
Abstract
We conducted a systematic review of the definition of a scaphoid fracture on MRI scans, examining 58 studies of patients with suspected scaphoid fractures. Nearly half the studies did not report any definition or measurement of fracture. Among those that did, 29 out of 33 studies (88%) described a linear fracture shape, 13 out of 33 studies (39%) reported the extent of the fracture across the scaphoid and none specified the fracture line orientation. Of the 25 studies describing fractures using at least one of the shape and extent groupings, 12 (48%) regarded a linear signal through the cortex as a fracture, five (20%) regarded a linear intramedullary signal in isolation as a fracture and eight (32%) regarded a diffuse intramedullary signal in isolation as a fracture. This review highlights the need for a consensus definition of scaphoid fractures on MRI scans to assess the reliability and diagnostic performance of MRI scans for diagnosing true scaphoid fractures, as well as their potential harms and benefits.
Introduction
In patients with scaphoid tenderness after a fall, normal radiographs do not exclude a scaphoid fracture. The concern is that an undiagnosed non-displaced fracture, when missed, has the potential to displace or not heal if not adequately immobilized (Fowler and Hughes, 2015; Inoue and Sakuma, 1996; Mallee et al., 2015; Steinmann and Adams, 2006). It is not possible to reduce the probability of a fracture to zero and attempts to do so can introduce potential harm from over-testing and over-treatment (Ring et al., 2023; Sterling et al., 2022).
Various strategies for diagnosis of true scaphoid fractures are used in research and clinical practice including repeat radiograph after a week or two, ultrasound and the use of CT or MRI scans. However, there is no consensus reference standard to assess the diagnostic performance characteristics of these imaging strategies. Some researchers have adopted alternative statistical techniques such as latent class analysis, in which groupings of various factors associated with probabilities of a true fracture are considered in the absence of a reference standard (Buijze et al., 2011; Duckworth et al., 2011).
The use of MRI scans for diagnosing true scaphoid fractures have been reported by some to be both highly sensitive and specific (94 and 98% respectively), using a reference standard of 2–6 weeks post-injury radiographs (Bäcker et al., 2020). However, since MRI detects any change in water content, misinterpretations of bone bruises and other variations as fractures may be common. In one study, anatomical variations in MRI signal abnormalities among healthy individuals were misinterpreted as scaphoid fractures (De Zwart et al., 2012). Given the low prevalence of true fractures among suspected scaphoid fractures in many settings, even tests with good diagnostic performance characteristics can provide misleading information, including false positives. As we know from Bayes’ theorem, even highly sensitive and specific tests can be misleading when the likelihood of true fracture is low (Ring and Lozano-Calderón, 2008). Effective use of MRI to refine fracture probability would benefit from an unambiguous and consistent definition and measurement of fracture.
We systematically reviewed the specific criteria used to define scaphoid fracture on MRI in studies of patients with suspected scaphoid fractures to date and to assess the consistency and variability of these definitions.
Methods
The following databases were searched from inception to 6 November 2020: MEDLine/OVID, Cochrane library, Web of Science, Scopus and CINAHL (Online Tables S1–S5). All quantitative clinical studies that evaluated the use of MRI to diagnose true scaphoid fractures among suspected fractures were included. There were no restrictions on year of publication or language. The exclusion criteria were studies on cadaveric bones, non-union, stress fractures, patients younger than 13 years and those using contrast-enhanced MRI. We included studies of patients 13 years and older since the chondral ossification of the scaphoid is generally completed around this time, making the anatomy similar to that of adults (D’Arienzo, 2002). After reviewing the full text, we also excluded studies that were not specific for scaphoid fractures or studies that did not provide an MRI definition of fracture. Published studies were identified using MeSh terms such as ‘scaphoid fracture’, ‘scaphoid bone’, ‘wrist injuries’, ‘navicular fracture’, ‘magnetic resonance imaging’ and ‘MRI’ (Online Tables S1–S5).
Two reviewers (blinded for review) independently screened the title and abstract of studies to meet the inclusion criteria. Disagreements were discussed to reach consensus. Then the two reviewers independently assessed the full text reports for eligibility and independently noted the reasons for exclusion. Again, disagreements were discussed to reach consensus. In all stages, if consensus could not be reached by discussion, a senior author, JD (blinded for review), was involved. All included studies were screened using forward and backward citation to find additional eligible studies.
