
Abstract
This retrospective study compared the diagnostic accuracy of conventional radiography (CR) and computed tomography (CT) in classifying Kienböck’s disease (KD) according to Lichtman staging. Besides age, cartilage condition and vascularity, bone morphology is important in choosing the most appropriate treatment in KD. In 278 patients, two musculoskeletal radiologists performed a consensus reading of 281 lunate necroses according to the Lichtman classification, based on CR and CT. Stage IIIc was most common in CR (43%) and CT (61%), followed by stage IIIa for CR (25%) and stage IV for CT (15%). In 67%, KD was classified as the same in both modalities. The KD stage had to be upgraded in CT in 34% of cases, notably with stage IIIa progressing to IIIc in 24 out of 69 patients and stage IIIb to IIIc in 23 out of 38 cases. Overall, the Lichtman score was significantly higher on CT. The findings suggest that CT is better than CR in accurately determining the stage of KD stage, indicating a potential shift towards more surgical salvage procedures.
Introduction
Kienböck’s disease (KD) is characterized by osteonecrosis, fragmentation and collapse of the lunate, followed by carpal instability and osteoarthritis. The lunate consists of osseous, vascular and cartilaginous components, for each of which a separate classification has been developed: osseous, Lichtman (Lichtman and Degnan, 1993; Lichtman et al., 2010), vascular, Schmitt (Schmitt et al., 1997) and cartilage, Bain (Bain and Begg, 2006).
Lichtman et al. (2022) recently developed a unified classification and treatment algorithm combining the three existing classifications. Besides age, cartilage condition and vascularity, bone morphology is particularly important for choosing the most appropriate treatment in KD. In particular, the surgical treatment decision from stage III and IV is determined by the bony morphology of the lunate: apart from unloading procedures, revascularizing, local or carpal reconstructive methods or salvage procedures are used.
Assessment of the internal osseous structure and integrity of the lunate is often not possible by conventional radiography (CR) owing to superimposition of other information in the image. High-resolution computed tomography (CT) has been shown to be more accurate in the assessment of the osseous microstructure of the lunate in KD (Friedman et al., 1991; Schmitt et al., 1997).
The aim of the study was to compare the Lichtman osseous staging (Lichtman and Degnan, 1993; Lichtman et al., 2010) of KD by CR and CT.
Methods
Study design and patient selection
The study was approved by the institutional review board (ethics proposal number 21-0567). Informed consent was not required, in keeping with the policies for a retrospective study. Patients with KD treated at the Department of Hand Surgery at the Rhön-Clinic, Campus Bad Neustadt, between January 2010 and February 2021, were selected from the database for further analysis (n = 337). Eligible patients had to have undergone examination both by CT and CR within a 3-month timeframe. A total of 278 patients met this inclusion criterion.
CT imaging
CT scans of the wrist were performed either on a 64-row scanner (Optima) or a 256-row scanner (Revolution), both from GE Medical Systems (Milwaukee, WI, USA), using the following settings for both scanners: collimation 0.625 mm; pixel spacing 0.793 mm; pitch factor 0.516; tube voltage 120 kV; image matrix 512 × 512; and modulated tube current 100–220 mA. For the acquisition of transaxial CT images, the patients were standing beside the CT gantry with the forearm pronated and the hand placed flat and in a longitudinal direction on the gantry table. Images were reconstructed in the transaxial, sagittal and coronal planes using a bone-specific convolution kernel (slice thickness 0.625 mm, increment 70% and high-resolution bone kernel).
Conventional radiography
Plain radiographs were obtained in true posteroanterior and true lateral views using advanced flat panel detector technology (DR 400; Agfa-Gevaert N.V., Mortsel, Belgium). Attention was paid to ensure that the true posteroanterior view was obtained in a true neutral position, with 90° of shoulder abduction and 90° of elbow joint flexion, as the position of the distal ulna in relation to the distal radial surface changes longitudinally with varying degrees of forearm rotation (Epner et al., 1982; Palmer et al., 1982).
Image analysis
CR and CT images were analysed in random order by two radiologists (NH and RS, both specialized in musculoskeletal radiology with 11 and 35 years of experience, respectively) in a consensus reading using a picture archiving and communication system (PACS; Visage Client Version 7.1.18, Visage Imaging GmbH, Berlin, Germany). CR and CT readings were conducted 4 weeks apart. Readers were unaware of any clinical information and results from MRI.
