
Abstract
A higher body mass index (BMI) appears to be associated with lower mortality in critically ill patients, possibly explained by an altered innate immune response. However, the precise relationship between BMI and the innate immune response in humans in vivo is unknown. We investigated the relationship between BMI and the systemic cytokine response during experimental human endotoxemia. Endotoxemia was induced in 112 healthy male volunteers by intravenous administration of 2 ng/kg Escherichia coli endotoxin. Plasma concentrations of TNF-α, IL-6, IL-10 and IL-1RA were serially determined. The relationship between BMI and the cytokine response, as well as body temperature, was investigated. The BMIs of the participants ranged from 18.3 to 33.6 kg/m2, (median: 22.7 kg/m2). All participants showed a marked increase in plasma cytokine levels [median (interquartile range)] peak levels: TNF-α 509 (353–673) pg/ml; IL-6 757 (522–1098) pg/ml; IL-10 271 (159–401) pg/ml; IL-1RA 4882 (3927–6025) pg/ml; and an increase in body temperature [1.8(1.4–2.2)℃] during endotoxemia. No significant correlations were found between BMI and levels of any of the cytokines or body temperature. No relationship between BMI and the cytokine response was found in healthy volunteers subjected to experimental endotoxemia. These data question the relationship between BMI and cytokine responses in critical illness.
Introduction
Obesity is an epidemic disease in Western society 1 and a well-known risk factor for cardiovascular diseases, cancer, diabetes and asthma.2–4 However, among critically ill patients mostly beneficial effects of obesity have been reported,5–15 named ‘the obesity paradox’, 16 and a putative immunomodulatory mechanism has been suggested to explain these effects.17,18
Obesity leads to a chronic state of low-grade inflammation. Levels of the pro-inflammatory cytokines TNF-α, IL-6, IL-1β and the pro-inflammatory marker C-reactive protein (CRP) increase as the mass of adipose tissue increases, 19 while mass loss results in reduction of pro-inflammatory markers. 20 Interestingly, the profile of both pro- and anti-inflammatory cytokines, and adipokines in the morbidly obese are generally comparable to critically ill patients. 21 Possibly, the pre-existing pro-inflammatory state in obesity primes the immune system to mount a more pronounced immune response during systemic inflammation or sepsis. Accordingly, several animal studies have shown an increased inflammatory response during sepsis in obese animals compared to lean controls.22–24 This can partly be explained by the fact that fat tissue itself is reactive to exogenous triggering factors like LPS. It was shown that the intravenous injection of LPS in healthy adults results in expression of several adipocytokine and chemokine genes in subcutaneous fat tissue. 25 However, not only the adipose tissue itself may be responsible for the altered immune response in the obese, as blood drawn from obese women with a BMI > 40 kg/m2 produced twice the amount of TNF-α compared to patients with a BMI of 20–25 kg/m2 after in vitro stimulation with endotoxin. 26
Considering that an ever increasing number of overweight patients are admitted to intensive care unit, it is of importance to gain more insight into the potential immunomodulatory effects of adipose tissue. Existing data are derived mainly from in vitro, ex vivo and murine models of systemic inflammation, while human in vivo data are lacking. The experimental human endotoxemia model, in which a low dose of Escherichia coli endotoxin is administered intravenously to healthy volunteers, serves as a standardized way to investigate the innate response in vivo in humans. This study aims to investigate the effect of the body mass index on the pro- and anti-inflammatory cytokine production in vivo during experimental endotoxemia.