The methodological quality was independently assessed by two reviewers using the Quality Assessment of Diagnostic Accuracy Studies-2 (QUADAS-2) for diagnostic accuracy studies (Whiting et al., 2011); the Mixed Methods Appraisal Tool (MMAT) for quantitative studies, case reports and mixed method studies (Hong et al., 2018; Pace et al., 2012); and the Joanna Briggs Institute (JBI) checklist for cost-effectiveness studies (Gomersall et al., 2015). This review is reported in accordance with the ‘Preferred Reporting Items on Systematic Reviews and Meta-Analysis’ 2020 guidelines.
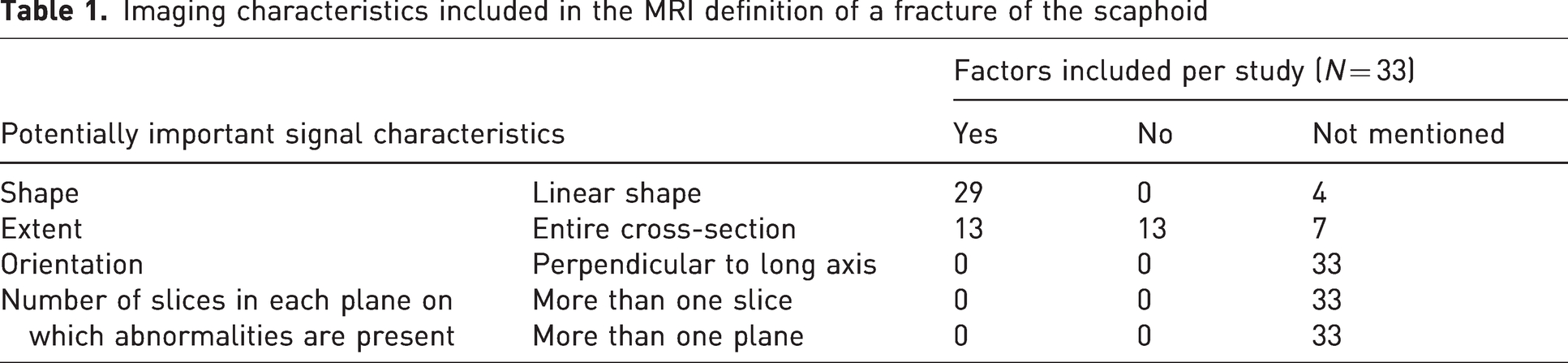
The following data were extracted independently in duplicate: study characteristics (including aims, inclusion/exclusion criteria, and participant characteristics); MRI timing; and the MRI definition of a scaphoid fracture. The factors used by other investigators and ourselves to diagnose fractures on MRI scans were recorded: (1) shape of signal (linear or diffuse); (2) extent of cross-section involved (complete or partial); (3) orientation of signal (ideally roughly perpendicular to long axis); and (4) number of slices and planes on which the abnormalities should be present (>1 slices and >1 planes) (Table 1). We then identified how often these fracture characteristics were used in the definition. We also identified grouping of shape and extent criteria including a linear signal abnormality through the cortex (‘cortical fracture’), a linear intramedullary signal abnormality (‘trabecular fracture’) and a diffuse intramedullary signal abnormality (bone marrow oedema).
Imaging characteristics included in the MRI definition of a fracture of the scaphoid
Statistical analysis
Listed fracture characteristics on MRI were analysed using descriptive statistical methods and presented as frequencies.
Results
The search rendered 2554 records. After screening titles and abstract, 2340 studies were excluded. The remaining 214 full texts were then assessed for eligibility. We excluded 156 full-text studies. Forty four studies did not use MRI to diagnose fractures or used contrast-enhanced MRI, 32 did not address acute fractures or were not specific to scaphoid fractures, 19 involved a population younger than 13 years, five were non-clinical studies, 11 studies used coded diagnoses rather than imaging interpretations, 10 had unsuitable study designs (international meeting abstracts, seminars and protocols of unpublished research) and 35 were duplicates. Fifty-eight studies were included (Figure 1). Forward and backward citation yielded another four studies. Of the 62 included studies, 29 (47%) did not report a definition for scaphoid fracture on MRI. The remaining 33 studies reported a definition and were included for critical appraisal and data extraction (Figure 1, Online Table S6). Five study groups authored more than one study. Two of these groups produced three (Annamalai and Raby, 2003; Brydie and Raby, 2003; Raby, 2001) and two (Buijze et al., 2011; Mallee et al., 2011) studies, respectively, and used consistent diagnostic criteria throughout these studies. The other three, representing two, three and four studies each, were not consistent in their use of diagnostic criteria (Appendix S1) (Bergh et al., 2014; 2015; Breitenseher et al., 1997a; 1997b; Clementson et al., 2015; 2016; 2017; Memarsadeghi et al., 2006; Schick et al., 1999).
