
Abstract
Correctly identifying carpal collapse is important for adequate treatment of Kienböck’s disease. This study aimed to assess the accuracy of traditional radiographic indices in detecting carpal collapse to differentiate between Lichtman stages IIIa and IIIb. In 301 patients, carpal height ratio, revised carpal height ratio, Ståhl index and radioscaphoid angle were measured on plain radiographs by two blinded observers. As a reference standard, Lichtman stages were determined by an expert radiologist using CT and MR imaging. The interobserver agreement was excellent. In the differentiation between Lichtman stages IIIa and IIIb, measurements of indices showed moderate to good sensitivity (0.60–0.95) and low specificity (0.09–0.69) using normal cut-off values from the literature, while receiver operating curve analysis revealed poor area under the curve (58–66%). Traditional radiographic indices showed poor diagnostic performance in detecting carpal collapse in Kienböck’s disease and did not reach sufficient accuracy in the differentiation between Lichtman stages IIIa and IIIb.
Keywords
Introduction
Differentiation of Lichtman stages IIIa (no carpal collapse), and IIIb (carpal collapse) Kienböck’s disease is important for choosing the most suitable and appropriate treatment (Goldfarb et al., 2003; Kienböck, 1911; Lichtmann et al., 2010). Patients with stages IIIa or less can be considered for surgical reconstruction techniques. In contrast, individuals with stages IIIb and IV are candidates for salvage procedures and have a worse prognosis (Mohan et al., 2020).
Various radiographic indices have been employed in clinical routine to determine the carpal height and assess carpal collapse on posteroanterior and lateral plain radiographs of the wrist. The Youm index is the most widely used method. This index, also known as the carpal height ratio (CHR), is defined as the quotient of the carpal height and the length of the third metacarpal bone (McMurtry et al., 1978; Youm et al., 1978). In case the whole of the third metacarpal bone is not included on the radiograph, the revised carpal height ratio (rCHR), also known as the Nattrass index, the Ståhl index (STI) and the radioscaphoid angle (RSA) can be used instead (Larsen et al., 1991; Nattrass et al., 1994; Ståhl, 1947).
Against this background, this study aimed to assess the accuracy of radiographic measurement methods in their ability to differentiate between Lichtman stages IIIa and IIIb.
Methods
Approval from the Institutional Review Board was obtained, and in keeping with the policies for a retrospective study design, informed consent was not required. All patients with the diagnosis of Kienböck’s disease treated at the Department of Hand Surgery at the RHÖN-Clinic Campus Bad Neustadt over a period of 11 years (January 2010 through February 2021), were selected from the database for further analysis (n = 337). A total of 301 patients met the inclusion criteria for the study.
As well as plain radiographs, all patients had a CT and MR scan. To establish a reference standard, a senior musculoskeletal specialist with more than 30 years of experience in imaging classified the Kienböck’s wrists into Lichtman stages I to IV using all available information (patient’s medical reports, X-rays, CT and MR images, surgery reports, histopathology, follow-up reports). Coronal and sagittal CT and MR images were used for the staging reference. Classification criteria on the lunate bone were (a) the shape, particularly the curvature of the proximal circumference, (b) the absolute length as well as the relative length (in relation to Gilula line I) and (c) the internal bone architecture. Stage IIIa was assumed with a decrease in height of the lunate bone of 0–2 mm, and stage IIIb with a decrease in height of more than 2 mm. Forty-seven patients with stage IIIc (coronally oriented lunate fracture) were assigned to stage IIIa if there was a longitudinal fragment displacement less than 2 mm (33 patients), and to stage IIIb in case of a displacement greater than 2 mm (14 patients). Finally, criteria for osteoarthritis (articular space width, subchondral remodelling, osteophytes) were assessed at the radiocarpal and midcarpal joints. The final patient cohort consisted of 13 patients with stage I, 48 patients with stage II, 82 patients with stage IIIa, 92 patients with stage IIIb and 66 patients with Lichtman stage IV Kienböck’s disease. Patients’ characteristics are summarized in Table 1.