Materials and methods
Design and participants
In this study, data and plasma samples of seven double blind, randomized placebo-controlled trials were used that were performed in our institution from 2005 to 2010. All seven studies (NCT00246714, NCT00513110, NCT00783068, NCT00785018, NCT00916448, NCT01349699, NCT01091571) investigated the effect of an intervention on the innate immune response elicited by endotoxin administration using the exact same endotoxemia protocol. The samples from these studies were re-analyzed for cytokines in one batch for the current study, to prevent bias from inter-assay variability. Only the data of participants that received LPS and placebo or LPS and an intervention that did not influence the immune response were used. We only studied male volunteers because of considerable differences in the LPS-induced cytokine response between men and women, and possible effects of hormonal variations due to the menstrual cycle. 27
The study protocols were approved by the Ethics Committee of the Radboud University Nijmegen Medical Centre and complied with the Declaration of Helsinki, including current revisions and the Good Clinical Practice guidelines. All participants were screened carefully (height, mass, general physical examination, medical history, routine laboratory tests, hepatitis and HIV serology, and an electrocardiogram in the 14 d preceding LPS administration). Participants that experienced febrile illness in the 4 wks preceding the test were excluded. Only non-smoking individuals were included. The participants abstained from caffeine and alcohol for 24 h, and did not drink or eat for 12 h prior to the start of the experiment.
Procedures
On the morning of the experiment, participants were admitted to the research unit of our intensive care department. Participants received a 20-gauge arterial catheter (Angiomat; Becton Dickinson, Sandy, UT, USA) for continuous blood pressure monitoring and blood sampling. Hemodynamic data were monitored continuously for safety. A venous cannula was placed to permit infusion of 1.5 l of 2.5% Glc/0.45% NaCl in 1 h preceeding LPS infusion (prehydration), followed by 150 ml/h until 6 h after LPS infusion and 75 ml/h until the end of the experiment to ensure an optimal hydration status. At t = 0 h, the participants received 2 ng/kg U.S. Reference Escherichia coli endotoxin intravenously over 1 min, followed by 5 ml of normal saline (E. coli O:113, Clinical Center Reference Endotoxin, National Institute of Health, Bethesda, MD, USA). The same batch of endotoxin was used for all studies.
Inflammatory parameters
EDTA-anti-coagulated blood was drawn from the arterial catheter at T = 0, 60 and 90 min, and 2, 4 and 8 h after LPS administration for the measurement of pro-inflammatory cytokines TNF-α and IL-6 and the anti-inflammatory IL-10 and IL-1RA. Blood was processed immediately by centrifugation at 2000 g at 4℃ for 10 min before being stored at −80℃ until further analysis. Concentrations of TNF-α, IL-6, IL-1ra and IL-10 were determined using a simultaneous Luminex assay, according to the manufacturer’s instructions (Milliplex; Millipore, Billerica, MA, USA). As a general clinical measure of inflammation, body temperature was measured every 30 min.
Data analysis and statistics
For all cytokines, peak levels and area under curve (AUC) values were determined. These values were related to the mass, body mass index (BMI), and body surface area (BSA) of the subjects using Spearman’s correlation analyses. Also, the ratio of the AUCs of TNF-α/IL-10 as a measure of pro-anti inflammatory balance was analyzed. To increase the sensitivity to detect a possible relation between BMI and cytokine induction, participants were stratified in three groups according to their BMI (<20, 20–25, >25 kg/m2) and systemic cytokine levels were compared between the strata. For data analysis, Graphpad Prism 5.0 was used (Graphpad Software, San Diego, CA, USA). All data are expressed as mean ± SEM or median (interquartile range), depending on their distribution. A P-Value of <0.05 was considered statistically significant. According to methods described previously, 28 we calculated that with a sample size of 112 participants and an alpha of 0.05 this study had 80% power to detect a correlation between BMI and peak cytokine response with an r of 0.23 or higher.
Results
Demographic data
One hundred and twelve men, aged 22.2 ± 0.2 yr, were enrolled. Participants had an average height of 184 ± 0.7 cm and mass of 77.2 ± 0.9 kg, resulting in a mean BMI of 22.8 ± 0.2 kg/m2. BMIs ranged from 18.3 to 33.6 kg/m2, and were distributed normally (Figure 1). Thirteen participants had a BMI < 20, 83 participants had a BMI of 20–25, and 16 participants had a BMI > 25 kg/m2. Height was not statistically different between the strata (185 ± 2.3 cm, 184 ± 0.8 cm and 185 ± 1.5 cm, respectively; one-way ANOVA P = 0.63).