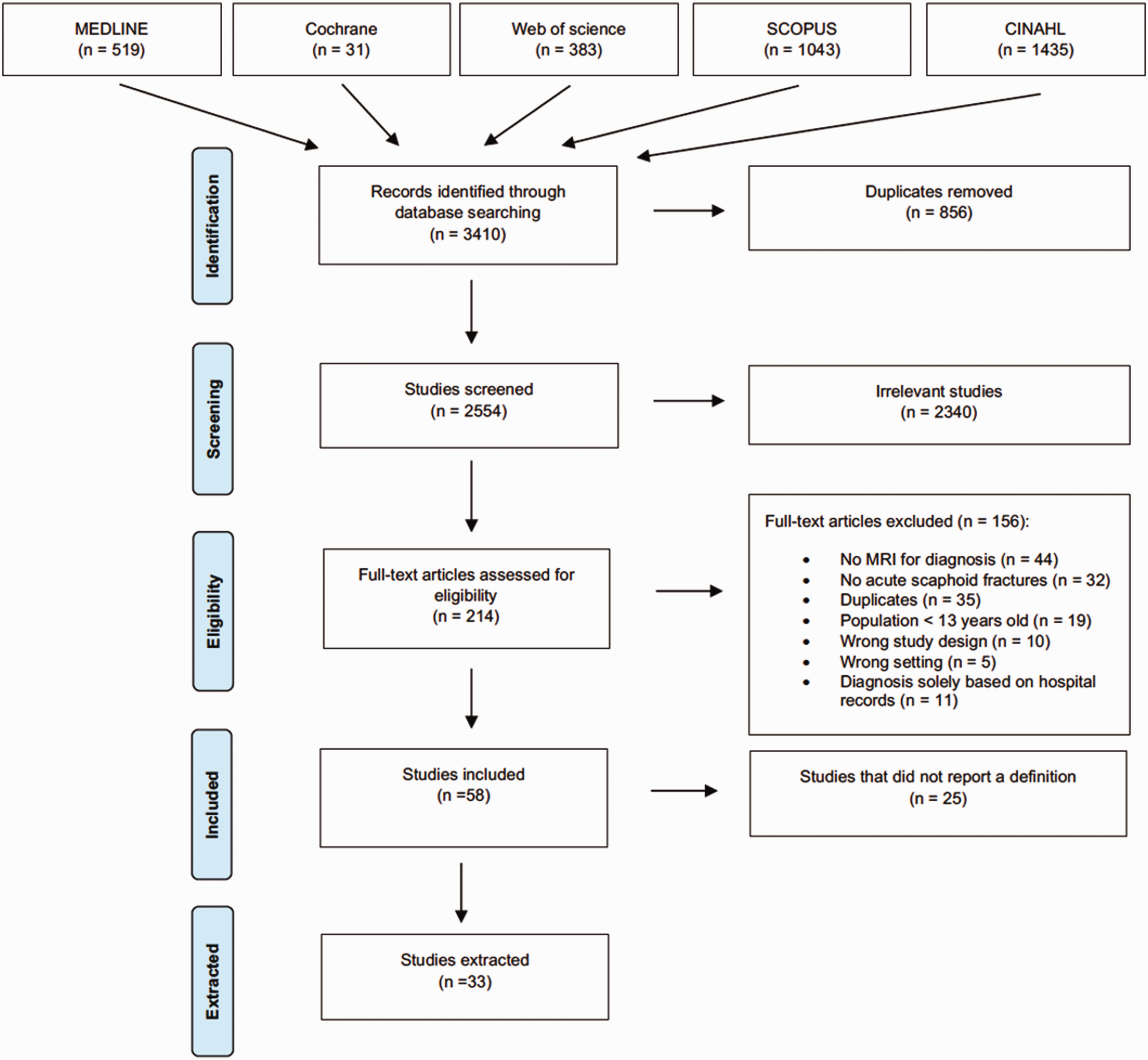
PRISMA flow diagram illustrating study selection process.