Patient characteristics.
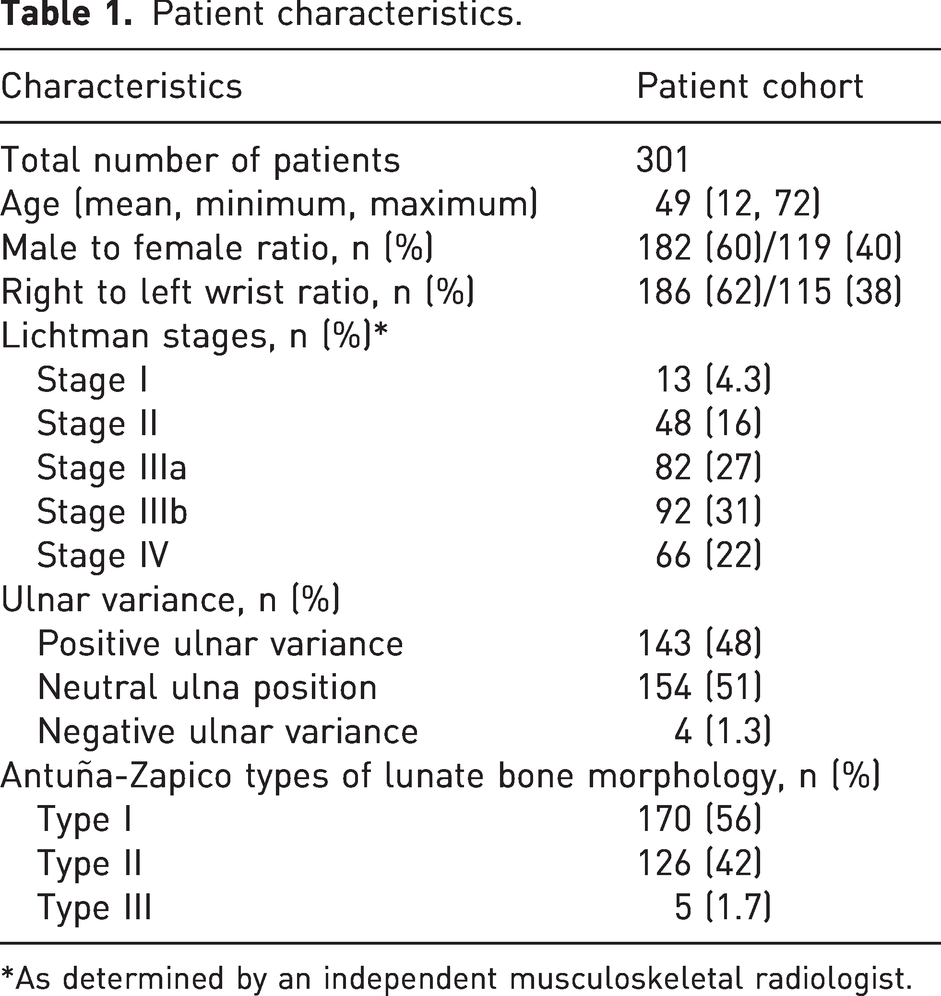
*As determined by an independent musculoskeletal radiologist.
Image acquisition and measurements
Radiographs of the wrist were acquired in a neutral position according to the standard operating procedure of the department of radiology. The posteroanterior (PA) views were taken at shoulder level with the upper arm abducted, the elbow flexed and the palm on the detector (quality criterion: the ulnar styloid process projected in profile on the ulnar side). For the lateral views, the upper arm was adducted to the trunk, the elbow was flexed and the hand was positioned on the ulnar side so that the forearm and hand were aligned colinearly (quality criterion: the pisiform bone projects between the palmar borders of the capitate bone and distal pole of the scaphoid). Patients without radiographs in the neutral position or those with limited image quality were excluded (n = 36). Two radiologists, who were blinded to both clinical data and Lichtman stages, determined the CHR (ratio of the carpal height and length of the third metacarpal), rCHR (ratio of the carpal height and length of the capitate), STI (ratio of the length and the sagittal depth of the lunate) and RSA (angle between the longitudinal axes of the radius and the scaphoid) (Figure 1).