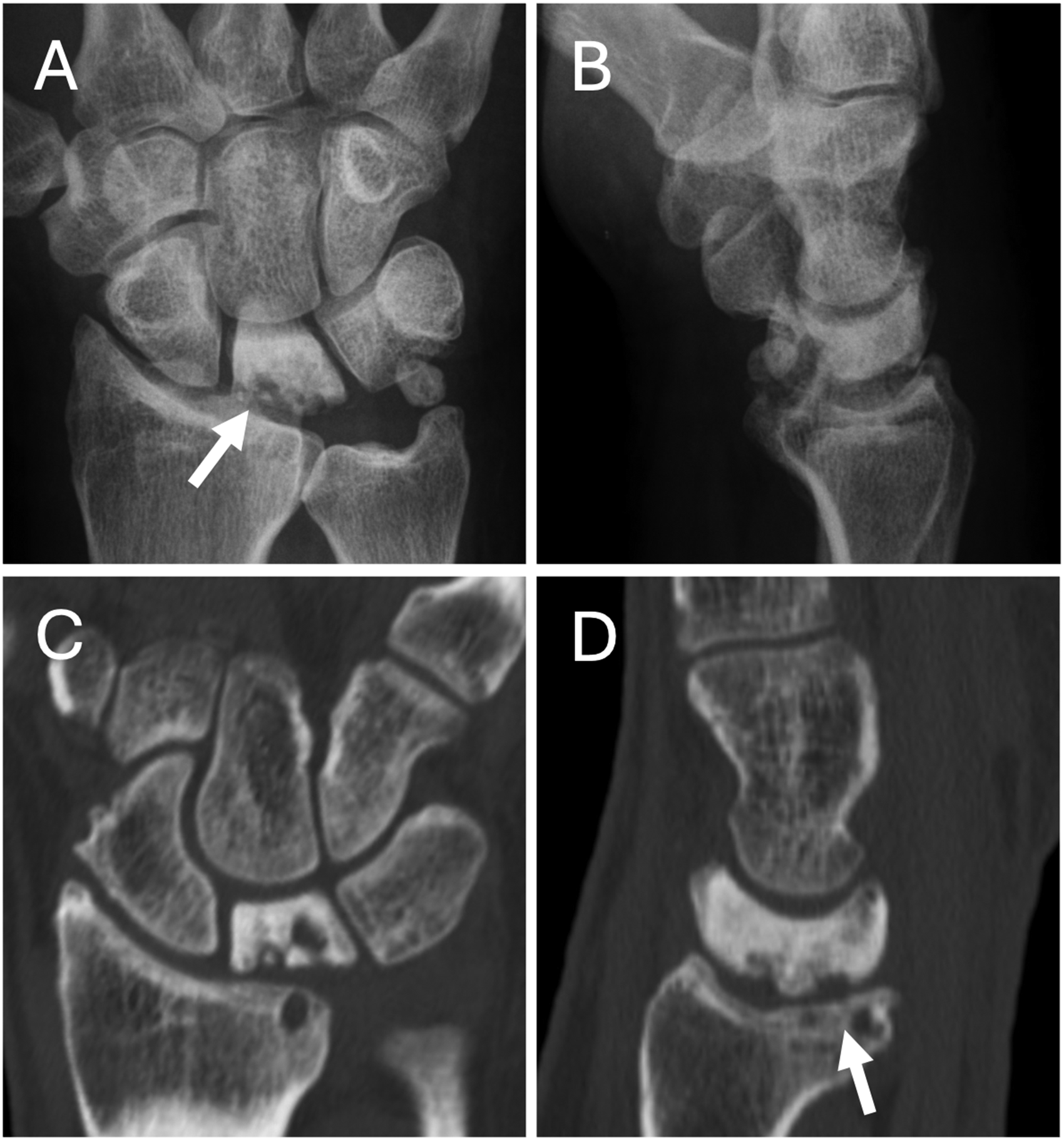
CR and CT images were graded into stages I, II, IIIa, IIIb, IIIc and IV according to the Lichtman classification (Lichtman and Degnan, 1993; Lichtman et al., 2010). Examples for upgrading stage IIIa on CR to stage IIIc on CT are shown in Figures 1 and 2. Figure 3 provides an example of an upgrade from stage IIIa on CR to stage IV on CT.