Critical appraisal and study characteristics
Sixteen publications were appraised using the QUADAS-2 tool (Annamalai and Raby, 2003; Bergh et al., 2015; Borel et al., 2017; Breitenseher et al., 1997a; 1997b; Bretlau et al., 1999; Buijze et al., 2011; Edlund et al., 2016; Fowler et al., 1998; Herneth et al., 2001; Ilica et al., 2011; Jorgsholm et al., 2013; Kumar et al., 2005; Mallee et al., 2011; Memarsadeghi et al., 2006; Schick et al., 1999). Twelve studies were appraised with MMAT (Brydie and Raby, 2003; Clementson et al., 2015; Clementson et al., 2016; 2017; Glad et al., 2010; Hunter et al., 1997; Kelson et al., 2016; Moller et al., 2004; Moreno Ramos et al., 2013; Raby, 2001; Senevirathna et al., 2013; Thavarajah et al., 2011). Five were appraised using the JBI checklist for economic evaluations (Bergh et al., 2015; Brooks et al., 2005; Dorsay et al., 2001; Gooding et al., 2004; Patel et al., 2013) (Online Tables S7–S9). The studies included an average of 90 participants (range 12–532), 61% men, with a mean age of 29 years (range 14–86 years). Three studies did not report a time frame (Dorsay et al., 2001; Glad et al., 2010; Hunter et al., 1997) and the others performed MRI scan within 6 weeks of injury. The majority (58%) of MRI scans were performed within seven days after injury.
Imaging characteristics used to diagnose fracture on MRI
Linear shape was a criterion for diagnosis of fracture in 29 of 33 studies (88%) and was not mentioned in four studies (Appendix S2; Online Tables S10 and S11). The extent of signal change across the scaphoid was a criterion in 26 studies and was not mentioned in seven studies (Appendix S2; Online Tables S10 and S11). In studies considering the extent of signal change across the scaphoid, the signal needed to cross the entire bone in 13 studies (39%) and only part of the bone in a further 13 studies (39%) (Appendix S2; Online Tables S10 and S11). No studies mentioned whether these signal changes needed to be oriented perpendicular to the long axis of the scaphoid or present on multiple slices or in multiple planes (Table 1, Figure 2).
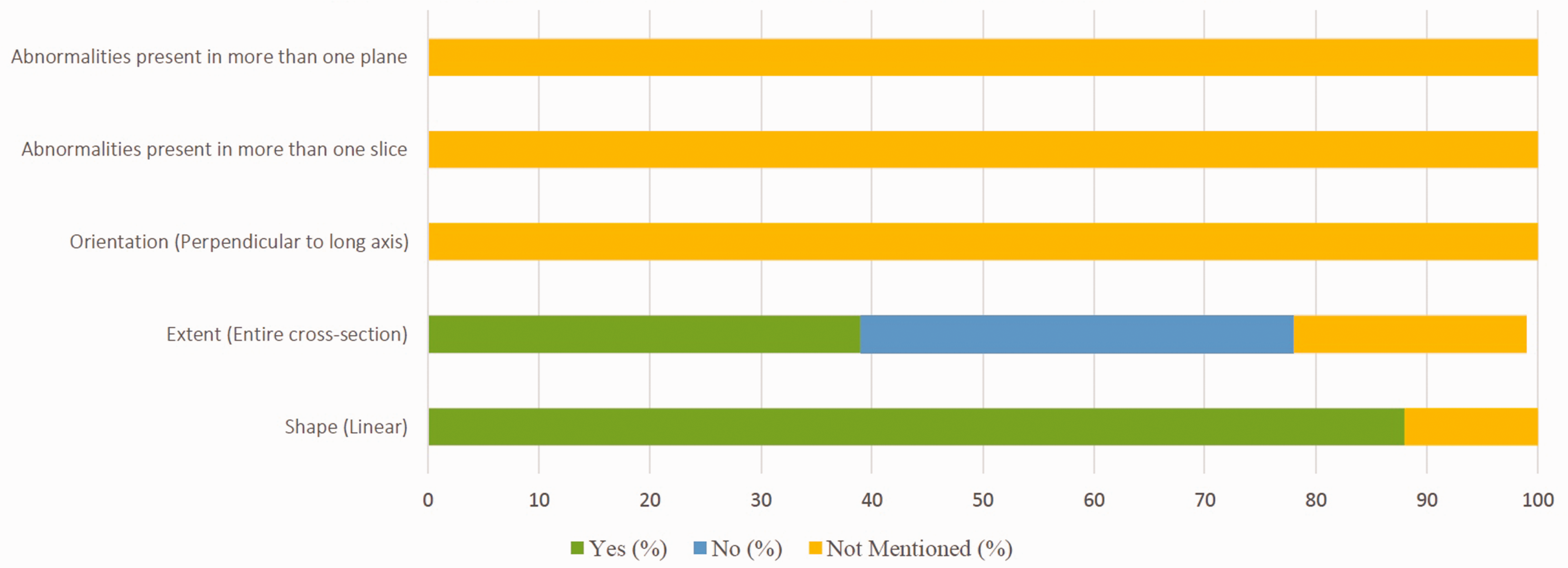
Imaging characteristics included in MRI definition of scaphoid fracture.