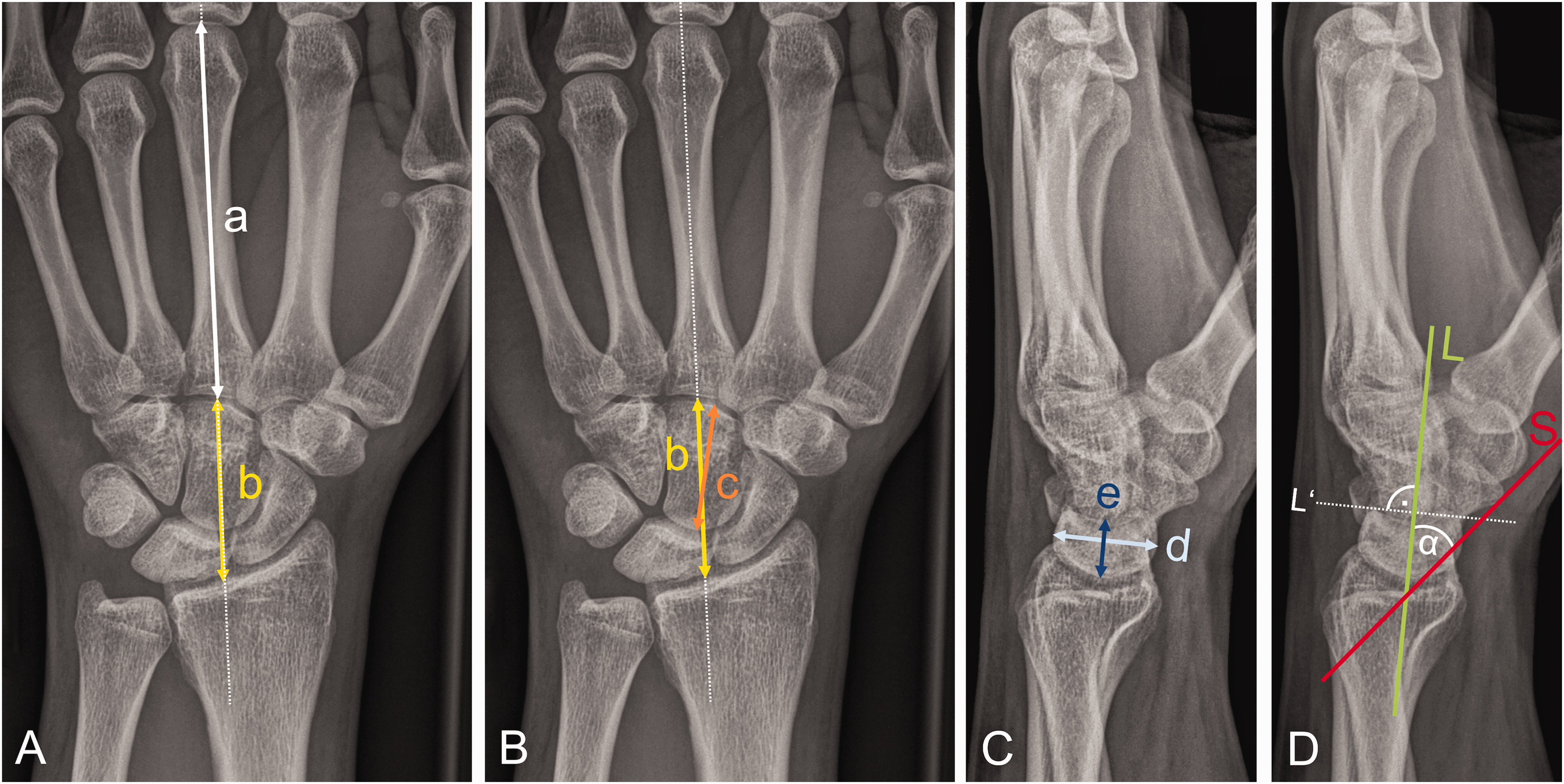
Illustration of radiographic measurement methods for the evaluation of Kienböck’s disease in a 22-year-old male with a Lichtman stage IIIa. (A) The carpal height ratio (CHR) is measured by dividing the carpal height (b) by the length of the third metacarpal (a) on a posteroanterior (PA) radiograph. (B) The revised carpal height ratio (rCHR) is measured by dividing the carpal height (b) by the length of the capitate (c) on a PA. radiograph. (C) The Ståhl index (STI) is defined by the quotient of the longitudinal (e) and sagittal (d) diameter of the lunate bone on a lateral view and (D) The radioscaphoid angle (RSA) is measured on a lateral radiograph and is defined as the angle between the longitudinal axis of the radius and the longitudinal axis of the scaphoid.
Ulnar variance according to Gelberman et al. (1975) was measured. Positive ulnar variance describes where the distal articular surface of the ulna is more than 2.5 mm distal to the articular surface of the radius, and negative variance is when the ulna is ≤2.5 mm than the radius at the distal radioulnar joint. In addition, features of the proximal articular surface of the lunate bone according to Antuña-Zapico (1966; 1993) were evaluated. Type 1 corresponds with the proximal and articular surfaces forming an angle >130°, in Type II the angle is <130° and in Type III, there are two distinct surfaces that articulate with the radius and with the triangular fibrocartilage complex.
Statistical analysis