Distribution of BMIs of the study population.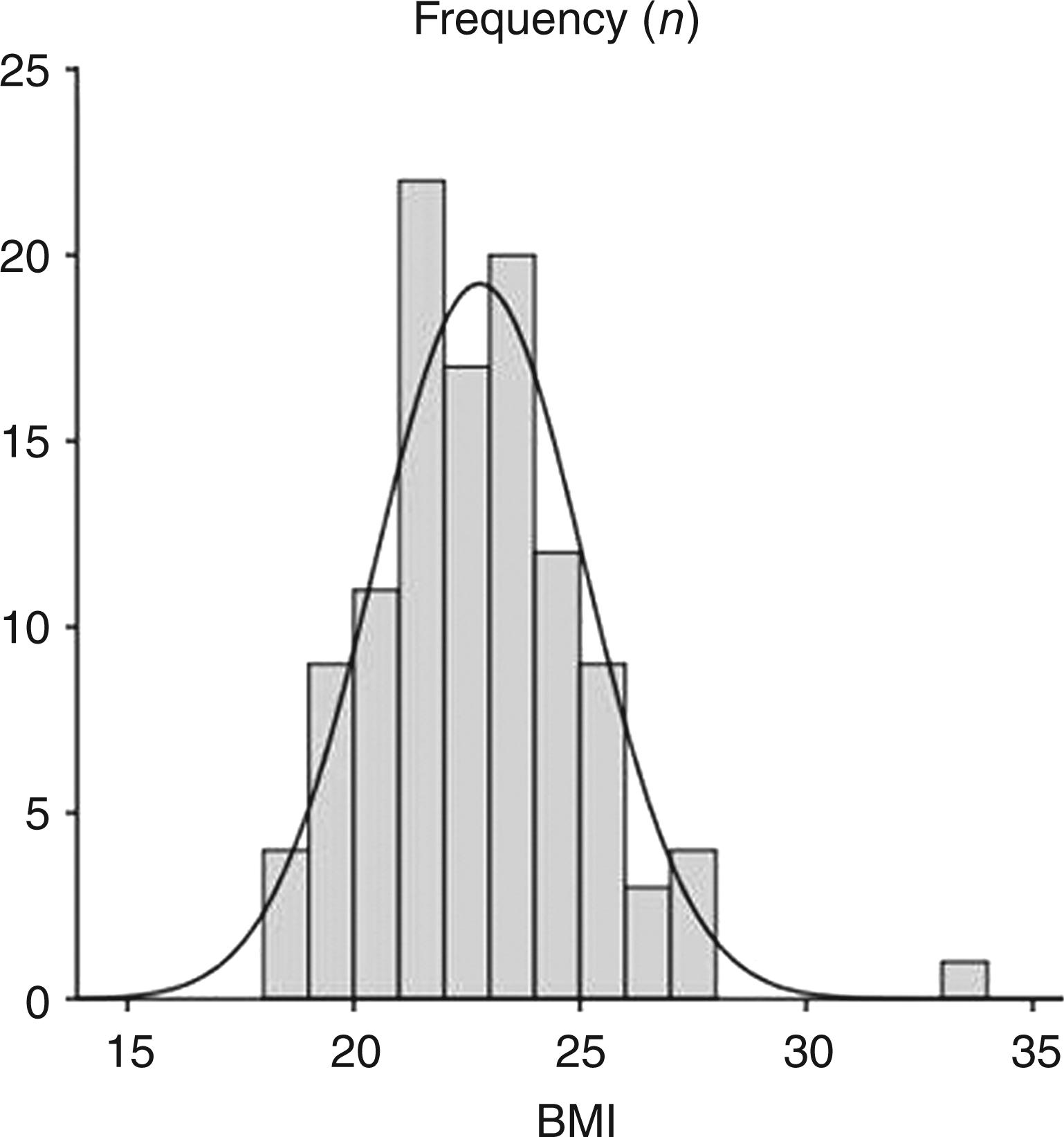
Endotoxemia symptoms
Approximately 1 h (T = 1) after the administration of LPS, participants began to show flu-like symptoms. The symptoms reached maximum severity at T = 90 min. Thereafter, symptoms declined gradually to normal values at the T = 8 h (data not shown). There was a transient increase in body temperature of 1.8 (1.4–2.2)℃ (Figure 2). There were no differences in symptom scores and body temperature between the three different BMI strata.
