
Abstract
Congenital hand and upper limb differences may be detected during antenatal ultrasonography or visually at birth. We investigated the experience of parents when they first learned that their child had an upper limb difference. This national retrospective cross-sectional quantitative and qualitative survey within the UK and Ireland received 261 responses from parents of children. Differences were first suspected antenatally among 41% of respondents and in 57% postnatally, with 2% unsure. Of the children, 54% were seen in a clinic by a specialist congenital hand surgeon within 3 months and 88% within 12 months, with 73% of respondents feeling unsupported after a diagnosis that was unexpected. Qualitative analysis outlined a broad spectrum of parental concerns about the quality of information received, especially regarding the child’s future biopsychosocial needs. This study showed the need for more support for parents from frontline healthcare professionals and the need for a streamlined referral pathway.
Introduction
The incidence of congenital hand and upper limb differences (CHULDs) varies between countries but generally occurs in 19.2–27.2 per 10,000 live births (Chan et al, 2022). These differences may range from simple accessory digits to complex presentations that affect the elbow, forearm, wrist and hand. Depending on the nature of the CHULD, it may be detected during antenatal ultrasonography or become evident only after birth. Observation of a CHULD either at birth or on an ultrasound scan is a traumatic experience for a parent. This unexpected revelation affects the parental dream of a ‘perfect’ child. The parent immediately wonders whether the child can function normally in life and how they will cope socially, and also has feelings of guilt relating to the cause of the anomaly.
Current practice within the UK’s National Health Service (NHS) is to offer expectant mothers an initial ultrasound scan at 8–14 weeks to determine gestational age, followed by detailed ultrasonography between 18+0 to 20+6 weeks to screen for 11 key physical conditions and to assess the fetus against a list of anatomical features set out by the Fetal Anomaly Screening Programme (FASP) ‘base menu’ (Public Health England, 2022). These conditions include confirmation of the presence of the humerus, radius and ulna bilaterally, although exact measurements of these skeletal structures are not required. Metacarpal presence is screened; however, a digit count is not required.
Antenatal detection of CHULD during this screening is not always straightforward; a window of opportunity presents at the end of the first trimester to the beginning of the second trimester (12–14 weeks), owing to the anatomical positioning of the hand in an extended, abducted position, before flexion occurs in later intrauterine periods (Bae et al., 2009). Prenatal sonographic assessment of upper limb anomalies becomes more difficult in distal differences, with reported sensitivities at 20%–30% for differences in the hand compared to more than 40% for differences in more proximal limb regions (Piper et al., 2015). As a result, a scan can be reported as ‘normal’, but a child can be born with a CHULD.
When an anomaly is suspected, the current UK standard according to the service specification is to inform the mother of the scan findings immediately and offer further investigation as per local protocol, or to have no further investigation (Public Health England, 2019). Previous consensus guidelines (Johnson et al., 2020) have provided a framework leading to discussions when an unexpected finding is noted on ultrasound; however, this does not relate specifically to CHULDs.
Reach (https://reach.org.uk/) is a UK based national support group for children with upper limb anomalies. The charity has an extensive network of parents of children with CHULDs. In this national cross-sectional study, we looked at the experiences of parents of children in the UK and Republic of Ireland when given the unexpected news of a CHULD, via the Reach network. We sought to determine the actual parental experience in the early few days after the surprising news and, with hindsight, whether parents preferred to be given a prenatal or postnatal diagnosis. The aim of the study was to see whether the support that parents received at this difficult time was adequate.
Methods
Ethics
This study was completed in accordance with the Helsinki Declaration as revised in 2013. We completed the Health Research Authority ethical advice tool, which confirmed the study did not require formal ethical review board.
Questionnaire development
A self-administered online questionnaire (Supplementary Figure S1, available online) was produced after a literature review, based on previous similar works by our group (Clelland et al., 2022). A multidisciplinary team, including two consultant congenital hand surgeons (RL, WLL) with Level 4 experience (Tang and Giddins, 2016), a nurse specialist (ÓD) in the psychosocial aspects of CHULDs and a small group of Reach members who are parents of children with CHULDs were involved in its development. The questionnaire was then piloted in 20 families for constructive feedback to improve construct validity and ensure sensitive means of questioning, with nine responses received. One question involved the rank-ordering of priorities, which was considered by one parent to be difficult to interpret and was subsequently removed. We used this feedback and an iterative process within our team to produce the final questionnaire.
The questionnaire collected basic demographic information and a parental description of the CHULD. It asked when they first suspected the diagnosis and what information was given then, and the time and route of referrals.
Data collection protocol
The survey was hosted via Google Forms (https://www.google.co.uk/forms/), between 23 September 2021 and 19 December 2021. A link was distributed via Reach to members and subsequently shared on social media to other charities supporting children with limb differences. Parents in the UK and Ireland with a child affected by a CHULD and aged 10 years or younger were included in the study. Parents who had received an unexpected diagnosis, either antenatally or postnatally, were included.
