagents
The national standard for bacterial endotoxins is LPS, which was obtained from Escherichia coli O55:B5 (9000 EU/vial, batch 981, identical to the 2nd international WHO standard for endotoxin 94/580 from E. coli O113: H10) and provided by the National Institutes for Food and Drug Control (NIFDC). RPMI-1640 (Gibco, Cat # 11875119) was used to dilute all reagents and samples. DMSO (Sigma-Aldrich, Cat # D2650) was used as a blood cryoprotectant. The following reagents were also used: heparin sodium for injections (ChangZhou Qianhong Co.), human immunoglobulin (pH 4) for intravenous injections (Shanghai Xinxing Co.), recombinant hepatitis B vaccine (Yeast) (Biokangtai Co.), polyethylene glycol IFN-α2β for injection (pegIFN-α2β) (Changchun Heber Biological Technology Co., LTD), a solution of human albumin for infusion (Octapharma AB), and a rabies vaccine (Vero Cell) for human use that was freeze-dried (Liao Ning Yi Sheng Bio-Co).
Consumables
The following were used for these experiments: 24-well cell culture plates (Corning, Cat # 3524, sterile, non-pyrogenic, polystyrene), 2-ml cryogenic vials (Corning, Cat # 430659, sterile, non-pyrogenic, polypropylene), 50-ml centrifuge tubes (Corning, Cat # 430828, sterile, non-pyrogenic, polypropylene), and human IL-6 and IL-1β ELISA kits (Xin Bo Sheng Co.). Other reagents/materials were purchased as sterile and pyrogen-free, and glassware was incubated at 250℃ for 1 h.
Collection of blood
Blood samples were collected from healthy volunteers (n = 5) from whom the following were excluded: infection with HIV, hepatitis B virus (HBV), and the consumption of drugs known to influence the production of cytokines. A 20-ml syringe that contained heparin at a concentration of 15 U/ml blood was used to obtain 10–15 ml of blood that was drawn from the vein of the left of right arm of each donor.1,18 The blood was then immediately transferred into a 50-ml centrifuge tube, each of which contained an equal proportion of the samples. The centrifuge tubes were gently mixed.
Cryopreservation and thawing of whole blood samples
DMSO (10% or 15%, v/v) was added slowly drop-by-drop to tubes containing 30 ml of pooled whole blood while the tubes were gently swirled. The mixture was then rapidly aliquoted into cryovials (1.8 ml/cryovial). The samples were frozen under gradient conditions and then transferred into a liquid nitrogen tank if necessary.
Before the cytokine induction assays were performed, the cryopreserved blood was thawed in a water bath at 37℃ for 3 min and then transferred to a 50-ml centrifuge tube while gently swirling.
Shipment
The required number of aliquots of frozen blood was shipped to other laboratories in a transporter containing liquid nitrogen (Chengdu Shengjie Cryogenic Equipment Co., Ltd, Chengdu, China). After arrival, the aliquots were transferred to a nitrogen tank in each laboratory.
Protocol for human whole blood tests
Cultures (600 µl) were set up in quadruplicate in 24-well plates. A 600 µl volume of the sample was added to wells containing the following: 500 µl RPMI-1640, 50 µl thawed whole blood, and 50 µl sample/control.1,17
The contents of the wells were mixed 3–5 times by aspirating and expelling 100 µl of the solution.16,24 This technique was also used to make the culture medium homogeneous after incubation. The wells were incubated at 37℃ in an atmosphere of 5% CO2 in air for a period of up to 22 h. The supernatants were then assayed to determine the levels of IL-6 and IL-1β with commercial ELISA kits.