Body temperature, mean arterial pressure, heart rate and white blood cell count during experimental human endotoxemia. Left-hand panels: values are depicted as median with interquartile range. Right-hand panels: maximal differences compared with baseline. Data were stratified according to BMI. Boxes represent interquartile ranges, whiskers represent the 10th and 90th percentile. Differences between groups were analyzed by the Kruskal–Wallis test for nonparametric data. No significant differences were found between the three groups. MAP: mean arterial pressure; HR: heart rate; WBC: white blood cell count.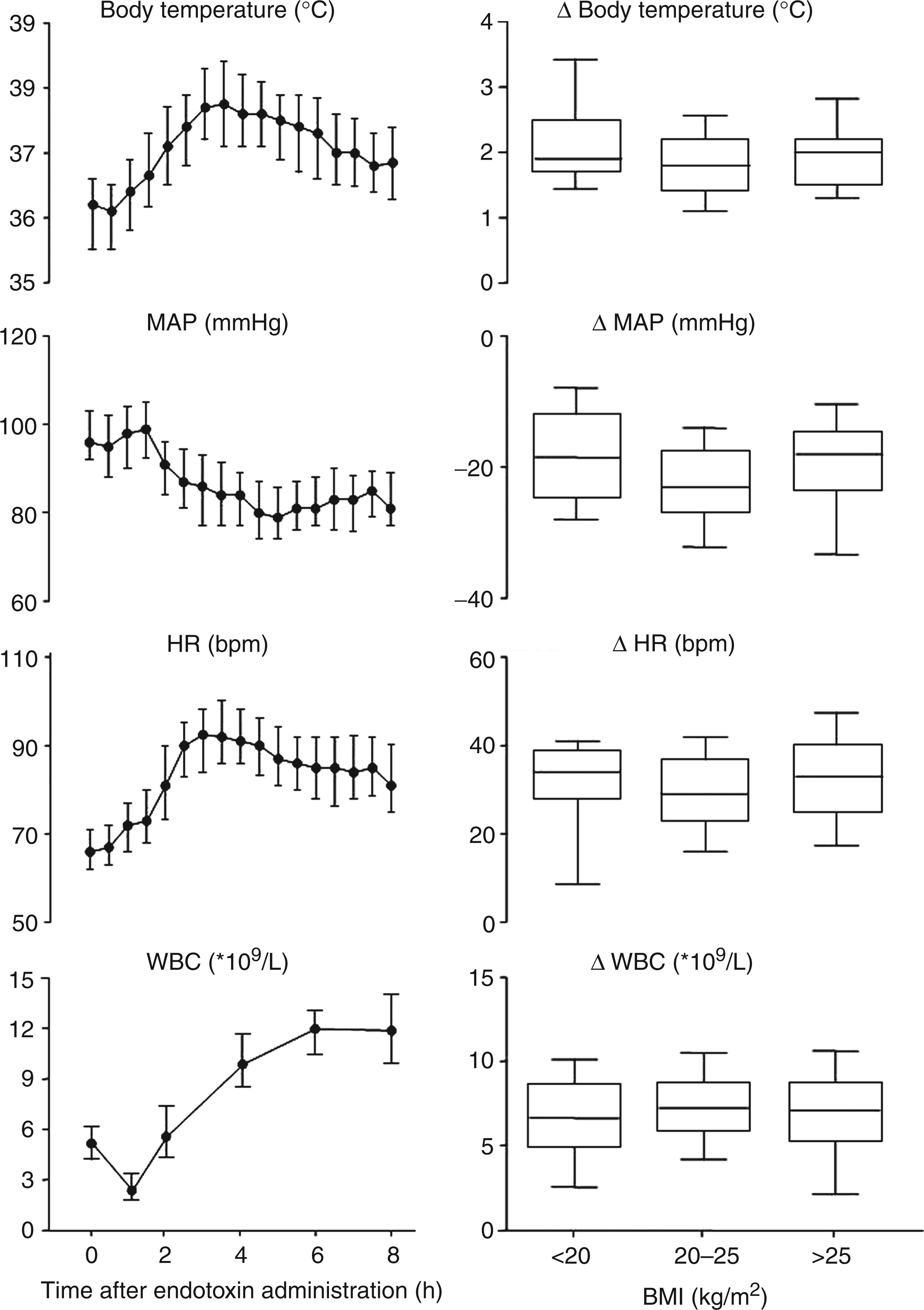
Cytokine response