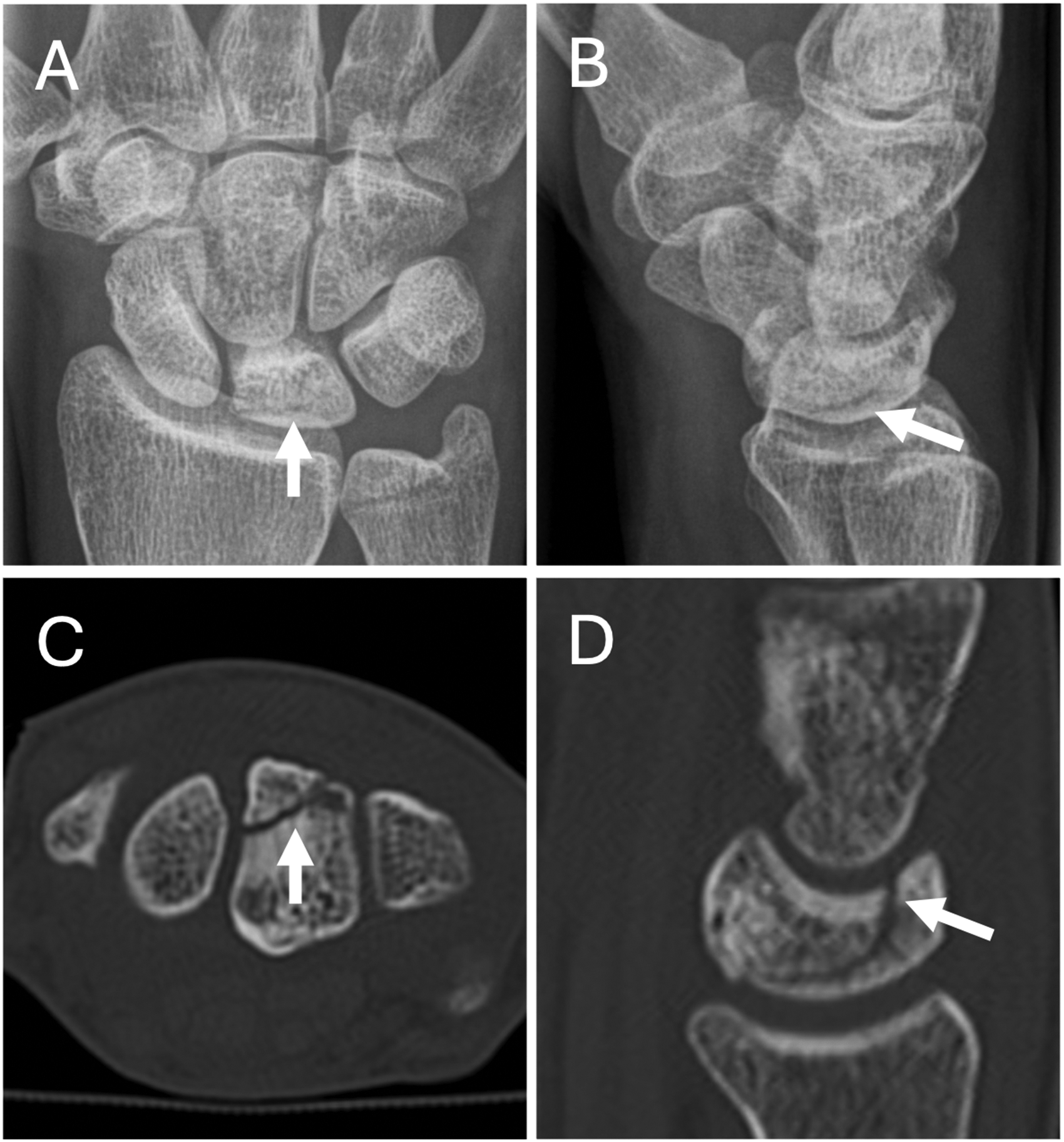
A 34-year-old woman with Lichtman stage IIIa on CR and stage IIIc on CT. In the (a) posteroanterior and (b) lateral views, CR shows only a horizontal fracture line in the lunate (arrows). In the (c) transaxial and (d) sagittal CT images, the fracture line (arrows) extends to the distal pole of the lunate, which was not visible on CR. CR: conventional radiography; CT, computed tomography.