Statistical analysis
The data are expressed as the mean and SEM. The detection limit of the IL-6/IL-1β response to LPS was calculated as the minimum concentration of LPS that induced a significant amount of cytokine (IL-6 or IL-1β) production. Significance was defined as a P value below 0.01 and an amount greater than 3 SD above that obtained in the negative control. 25
Results
IL-6 and IL-1β release from pooled blood cryopreserved with 10% or 15% (v/v) DMSO
The results of this experiment are shown in Figure 1. The data showed that when blood was cryopreserved with 10% DMSO, the release of IL-6 was 1.8-fold (0.125 EU/ml LPS), 15.1-fold (0.25 EU/ml LPS), and 40.7-fold (0.5 EU/ml LPS) higher than the level observed at 0 EU/ml, which had an OD of approximately 0.1 under all conditions used in the study, and all of these differences were significant. When 15% DMSO was used, the release of IL-6 in response to 0.25 and 0.5 EU/ml of LPS was not significantly different from the level observed in the control (0 EU/ml).
The amounts of IL-6 (a) and IL-1β (b) released after treatment with 0.125, 0.25 and 0.5 EU/ml LPS for 22 h. The levels were detected with ELISA using pooled blood cryopreserved with 10% or 15% DMSO at –80℃ for 1.5 mo. **P<0.01 vs. 0 EU/ml, *P<0.05 vs. 0 EU/ml. #P>0.05 vs. 0 EU/ml.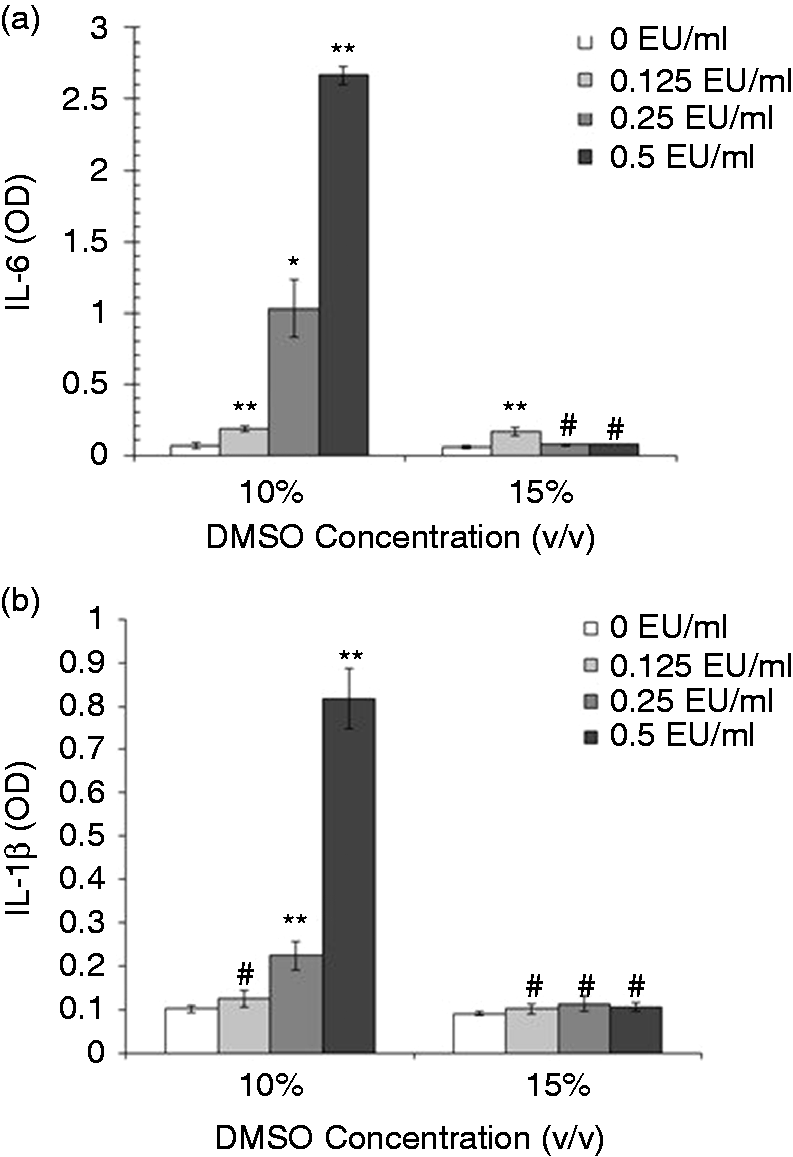
In the LPS-treated groups, when blood cryopreserved with 10% DMSO was used, the release of IL-1β was 1.2-fold (0.25 EU/ml LPS) and 7.1-fold (0.5 EU/ml LPS) higher than that observed in response to 0 EU/ml LPS. When 15% DMSO was used, the release of IL-1β in response to 0.125, 0.25, and 0.5 EU/ml LPS was not significantly different from the level induced by 0 EU/ml.