Endotoxemia led to a marked cytokine response, illustrated in Figure 3. TNF-α peaked at T = 1.5, while IL-6 was maximally induced at T = 2 h. Peak levels of IL-10 and IL1ra were reached at T = 2 and T = 4, respectively [peak levels: TNF-α 509 (353–673) pg/ml, IL-6 757 (522–1098) pg/ml, IL-10 271 (159–401) pg/ml, IL-1RA 4882 (3927–6025) pg/ml)].
Plasma cytokine levels during endotoxemia. Values are depicted as median with interquartile range.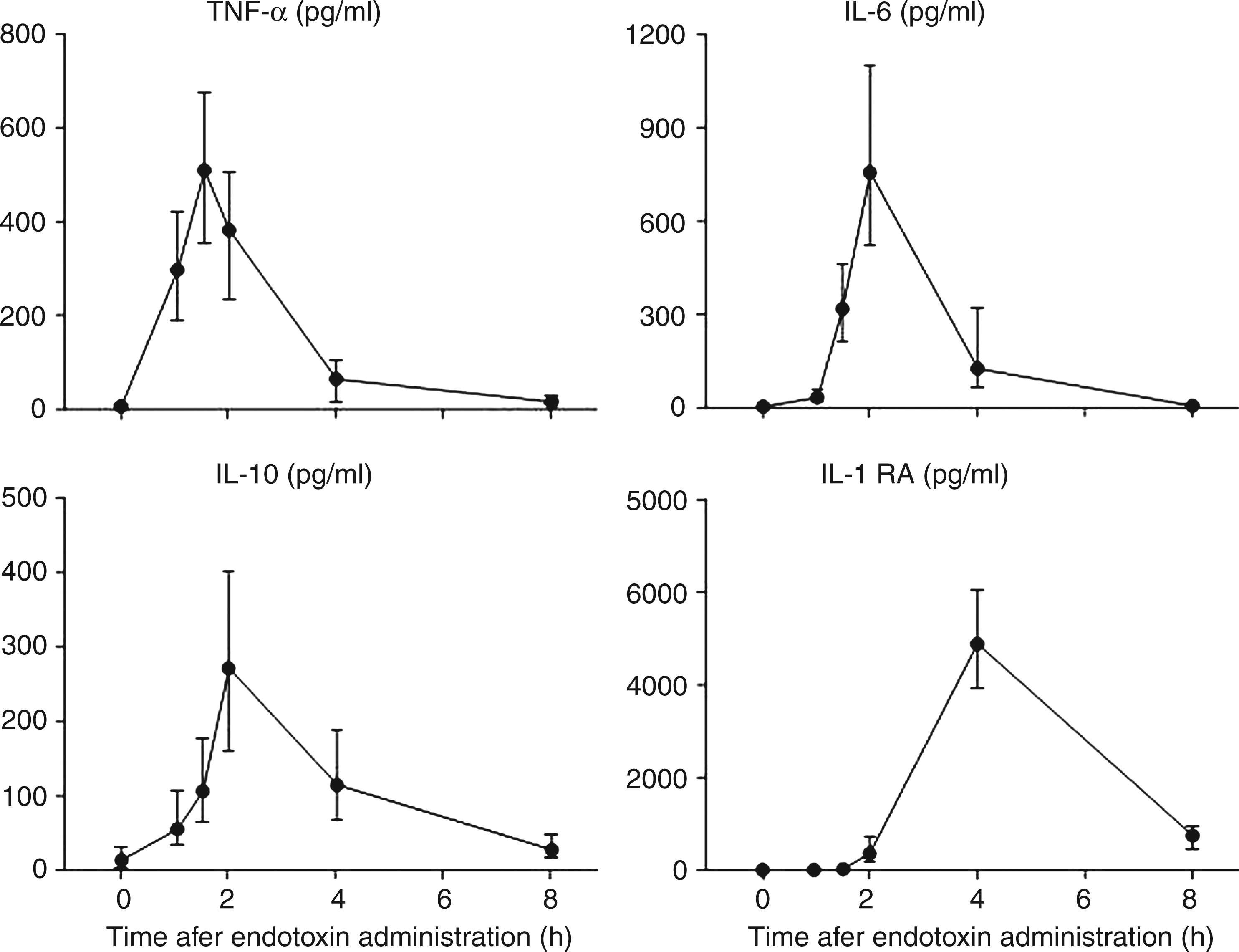
Correlation analyses
Spearman correlation analyses between indexes of body mass and cytokine levels.
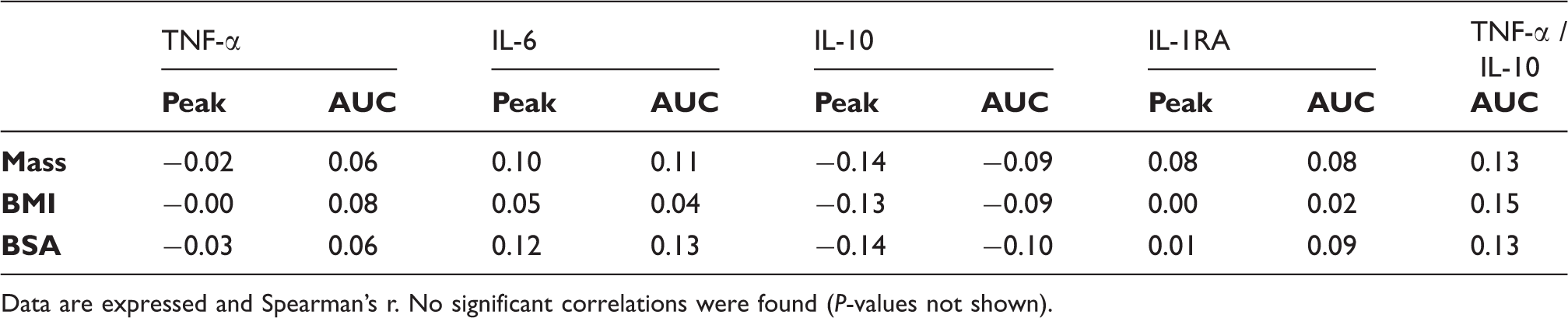
Data are expressed and Spearman’s r. No significant correlations were found (P-values not shown).
Furthermore, no significant differences were found between the three aforementioned strata, neither in cytokine peak levels (Figure 4), nor in AUCs of the different cytokines, nor in the ratio of the AUCs of TNF-α/IL-10. One participant was a statistically significant outlier for IL-10 (peak level 3502 pg/ml), and another for IL-1RA (peak level 56,399 pg/ml), but they had normal BMIs of 21.5 and 21.7 kg/m2 respectively. In addition, the participant with the highest BMI (33.6 kg/m2) had normal peak levels of TNF-α (616 pg/ml), IL-6 (1233 pg/ml), and IL-1RA (6384 pg/ml), while peak IL-10 was relatively, but not abnormally, low (126 pg/ml).