Twenty-five of 33 studies (76%) described a fracture using at least one grouping of shape and extent criteria (Table 2). A linear signal through the cortex (cortical fracture) alone was considered a fracture in 12 studies, only in combination with an intramedullary linear signal (trabecular fracture) in four studies, only in combination with a diffuse intramedullary signal (bone marrow oedema) in three studies and was not mentioned in 15 studies (Appendix S2; Online Tables S10 and S11). A linear intramedullary signal (trabecular fracture) in isolation was considered a fracture in 11 studies, only in combination with a diffuse intramedullary signal (bone marrow oedema) in two studies, was not considered fracture in four studies and was not mentioned at all in 15 studies (Appendix S2; Online Tables S10 and S11). A diffuse intramedullary signal (bone marrow oedema) alone was regarded as a fracture in eight studies, only in combination with other factors in four studies, was not considered a fracture in 10 studies and was not mentioned in 11 studies (Appendix S2; Online Tables S10 and S11).
Summary of the criteria used to define a scaphoid fracture in 33 studies
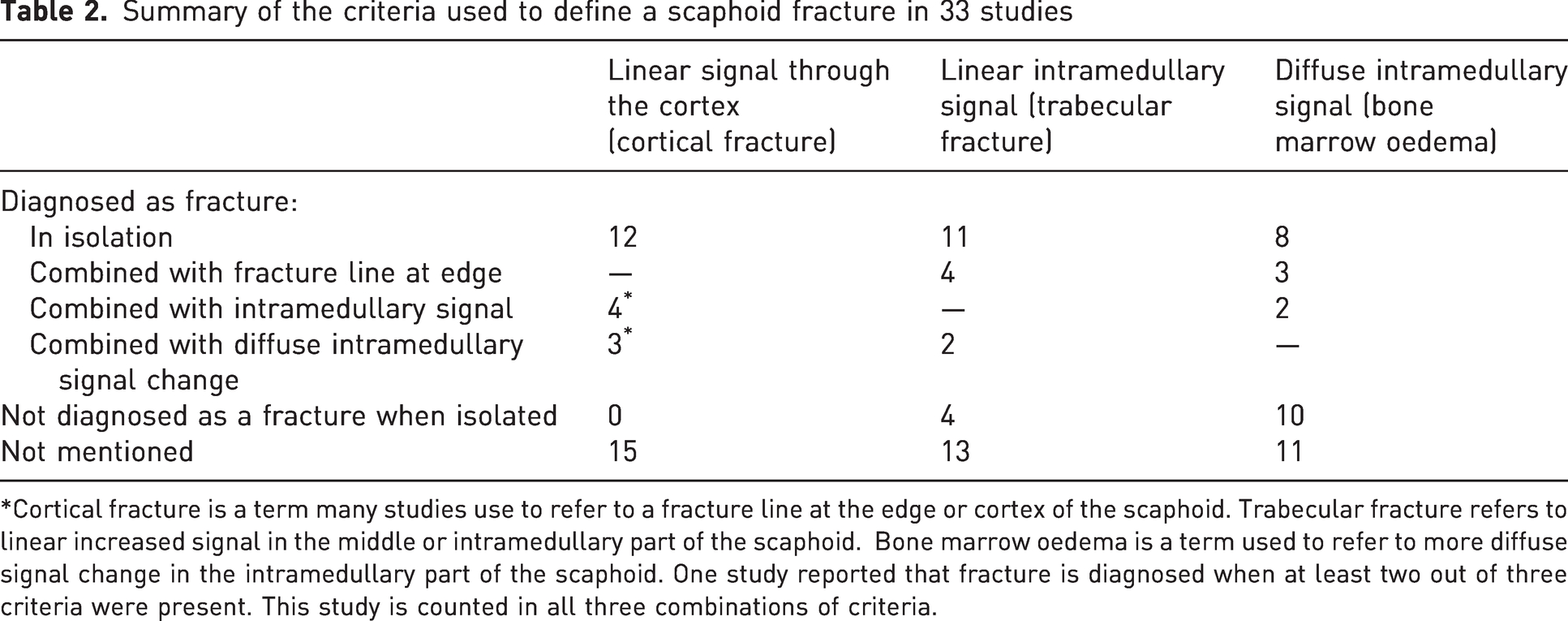
*Cortical fracture is a term many studies use to refer to a fracture line at the edge or cortex of the scaphoid. Trabecular fracture refers to linear increased signal in the middle or intramedullary part of the scaphoid. Bone marrow oedema is a term used to refer to more diffuse signal change in the intramedullary part of the scaphoid. One study reported that fracture is diagnosed when at least two out of three criteria were present. This study is counted in all three combinations of criteria.