Analytical methods
We used a mixed-methods design for our study. This included the use of quantitative methods to assess parental experience and qualitative free-text responses, which could then by analysed to provide additional understanding of responses. Quantitative descriptive statistics were used to record the time taken to specialist consultation and to understand the experience of parents from discovery of the CHULD to diagnosis. The chi-square test with proportional calculation was used to identify significant differences between groups. A thematic analysis was carried out to identify themes within the qualitative responses (Braun et al., 2019). Two authors (ADC and RL) first familiarized themselves with the data independently. Anonymous information was subsequently coded on a spreadsheet and developed into subthemes and then themes. These were subsequently re-evaluated by the same authors to improve rigour and ensure that the themes reflected qualitative responses accurately. Representative quotations which describe the themes were noted.
Results
A total of 261 responses were collated over the 3-month period of the study.
Quantitative analysis
The diagnosis of CHULD was identified antenatally in 110 (41%) of respondents and in 150 (57%) postnatally, with 1 (2%) respondent being uncertain about when she was first given a diagnosis. Relevant information (as judged by the parents) was only given to 28% of all parents (Figure 1). In these cases, it was mostly provided by paediatricians (37%), followed by sonographers (25%), surgeons (24%) and midwives (14%). When asked, 51% of parents said they would have preferred to have received information about the child’s diagnosis before birth. Of the parents, 40% stated they would have liked to receive more information before the baby’s hospital discharge.
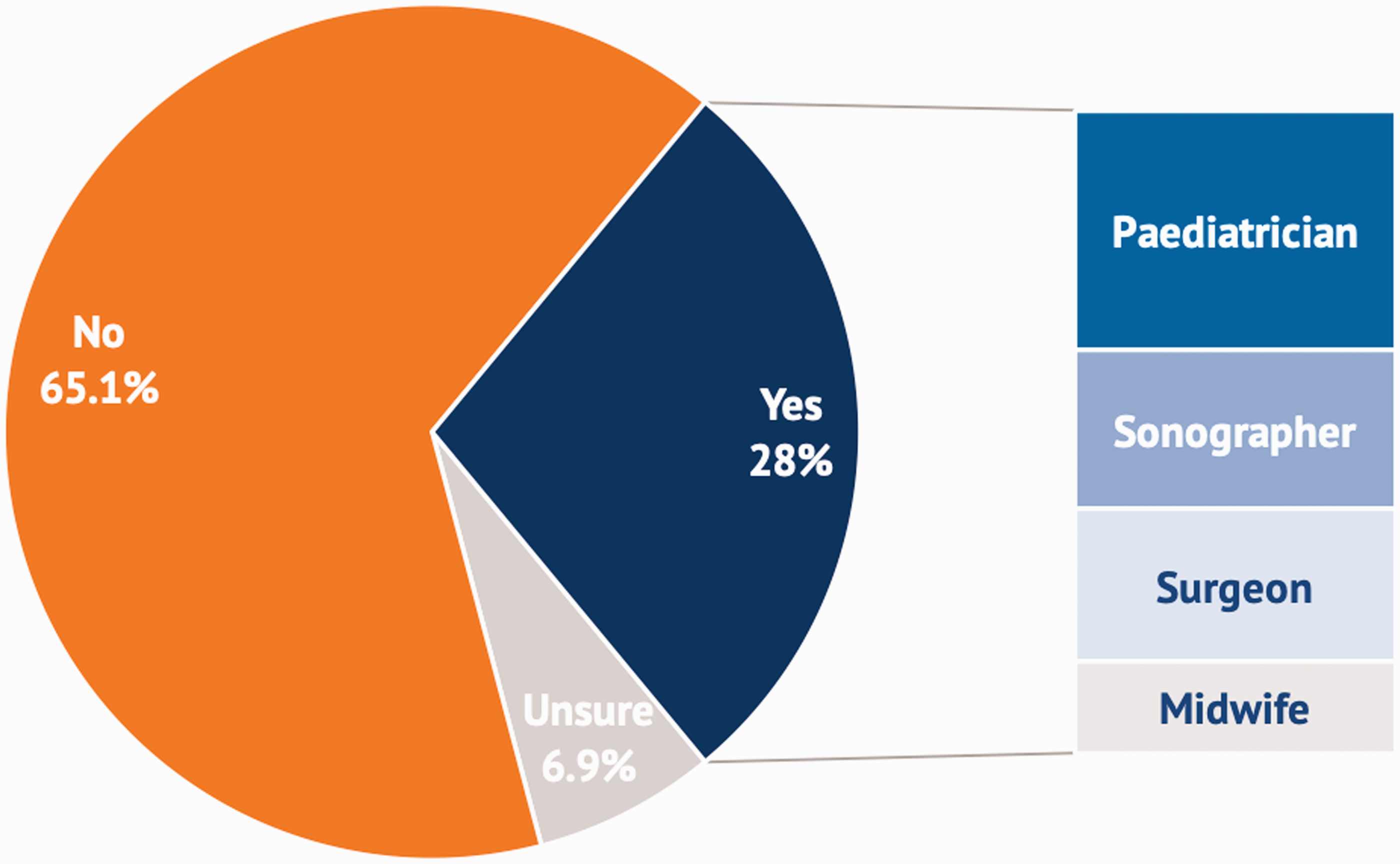
Percentage (%) of parents given information they considered relevant.