Cytokine peak levels stratified according to BMI. Boxes represent interquartile ranges; whiskers represent the 10th and 90th percentile. Differences between groups were analyzed by the Kruskal–Wallis test for nonparametric data. No significant differences were found between the three groups. AUCs of the cytokine responses stratified according BMI were not shown, but also showed no difference.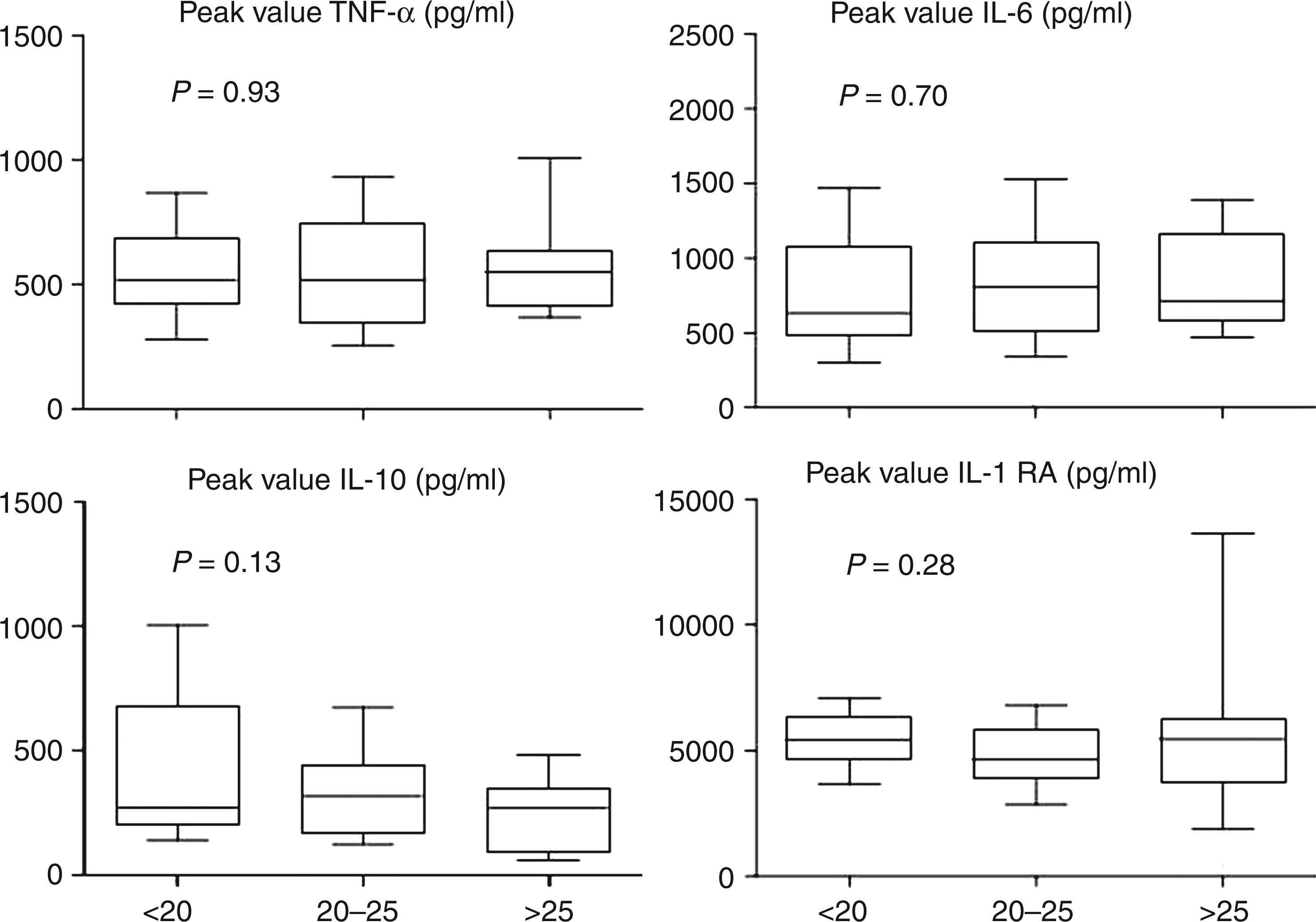
Discussion
This is the first study that investigates the relationship between BMI and the innate immune response in humans in vivo during systemic inflammation. No correlation was found between BMI and the systemic inflammatory cytokine response after the intravenous administration of endotoxin to human volunteers.