IL-6 and IL-1β release from pooled cryopreserved blood stored at –196℃ and –80℃
The results of this experiment are shown in Figure 2. The data show that when cryopreserved blood stored at –196℃ was used, the release of IL-6 was significantly higher by 8.6-fold (0.25 EU/ml LPS) and 19.9-fold (0.5 EU/ml LPS) over the level observed in the samples treated with 0 EU/ml. When the blood was stored at –80℃, the release of IL-6 in response to 0.25 and 0.5 EU/ml LPS was significantly increased by 0.9-fold and 2.8-fold, respectively, over the level observed in the group treated with 0 EU/ml LPS.
IL-6 (a) and IL-1β (b) release after treatment with 0.25 and 0.5 EU/ml LPS for 22 h. Levels were detected with ELISA in pooled blood cryopreserved with 10% DMSO at –196℃ or –80℃ for 3 mo. **P<0.01 vs. 0 EU/ml. *P<0.05 vs. 0 EU/ml. #P>0.05 vs. 0 EU/ml.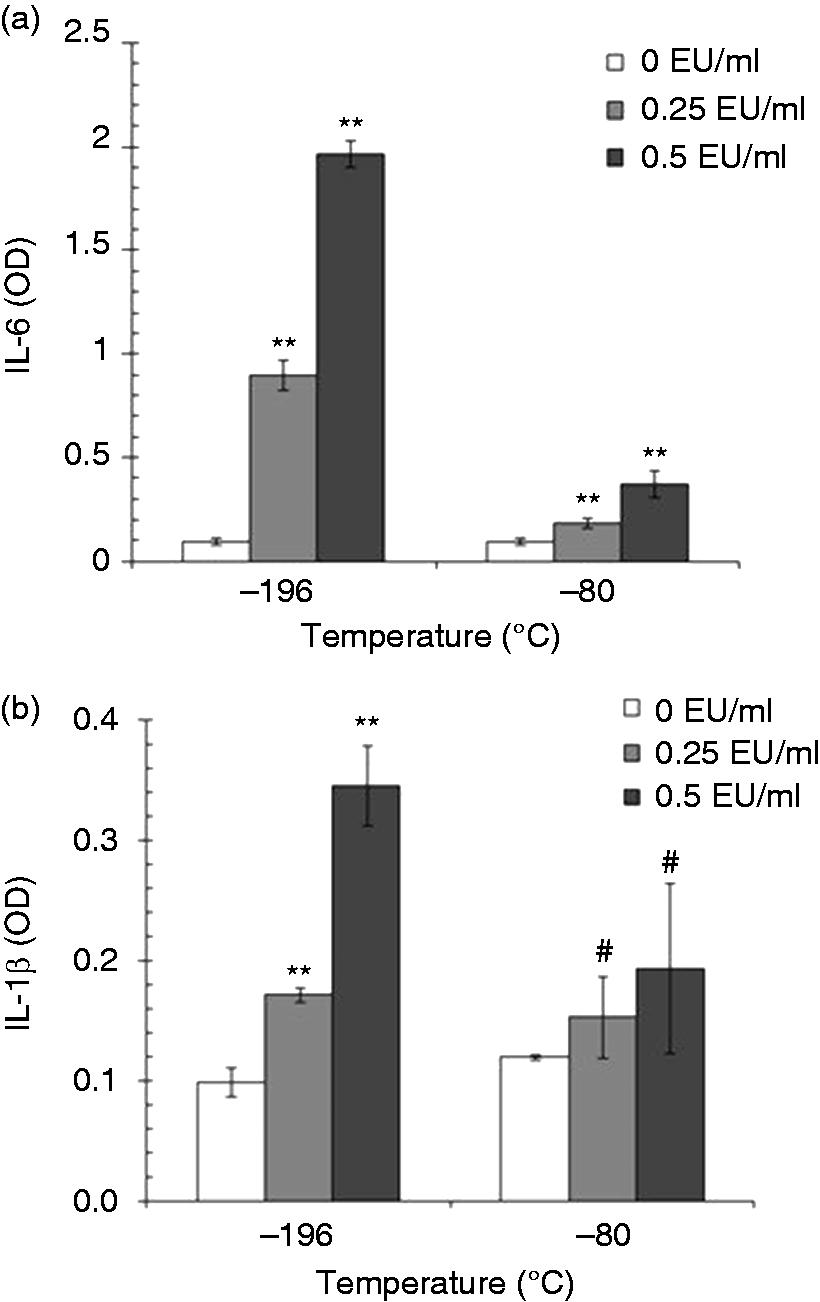