The interobserver agreement among the two observers for measurement of CHR, rCHR, STI and RSA was evaluated using the intraclass correlation coefficient (ICC) for continuous variables and Kappa (κ) statistics for categorical variables. Receiver operating characteristic (ROC) curves were plotted to analyse the diagnostic ability of CHR, rCHR, STI and RSA in relation to the Lichtman classification. To examine whether CHR, rCHR, STI and RSA measurements differed between Lichtman stages IIIa and IIIb, Student's t-test for independent samples was applied to test for differences in means. To determine the sensitivities and specificities of the radiographic indices for the differentiation between Lichtman stages IIIa or IIIb cut-off values of the individual indices given in the corresponding literature were used (normal ranges: CHR 0.51–0.57, rCHR 1.52–1.62, STI 0.5–0.56 and RSA <60°) (Larsen et al., 1991; McMurtry et al., 1978; Nattrass et al., 1994; Ståhl, 1947; Youm et al., 1978). Therefore, the mean of each value range was used (CHR: 0.54; rCHR: 1.57; STI: 0.5; RSA: 45°) to define a reference value for physiologic wrist anatomy for the statistical analysis. A p-value of 0.05 was set as the limit of statistical significance.
Results
Ulnar variance and lunate morphology
The agreement between the observers in evaluating the ulnar variance and the lunate’s proximal articular surface morphology according to the Antuña-Zapico classification system was excellent (κ 0.99; 0.98).
Radiographic indices
Interobserver ICC between the two observers were good to excellent, for the CHR 0.98 (95% CI, 0.95–0.97), for rCHR 0.87 (0.84–0.90), for STI 0.97 (0.96–0.98) and for RSA 0.92 (0.88–0.94). Mean RSA was 60° (CI, 58.9°–60.0°) for observer 1 and 59° for observer 2 (57.9°–59.6°), respectively.