The debate on the existence of a beneficial effect of obesity in critically ill patients has been going on for decades, including several meta-analyses, of which most conclude that obese patients have equivalent or improved survival compared with patients with a BMI between 20 and 25 kg/m2.15,29,30 The findings of these studies have been subject of debate31–33 and the mechanism of action by which a higher BMI is associated with a better outcome is unclear. One of the supposed mechanisms by which obesity leads to a better prognosis is an altered immune response. In the current study we tested this hypothesis in an experimental human endotoxemia model. In contrast to data obtained from intensive care unit patients, which are difficult to interpret owing to differences in patient characteristics (age, gender, comorbidity, etc.) and differences with regard to the inflammatory stimulus (type and site of infection, time of onset, disease severity, etc.), the experimental endotoxemia model makes it feasible to test the immune response in a standardized manner in a homogenous group of participants. Our findings in humans do not correspond to the results from previous rodent studies, of which most,22,34,35 but not all, 36 report a pro-inflammatory effect of obesity. In humans, apart from more nutritional reserves, higher levels of pro-inflammatory 37 and anti-inflammatory cytokines,38,39 and the higher cholesterol and lipid levels common in obese patients that bind endotoxin during critical illness and provide the precursors for adrenal steroid synthesis 40 have been related to the beneficial effects of a higher BMI. In addition, neutrophil dysfunction and attenuation of acute lung injury, 41 and diaphragmatic remodeling due to chronically increased mass 42 and chronically increased intra-abdominal pressure 43 are possibly related to a lower acute respiratory distress syndrome incidence in obese patients. 44
While our study demonstrates the absence of a clear association between BMI and the cytokine response, we acknowledge several limitations. First, we used data of 112 healthy volunteers from 7 previously conducted endotoxemia trials. Despite this relatively large sample size, our population does not comprise a large number of overweight and obese participants, and no massively obese participants with a BMI > 35 kg/m2; therefore, any interpretation of the effects of a BMI > 30 kg/m2 is limited, especially when considering that a possible relation may not be linear, but rather be dependent on a certain BMI threshold. Nevertheless, ICU mortality has been shown to decrease gradually with increasing BMI, with beneficial effects already found in patients with a BMI of 25 to 30 kg/m2, 45 suggesting that our sample population was appropriate to detect a possible difference. Second, we only measured four key cytokines, two of which are considered archetypal pro-inflammatory cytokines, and two that are regarded as classic anti-inflammatory cytokines. All four cytokines are induced relatively early in the inflammatory response. Late cytokines, like, for example, IFN-γ, HMGB-1, IL-8 and IL-17, were not measured. Therefore, we cannot rule out the possibility that a correlation exists between BMI and one of the unmeasured mediators; however, as early pro-inflammatory cytokines orchestrate the subsequent immune response, the panel of markers we chose is representative of the general inflammatory cytokine response induced by endotoxin administration. In accordance, no BMI-dependent effects on inflammatory symptoms and fever were observed. Finally, BMI is only an indirect measure of obesity, as it assumes that overweight is attributed to excess body fat, while, in fact, well-trained muscular participants with low levels of body fat may actually have higher BMIs. Previous studies have shown that, after adjustment for BMI, waist circumference and waist-to-hip ratio were associated strongly with the risk of death for non-hospitalized patients, 46 whereas a higher mortality rate was observed for adults with a thigh circumference <60 cm. 47 Unfortunately, more direct measures of body fat percentage, such as skin fold measurements or bioimpedance determinations, were not available as the primary aim of the individual trials in which these volunteers participated was not to investigate the effect of body fat on innate immunity.
In conclusion, we have studied the effect of BMI on the systemic cytokine response induced by endotoxin administration in a large group of healthy young men, and found no relation between BMI and the cytokine response. Our data suggest that the better prognosis of obese patients during critical illness is unlikely to be mediated through an altered cytokine response.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.