When cryopreserved blood stored at –196℃ was used, the release of IL-1β was significantly increased by 0.7-fold (0.25 EU/ml of LPS) and 2.5-fold (0.5 EU/ml of LPS) over the level observed in the 0 EU/ml LPS group. However, when the samples were stored at –80℃, there was no significant difference in the release of IL-1β among the 0, 0.25, and 0.5 EU/ml LPS groups.
IL-6 and IL-1β release from pooled cryopreserved blood after storage for 1.5, 3, 6 and 12 mo
The results of this experiment are shown in Figure 3. The data show that when cryopreserved blood was stored for 1.5, 3, 6, and 12 mo, the release of IL-6 in response to 0.5 EU/ml LPS was increased significantly by 55.1 -, 19.9 -, 23.1 - and 5.8-fold, respectively, over the level observed in the 0 EU/ml groups. Under the same conditions, the release of IL-1β was significantly increased by 10.7-fold (1.5 mo), 2.5-fold (3 mo), and 1.6-fold (6 mo after storage) over the level observed in the 0 EU/ml groups.
IL-6 (a) and IL-1β (b) release after treatment with 0.5 EU/ml LPS. Levels were detected with ELISA in pooled blood cryopreserved in 10% DMSO at –196℃ for 1.5, 3, 6 and 12 mo. **P<0.01 vs. 0 EU/ml. *P<0.05 vs. 0 EU/ml. #P>0.05 vs. 0 EU/ml.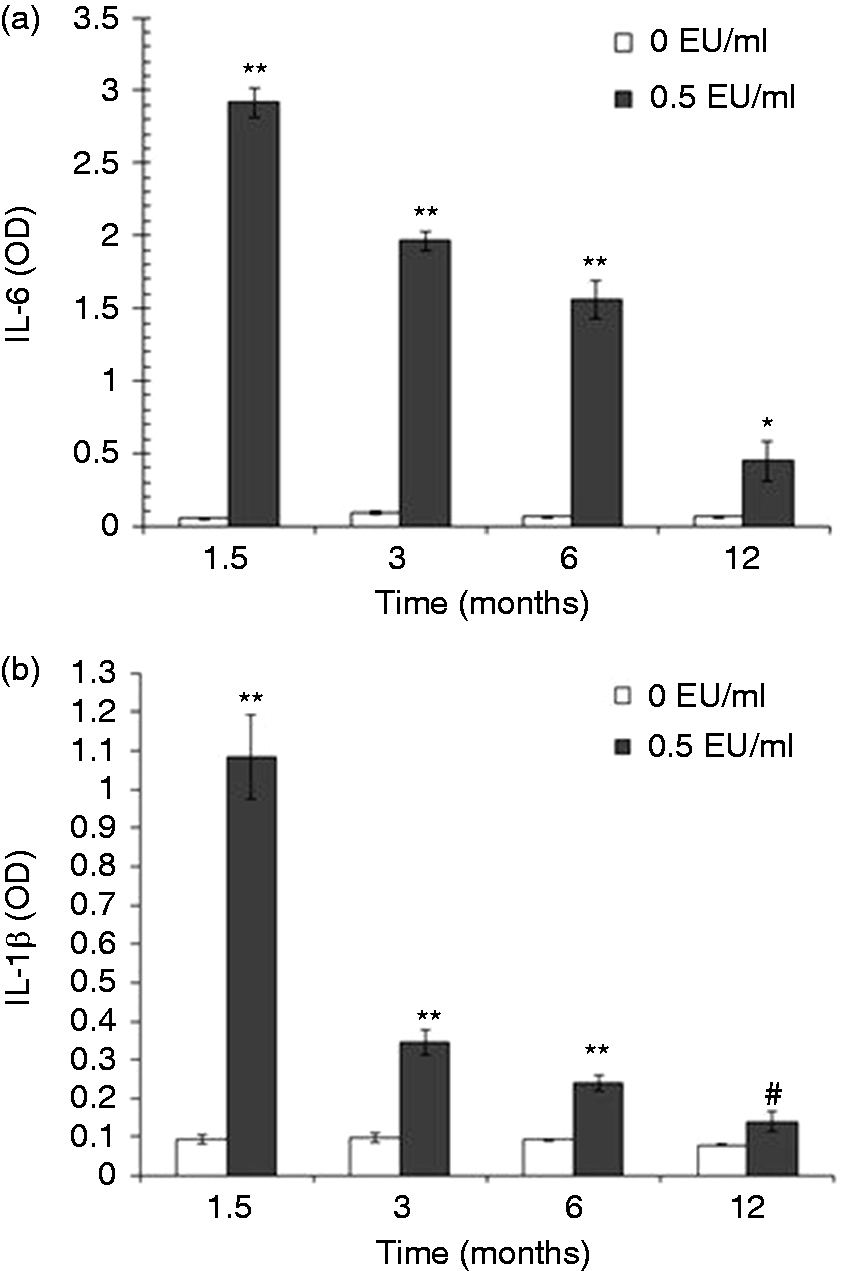
Detection limit of the IL-6 and IL-1β responses to LPS and the dose-dependent relationship between the release of the cytokines IL-6 and IL-1β and LPS concentrations
The results of this experiment are shown in Figure 4. The data show that the detection limits of IL-6 and IL-1β responsiveness to LPS were 0.2 and 0.4 EU/ml, respectively, and the release of both cytokines increased in a dose-dependent manner in response to the concentration of LPS (range, 0.2–1.6 and 0.4–1.6 EU/ml, respectively). When the quantitative BET is used,
6
it is necessary to exclude interference in the secretion of cytokines (IL-6 and IL-1β). As the detection limit of the test decreases, the fold-dilution of the sample increases.