Differentiation between Lichtman stages IIIa and IIIb by using radiographic indices
When comparing STI, CHR, rCHR indices and RSA angles in Lichtman stages IIIa and IIIb, mean STI and rCHR showed pathological values both for IIIa and IIIb. Only mean RSA and CHR showed normal values in stage IIIa and pathological values in stage IIIb (Table 2). Calculated areas under the curve (AUC) were low (rCHR: 58.1; CHR: 58.5; STI: 58.5; RSA: 66.1) for the differentiation between Lichtman stage IIIa (82 patients) and IIIb (92 patients) using measurements of radiographic indices (Figure 2). Using cut-off values from previous literature, the indices showed moderate to good sensitivity (0.60–0.95) and low to insufficient specificity (0.09–0.69) (Table 3).
Radiographic indices measurements of the two blinded observers.
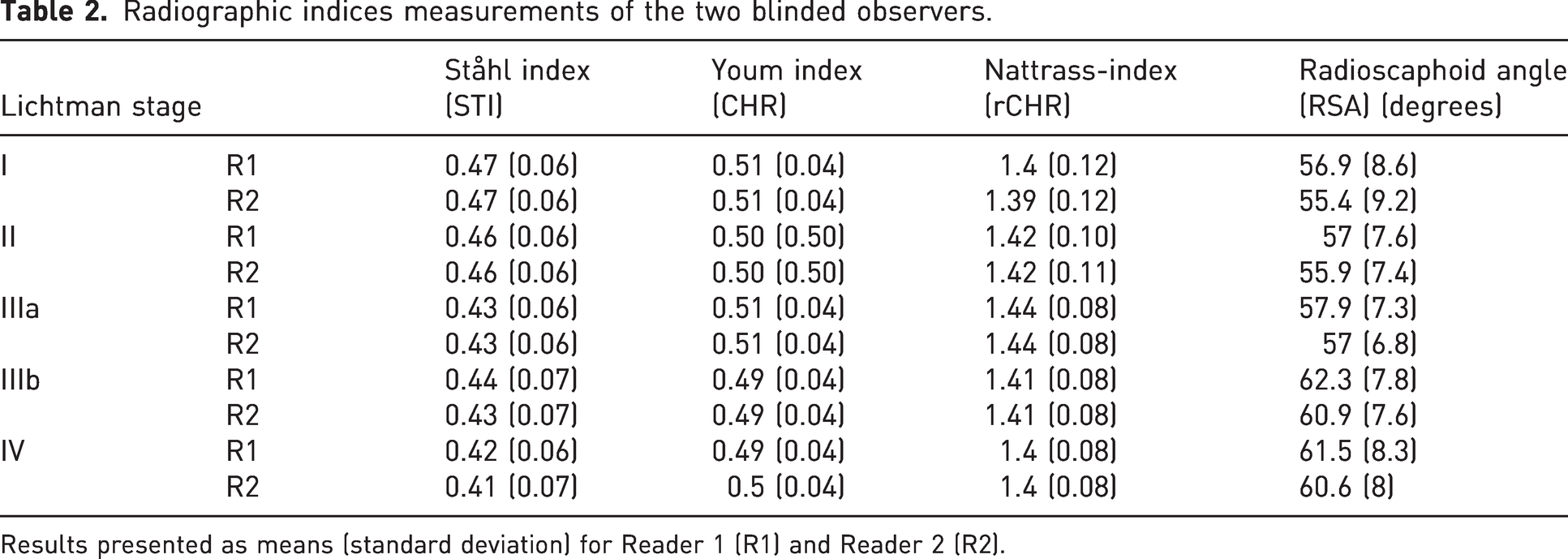
Results presented as means (standard deviation) for Reader 1 (R1) and Reader 2 (R2).