A 24-year-old woman with Lichtman stage IIIa on CR and stage IIIc on CT. CR in the (a) posteroanterior and (b) lateral views show a proximal impaction fracture of the lunate (arrows). In the (c) transaxial and (d) sagittal CT images, the coronal fracture of the lunate is clearly visible. Note the osteonecrosis (osteosclerosis) of the posterior aspect of the lunate in panel d. CR: conventional radiography; CT, computed tomography.
A 48-year-old man with Lichtman stage IIIa on CR and stage IV on CT. CR in the (a) posteroanterior and (b) lateral views. Multiplanar CT reconstruction in the (c) coronal and (d) sagittal plane. Note the osseous destruction of the proximal aspect of the lunate in the radiographs (arrow in panel a) and osteosclerosis of the lunate. The osteoarthritis in the lunate fossa of the radius with subchondral cysts is clearly depicted on the CT images (arrow in panel d). There is an incidental finding of a calcified lesion in the ulnar recess in panels a and b. CR: conventional radiography; CT, computed tomography.
Statistical analysis
Data analysis was performed using RStudio Build 421, Version ‘Mountain Hydrangea’ (R Foundation for Statistical Computing, Vienna, Austria).
Descriptive statistics were used to characterize the data. For statistical analysis, Lichtman stages were recoded into scores of 1–6. Normally distributed metric variables are expressed as mean (standard deviation [SD]). Non-normally distributed metric variables are reported as median (interquartile range [IQR]) of the first quartile to the third quartile). For comparison of Lichtman classification between CR and CT, the Wilcoxon signed-rank test was used. Cohen’s Kappa was determined to assess the agreement of Lichtman classification between the imaging modalities. A generalized estimating equation model was used to determine which factors influence the increase in grading to stage IIIc on CT from CR (dependent variable: stage IIIc in CT imaging; independent variables: modality, age, sex, time interval between CT and CR). The α level was at 0.05.
Results
A total of 278 patients (168 male patients; median age 36 years [IQR 26–47]; age range 13–68 years) with KD (right lunate 173; left lunate 108) were included in the study. In three patients, both wrists were affected. The median time interval between plain radiography and CT was 6 days (IQR 0–24; range 0–86).
Table 1 lists the number of cases and frequencies of Lichtman stages of KD for CR and CT. The most common stage in both CR and CT was stage IIIc.
Comparison of stages of Kienböck’s disease (according to Lichtman et al., 2010) in CR and CT (n = 281 [left 108, right 173]).
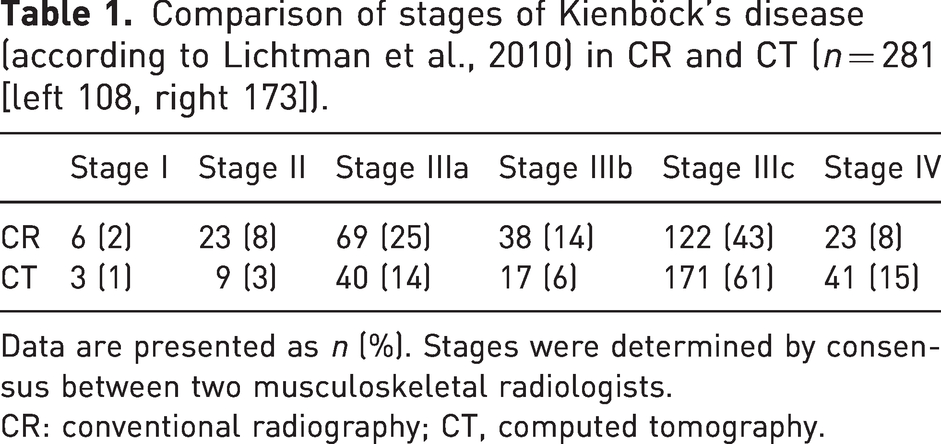
Data are presented as n (%). Stages were determined by consensus between two musculoskeletal radiologists.
CR: conventional radiography; CT, computed tomography.
Overall, the Lichtman grade was significantly higher on CT than on CR. On CT, the mean Lichtman score was 4.66 (SD 1.06) (stage IIIc); on CR, it was 4.12 (SD 1.23) (stage IIIb) (p < 0.001).