IL-6 and IL-1β release after treatment with 0.2, 0.4, 0.8, 1.0, and 1.6 EU/ml LPS for 22 h. Levels were detected with ELISA in pooled cryopreserved blood stored with 10% DMSO at –196℃ for 4 mo (n = 4). **P<0.01 vs. 0 EU/ml.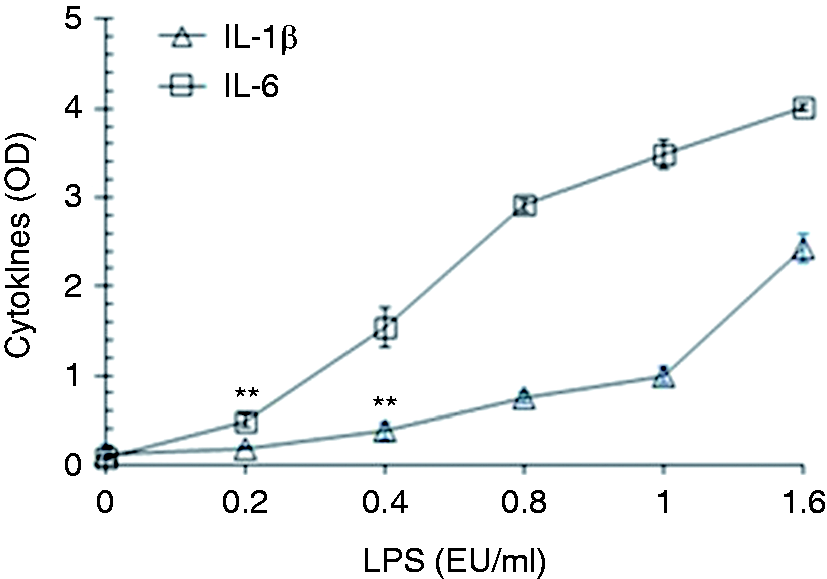
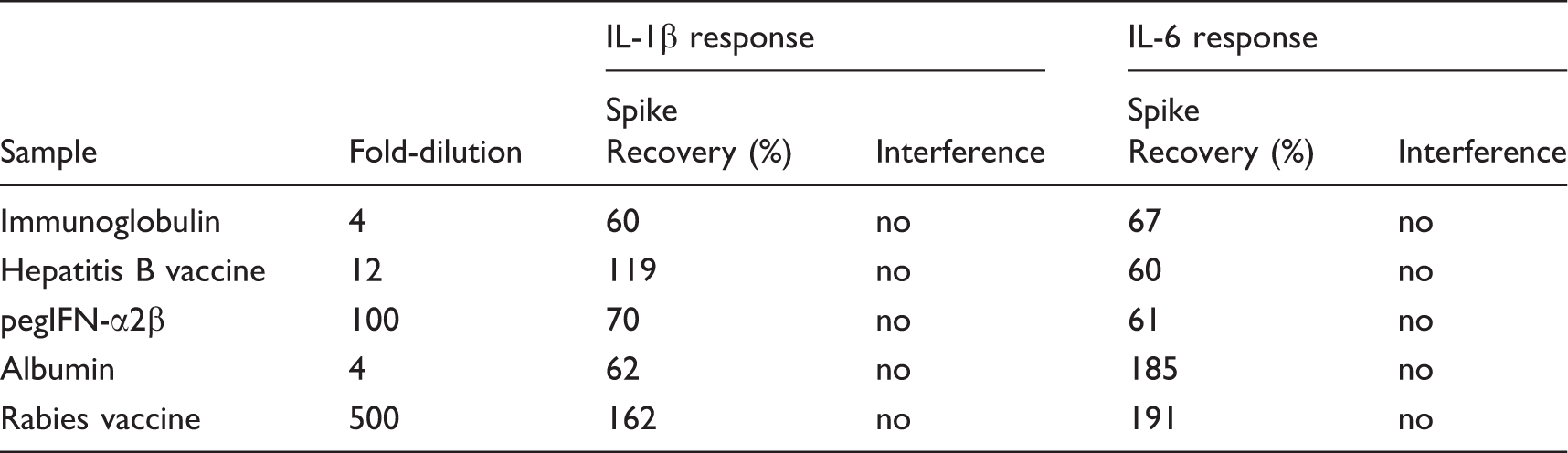
Application of IL-6 and IL-1β responses to samples
Recovery of LPS spike in samples in which the IL-6 and IL-1β response was measured in pooled cryopreserved blood.