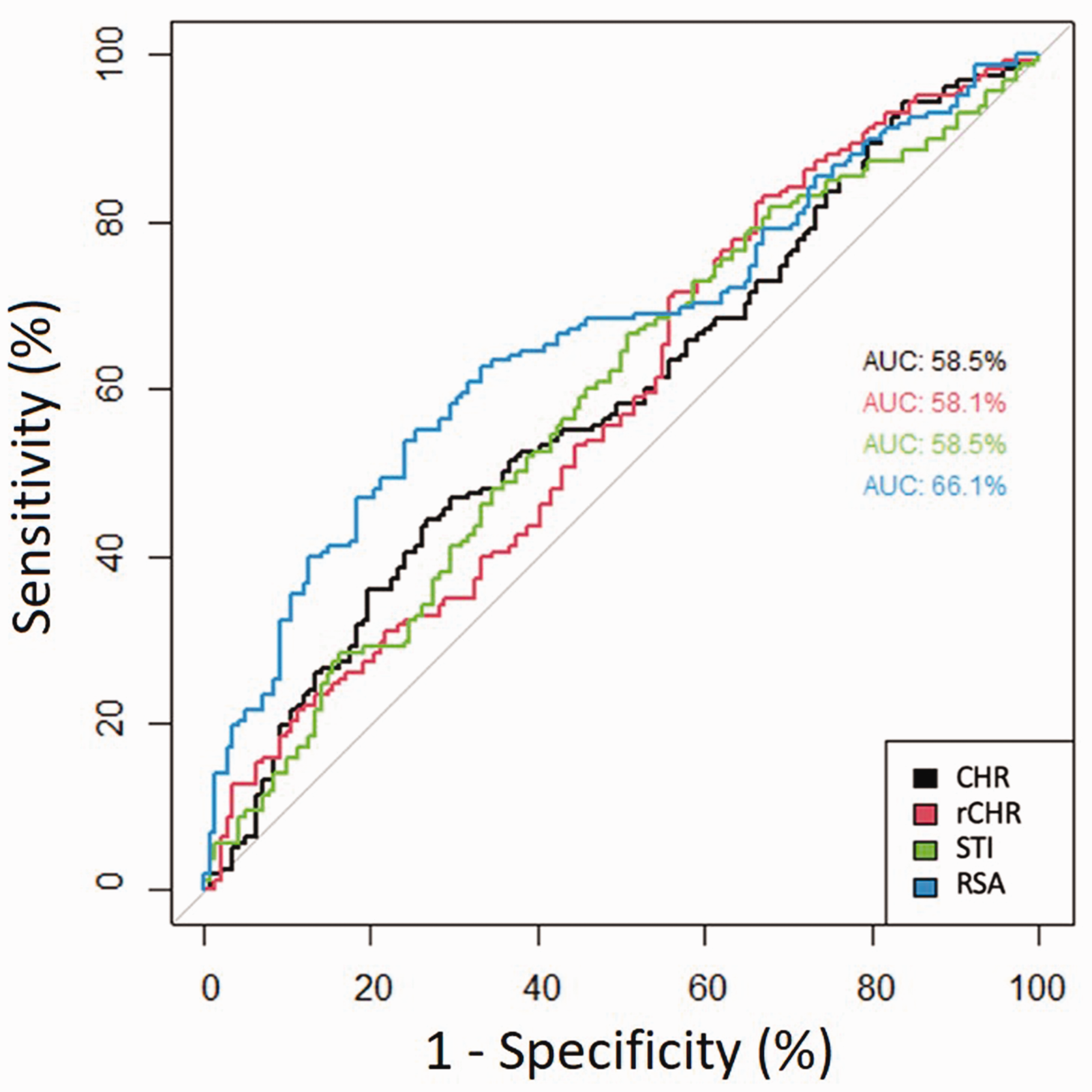
Plotted receiver operating characteristic area for the radiographic indices carpal height ratio (CHR), revised carpal height ratio (rCHR), Ståhl index (STI) and radioscaphoid angle (RSA) with associated accuracies (areas under the curve).
Diagnostic performance in determining Lichtman stages IIIa and IIIb.

PPV: positive predictive value; NPV: negative predictive value.