The changes of the CR stages after the CT assessment are listed in Table 2. In 67% of cases, the KD stage was classed as the same by both CR and CT imaging. Lichtman stage was increased on CT imaging in 34% of cases. In 17% of cases, the stage was increased by one grade and in 11% of cases by two grades. KD stage II, IIIa and IIIb were upgraded to stage IIIc after CT assessment in 11 out of 23, 24 out of 69 and 23 out of 38 cases, respectively. KD stage IIIb and IIIc were upgraded to stage IV on CT assessment in 6 out of 38 and 11 out of 122 cases, respectively.
Number of stages in which CT staging was rated higher (positive) or lower (negative) compared to CR staging (according to Lichtman et al., 2010).
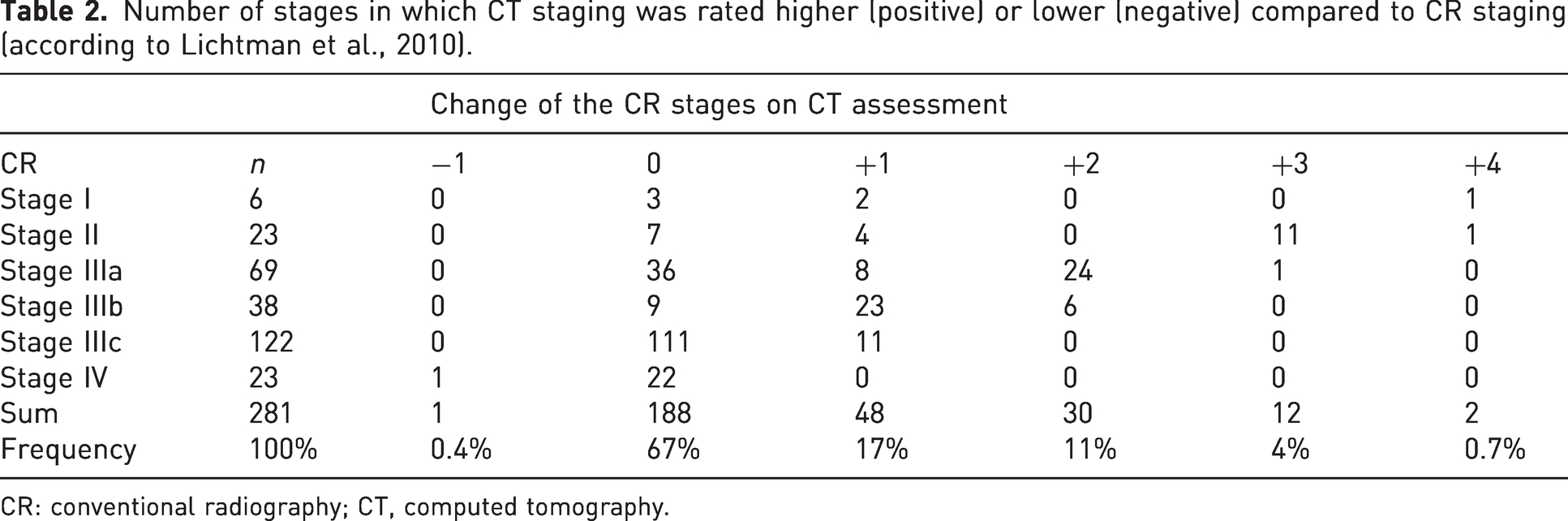
CR: conventional radiography; CT, computed tomography.
After adjusting for age, sex and time difference between CT and CR in the generalized estimating equation model, there was a 2.03-fold increased likelihood for classifying the Lichtman stage as IIIc using CT compared to CR (p < 0.001).
Owing to the frequent upgrading of the Lichtman stages in CT imaging, there was only a moderate correlation between the CT and CR classifications (κ = 0.51, 95% CI: 0.44 to 0.59).
Discussion
In summary, the study found that KD stage was graded significantly higher by CT imaging compared to CR. Stage IIIc KD was by far the most common in both CT and CR imaging. In CT imaging, the Lichtman stage was increased in 34% of cases. KD stages II, IIIa and IIIb were frequently upgraded to stage IIIc on CT assessment. In the generalized estimating equation model, there was a significantly likelihood for classifying Lichtman stage IIIc on CT compared to CR and this was independent of age, sex, affected hand side and the time interval between CT and CR imaging. Stage IV KD was detected more often by CT imaging.