Within/inter-laboratory reproducibility
The test system evaluated here was validated in three different laboratories after a detailed standard operating procedure was compiled and made available to them. Successful technology transfer was assessed in a prevalidation phase.
Three drugs (immunoglobulin, hepatitis B vaccine, and pegIFN-α2β) were tested at their MVD, each of which was calculated as the endotoxin limit concentration in EU/ml divided by the limit of detection (LOD, in this case 0.4 EU/ml).
Each drug presented five blinded spikes, two of which were defined as non-pyrogenic, meaning they were below 0.4 EU/ml (0 and 0.2 EU/ml), and three of which were pyrogenic (0.4, 0.8, and 1.0 EU/ml). These were tested in each of the different laboratories.
After the interference test was passed, the samples were classified by a so-called prediction model (PM), which classified the samples as non-pyrogenic when the responses were significantly lower than the 0.4 EU/ml control response (significance level, 1%). They were otherwise classified as pyrogenic.
The predictability of IL-6/IL-1β tests.
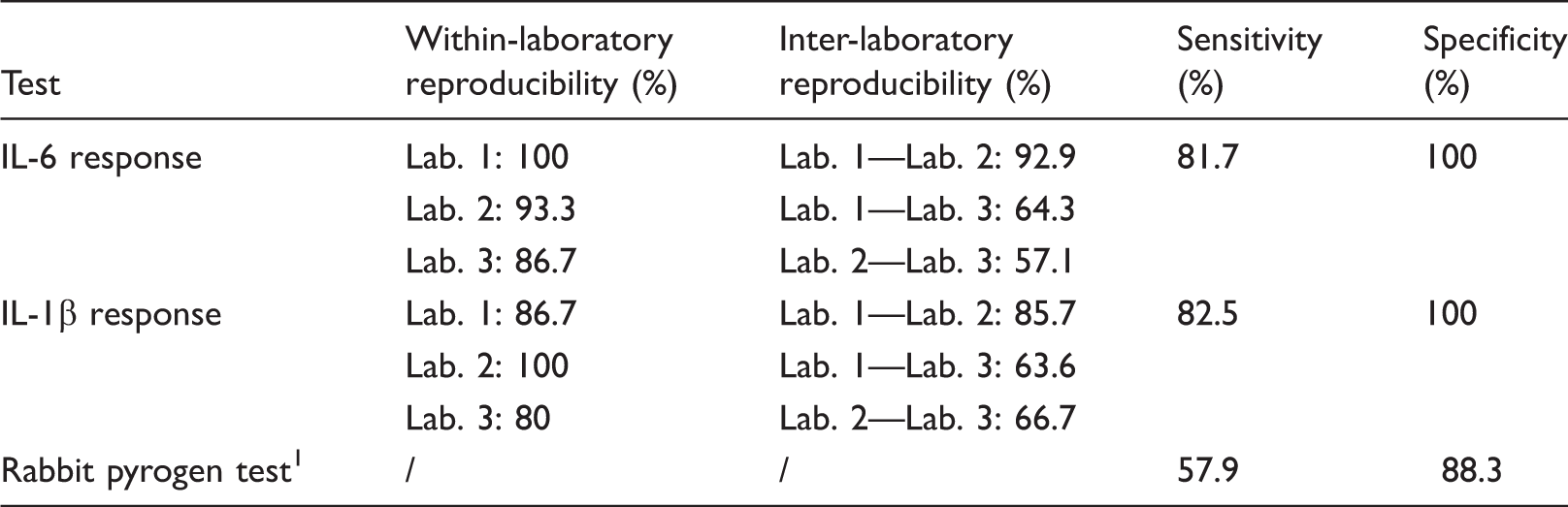
Lab. 1: Liaoning Provincial Institute for Food and Drug Control; Lab. 2: National Institutes for Food and Drug Control; Lab. 3: Tianjin Municipality Institute for Drug Control.