Discussion
True scaphoid fractures remain difficult to diagnose in patients with suspected scaphoid fractures. It is estimated that approximately one out of six scaphoid fractures is overlooked on initial radiographs, and additional imaging is often used to exclude a fracture (Hunter et al., 1997; Mallee et al., 2015). MRI is recommended as a secondary imaging method to diagnose true fractures among suspected fractures (Annamalai and Raby, 2003; Bergh et al., 2014; Borel et al., 2017; Edlund et al., 2016; Herneth et al., 2001; Ilica et al., 2011; Jorgsholm et al., 2013). In this systematic review we established that almost half (47%) of the studies that address the use of MRI to diagnose scaphoid fractures did not report a definition or measurements. Among the 33 studies that did present definitions and measures of fracture, these tend to be inconsistent and contradictory sometimes even among the same group of researchers.
The main weakness of this study was the need to interpret reported definitions, which were often limited and sometimes cryptic. To counter this, we devised a checklist of morphological features to consider. While others might derive different results from a repeat of our review, we are confident that some level of variation and contradiction among fracture definitions would remain. Second, some authors and research groups contributed to more than one of the included studies. It is therefore notable that there were sometimes inconsistencies even within author groups.
The observation that definitions and measures of scaphoid fractures on MRI are often omitted or inconsistent in published research points to the need for a consensus definition to ensure consistent reporting, optimal reliability and accuracy. A potential future consensus is that most studies (88%) considered linear signal change to be part of the fracture definition.
As an example of the problems that can arise in the absence of a consensus reference standard for MRI signal changes representing a fracture, the sensitivity of cone beam CT (CBCT) in detecting carpal fractures using MRI as a reference standard was 100% using ‘cortical fracture’ as the standard and 89% when intramedullary oedema (‘trabecular fracture’) was considered a fracture (Borel et al., 2017). Furthermore, when five musculoskeletal radiologists interpreted blinded MRI scans of healthy individuals and patients evaluated for suspected scaphoid fracture they diagnosed 13 scaphoid fractures, 36 bone bruises and 23 other fractures among the healthy volunteers (De Zwart et al., 2012). Signal changes in bone marrow oedema on MRI are common in the absence of trauma or fracture and can be misinterpreted (Alam et al., 1999).
The observation that fracture orientation and number of slices and planes were not used by any study to help define and measure scaphoid waist fracture on MRI seems like a missed opportunity. This omission may reflect both practical and methodological factors, including variability in MRI protocols across institutions, limited reporting standards, or lack of consensus on the clinical relevance of specific imaging characteristics. Our view is that authors and investigators may tend to be advocates and promoters of a diagnostic technique, which can lead to enthusiasm for any signal detected on MRI rather than cautious, critical appraisal of its diagnostic performance. This tendency may increase the risk for overdiagnosis and over-treatment. This review highlights the need for greater rigour and caution in the interpretation of MR imaging for suspected scaphoid fractures. We suggest that the four criteria used in this study (shape, extent, orientation and number of slices/planes) be further developed into a diagnostic strategy that can be tested for reliability and accuracy, keeping in mind that tests for accuracy will need to use latent class analysis or similar techniques as there is no consensus reference standard for a true fracture (Duckworth et al., 2011). Ambiguous and potentially misleading terms such as ‘trabecular fracture’ should be avoided.
Supplemental Material
sj-pdf-1-jhs-10.1177_17531934251367541 - Supplemental material for Variation in definitions of scaphoid fracture on MRI scans for suspected fracture: a systematic review
Supplemental material, sj-pdf-1-jhs-10.1177_17531934251367541 for Variation in definitions of scaphoid fracture on MRI scans for suspected fracture: a systematic review by Marouska F. van Boxel, Ali Kaplan, David Ring, Emily H. Jaarsma, Job N. Doornberg and Miryam C. Obdeijn in Journal of Hand Surgery (European Volume)
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.