In agreement with previous studies, CT imaging was better than radiographs in depicting the osseous microstructure of the lunate including osteosclerosis, subchondral impaction fractures, coronal fractures and osteoarthritis of the perilunate joints (Friedman et al., 1991; Schmitt et al., 1997). Owing to thin slices (slice thickness 0.625 mm) and the increased in-plane matrix (1024 × 1024), CT imaging offers isotropic voxels and the possibility of multiplanar reconstruction. Plain radiography often fails to detect a coronal lunate fracture owing to the superimposition of osseous structures.
Our data showed that Lichtman stages II to IIIb were frequently increased to stage IIIc on CT, with stage IIIc detected more than twice as often on CT than on CR. This can significantly alter treatment decisions, particularly in stage III. Stage IIIa might be treated with joint levelling procedures (Hegazy et al., 2021; Watanabe et al., 2008) or reconstruction of the affected proximal aspect by a vascularized medial femoral trochlea graft (Burger et al., 2013; Higgins and Burger, 2014). In stage IIIb, the radial column of the wrist is stabilized with scaphocapitate (Moy and Peimer, 1993) or scaphotrapeziotrapezoidal fusion (Stephens et al., 2022) to correct the flexion malposition of the scaphoid, or alternatively by proximal row carpectomy (PRC) (Hohendorff et al., 2012). In stage IIIc, the fractured lunate with intact vascularity can be treated with screw compression (Chou et al., 2019), whereas the fractured lunate with compromised vascularity (Schmitt C grade) cannot be reconstructed and requires salvage procedures such as PRC (Chim and Moran, 2012; Lichtman et al., 2016).
Traditional radiographic indices (radioscaphoid angle, carpal height ratio, Stahl index) have been shown to poorly detect carpal collapse to allow stages IIIa and IIIb to be differentiated (Luitjens et al., 2023). Our study confirms these findings with 12% of stage IIIa cases on CR imaging being upgraded to stage IIIb on CT imaging. Sagittal and coronal multiplanar reconstructions are best suited for assessing the proximal aspect of the lunate and the presence of carpal instability (rotatory subluxation of the scaphoid and dorsal intercalated segment instability) (Schmitt and Kalb, 2016).
Nevertheless, CR has a place in diagnosing and staging KD and for follow-up imaging after conservative or surgical treatment (White et al., 2016). In stage IV, further imaging is not necessary as only conservative treatment or salvage procedures are used in treatment (Lichtman et al., 2016). Ulnar variance can be easily assessed in the standardized radiographic dorsopalmar view (Palmer et al., 1982). Although recent studies have found no evidence for causation between ulnar variance and KD (Stahl et al., 2013), ulnar positive variance predisposes for ulnar impaction syndromes (Imaeda et al., 1996). Radiographs are valuable and cost-effective for ruling out other carpal entities such as rheumatoid arthritis, intraosseous ganglia and ulnar impaction syndromes (Watanabe et al., 2010).
Although CT imaging is best for visualizing the osseous changes of the lunate and the perilunar joints, only contrast-enhanced MRI can assess bone marrow (and bone) viability (Cerezal et al., 2000; Schmitt et al., 1997; Schmitt and Kalb, 2010). It is therefore used in KD stages I to IIIb and for ruling out other diagnoses (ulnar impaction syndromes, intraosseous ganglia, erosions etc.) and to aid further treatment planning (Schmitt et al., 2005).
The present study has some limitations. First, we did not correlate the Lichtman stages of KD with the treatment selected and did not take changes in treatment into account. Second, because of the large number of patients, we decided to assess radiographs and CT images in a consensus reading by two experts in the field of hand imaging.
In conclusion, CT imaging is significantly more accurate than CR in determining the exact stage of KD. In more than one-third of the cases, the disease stage was upgraded in CT imaging, most commonly to stage IIIc, indicating a potential shift in treatment towards salvage procedures.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Ethical approval for this study was obtained from the local ethics committee of (approval no. 21-0567). Trial registration: DRKS0002490.
Informed consent
The requirement for informed consent was waived due to the retrospective nature of the study.