The relative SDs (RSDs) calculated by all laboratories were generally smaller than 25%. Only two standards and four samples (mainly from laboratory 1) resulted in an RSD larger than 45% (e.g. 57.9%, 48.7%, and 56.9%). 24 Data that exceeded that RSD value were tested to determine whether they were outliers with the Grubbs-test. An outlying replicate was found to have caused the excessive variation and was excluded. Further analyses were performed with the remaining three replicates.
Sensitivity/specificity
The PM was used to reflect the predictive capacity of novel tests, and the overall performances of both the IL-6 and IL-1β tests were better than those of the rabbit pyrogen test: the sensitivities (the probability of correctly classifying positive samples) of the IL-6/IL-1β responses were 81.7% (49/60) and 82.5% (52/63), respectively, and their specificities (the probability of correctly classifying negative samples) were 100% (38/38) and 100% (42/42), respectively.1,24
Discussion
The pro-inflammatory cytokines IL-1β, IL-6, and TNF-α are known to act as endogenous pyrogens, and IL-1β is the most efficient endogenous pyrogen. 26 IL-6 can leak from the peripheral to the central compartment and is a critical endogenous pyrogen that acts downstream of centrally localized IL-1β and TNF-α. 27 We also found that in fresh pooled blood, IL-1β and IL-6 responded much more strongly than TNF-α to stimulation with LPS. 28
In the present study, the feasibility of using pro-inflammatory cytokines (IL-6 and IL-1β) as markers for LPS-induced pyrogenicity in pooled cryopreserved human whole blood was evaluated.
The factors that affected the responses of the cytokines to LPS included the concentration of DMSO in the cryoblood (10% and 15% v/v), temperature (–196℃ and –80℃) and the duration of storage (1.5, 3, 6, and 12 mo). These experiments were carried out to determine the ideal freezing conditions for cytokine responses in cryoblood. Our results suggest that cryopreserved blood stored with 10% DMSO at –196℃ exhibited the best response to LPS when IL-6 and IL-1β were used as indicators. While the responses of both cytokines declined over time, significantly more IL-6 (after 12 mo of storage) and IL-1β (after 6 mo of storage) was released by the samples in response to stimulation with 0.5 EU/ml LPS than in the negative controls. In this assay, we found that 0.5 EU/ml was the detection limit in rabbits injected with the maximum permissible volume of 10 ml/kg LPS (data not shown), 6 in agreement with the 2nd international WHO standard for endotoxins. 1
Overall, the mean OD following IL-6 and IL-1β release in response to induction by 0 EU/ml LPS (negative control) was no greater than 0.1 in this study, indicating that neither the donors’ physical condition nor the cryopreservation procedure altered the level of these pro-inflammatory cytokines.
The results of the present study establish that in cryoblood, the response to LPS was more sensitive for IL-6 than for IL-1β when their detection limits and the OD of their release were compared under the same conditions. However, our previous study showed that when fresh pooled blood was used, the IL-1β response was more sensitive. 28
We also found that the release of these cytokines depended on the concentration of LPS after the samples were stored for 4 mo at –196℃. These data support the notion these types of samples can be stored over the short-term to provide a regular supply of non-allergic, pathogen-free human blood for the quantitative evaluation of in vitro pyrogenicity.
In conclusion, cryopreserved pooled blood is a convenient and viable alternative for evaluating in vitro pyrogenicity. In this study, we show that monocyte activation test (MAT) provides advantages that have prompted domestic authorities to attach an increasing amount of importance to the development of this trend in the field, and we believe that MAT will be adopted by the ChP in the future.
Footnotes
Acknowledgment
The authors are grateful to Ingo Spreitzer of Section 1/3 Microbial safety, Paul-Ehrlich-Institut, Langen, Germany, for providing suggestions and encouraging to the manuscript throughout.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by National Major New Drug Creation Project (Research on key technologies for the evaluation and standardization of innovative biotechnology drugs, SQ2018ZX090101).