Discussion
The major finding of this study was that none of the traditional radiographic indices could accurately detect carpal collapse in Kienböck’s disease and differentiate between Lichtman stages IIIa and IIIb. Pathoanatomically, there are some differences between Kienböck’s disease advanced collapse and SLAC (scapholunate advanced collapse) wrist resulting from scapholunate dissociation (SLD). First, the increased flexed position of the scaphoid is not accompanied by a simultaneous dorsal shift in the radioscaphoid compartment. Instead, the proximal scaphoid pole remains centred in the scaphoid fossa of the radius, and rotatory subluxation of the scaphoid (RSS) is not present (Kawanishi et al., 2015; Taniguchi et al., 2002). Second, the centroid of the capitate also remains in a normal position and does not move dorsally in contrast to SLD (Kawanishi et al., 2015). This preserves the colinear alignment of the mid-carpal column. Third, in Kienböck's disease, the scapholunate ligament usually remains intact over a long period, making the proximal migration of the capitate less marked. Therefore, in Kienböck's, it must be assumed that carpal collapse is less pronounced compared with SLD and progresses continuously throughout the course of the disease without any definable thresholds.
For some radiographic indices, a large range of normal values have been published in the literature, indicating potential limitations in their discriminatory power. For example, the normal value range for the rCHR (Nattrass index) is from 1.52–1.62 (Nattrass et al., 1994), or that of the RSA is defined from 30°–60° (Larsen et al., 1991). In rheumatoid wrists, Borisch et al. (2004) showed that the Bouman index (height of the capitate divided by the carpal height) had higher applicability and sensitivity for a carpal collapse than the CHR, wherefore they recommended using the Bouman index, especially in rheumatoid arthritis patients (Bouman et al., 1994). Mohan et al. (2020) measured the CHR and ulnar variance on radiographs and compared it with the width/height (W/H) ratio of the lunate as measured on CT scans in 50 patients with Kienböck’s disease. The authors concluded that the lunate W/H ratio measured on CT, while significantly correlating with CHR, is a better measure of the lunate collapse. Furthermore, they found a significant correlation between the CHR on radiographs, and the W/H ratio on CT scans in delineating advanced collapse (Mohan et al., 2020). Thus, the primary objective of previous studies was to establish specific cut-off values of radiographic indices. For example, an RSA > 60° was set by Yajima et al. (1998) to indicate loss of carpal height due to scaphoid flexion in Lichtman stages IIIb and IV (Yajima et al., 1998). Another previous study of Goldfarb et al. (2003) on wrist radiographs from 39 patients with Kienböck’s disease showed that the use of the RSA increased the interobserver reliability of the Lichtman classification and allowed a better understanding of the distinction between a stage IIIa and IIIb disease. This is in contrast with the findings of our study, which indicate that accurate detection of mild carpal collapse was not reliable on the basis of measuring RSA.
Our study has some potential limitations. One limitation lies in the retrospective study design. Furthermore, we did not focus on clinical outcome parameters. Another potential limitation is that we did not have a healthy control group. Finally, the categorization of stage IIIc could also be troublesome. However, these potential limitations should not have influenced our results as those were not directly related to the major aim of our study.
We conclude that traditional indices measured on plain radiographs have poor diagnostic performance in the detection of carpal collapse in Kienböck’s disease in our patient cohort. CT or MR imaging is recommended as the presence or absence of carpal collapse is important for surgical decision-making.
Footnotes
Acknowledgements
Johanna Luitjens and Sophia Samira Goller contributed equally and share the first authorship. J Ricke, Chair of Department of Radiology, University Hospital, LMU Munich, Germany, contributed to the study.
Declaration of conflicting interests
The authors declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
All procedures were performed following the ethical standards of the Institutional Review Board and the Helsinki declaration or comparable ethical standards. Approval from the Institutional Review Board was obtained (No. 21-0567).
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.