We enquired about when parents would have preferred to first learn about their child’s CHULD. Of the parents who were given their child’s diagnosis antenatally, 84% reported preferring to learn of the CHULD at this time. Conversely, of those who learned of the CHULD in the postnatal period, 61% stated this would be their preferred time to learn of the diagnosis. The proportion of those who would have preferred to learn about their child’s diagnosis in the postnatal period was statistically less, when analysed using a post-hoc chi-square test (p < 0.001).
Of the children, 54% were seen in clinic by a specialist congenital hand surgeon within 3 months and 88% within 12 months (Figure 2). However, it is of concern that 73% of parents described feeling unsupported after the surprising news and while waiting for their appointment, and 93% reported they had to search for information for themselves.
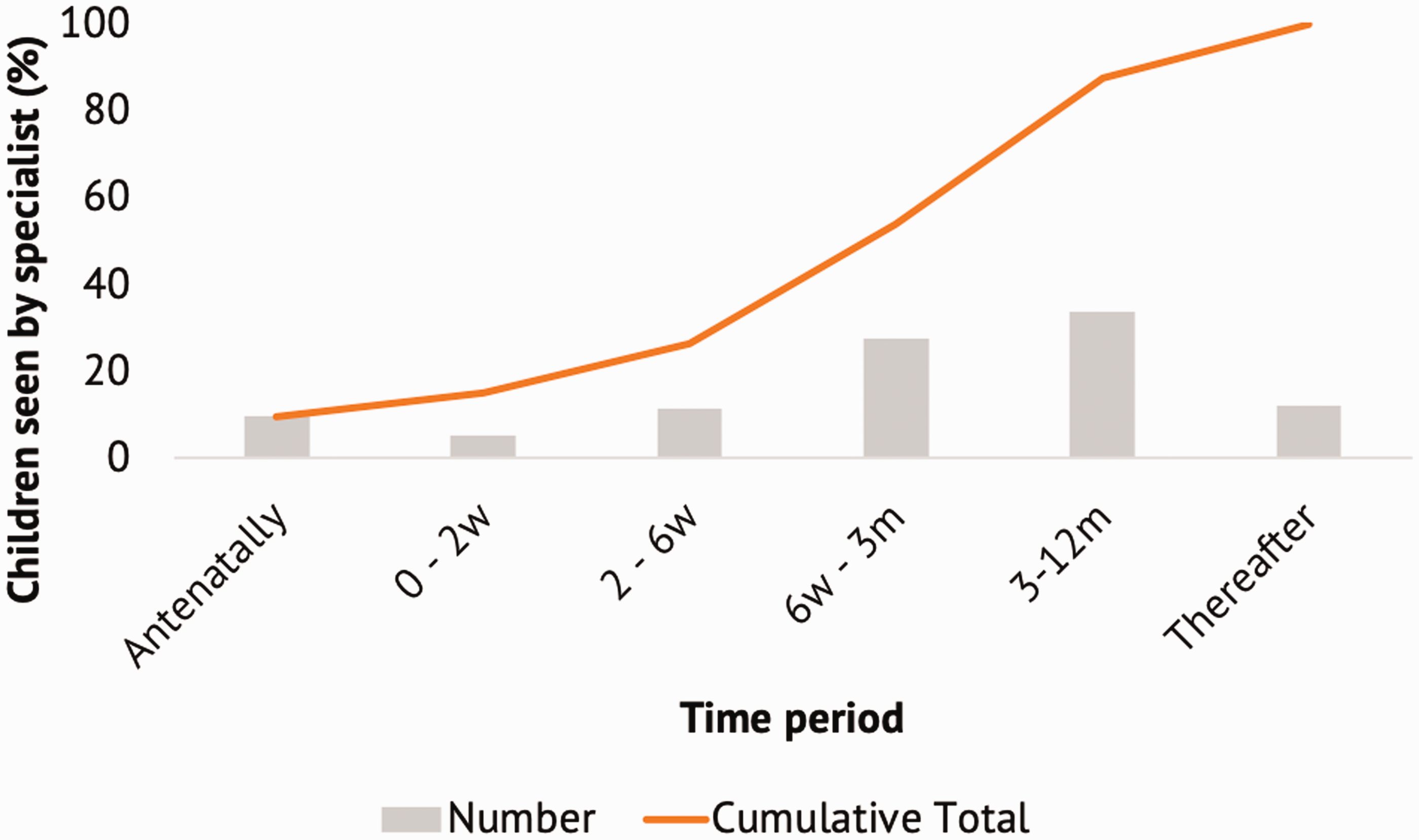
Time taken to for clinic consultation with specialist congenital hand surgeon.
Qualitative analysis
Results from the qualitative analysis are given in Table 1, which also displays representative quotations about the subthemes. The key themes were:
Qualitative analysis of parental responses.
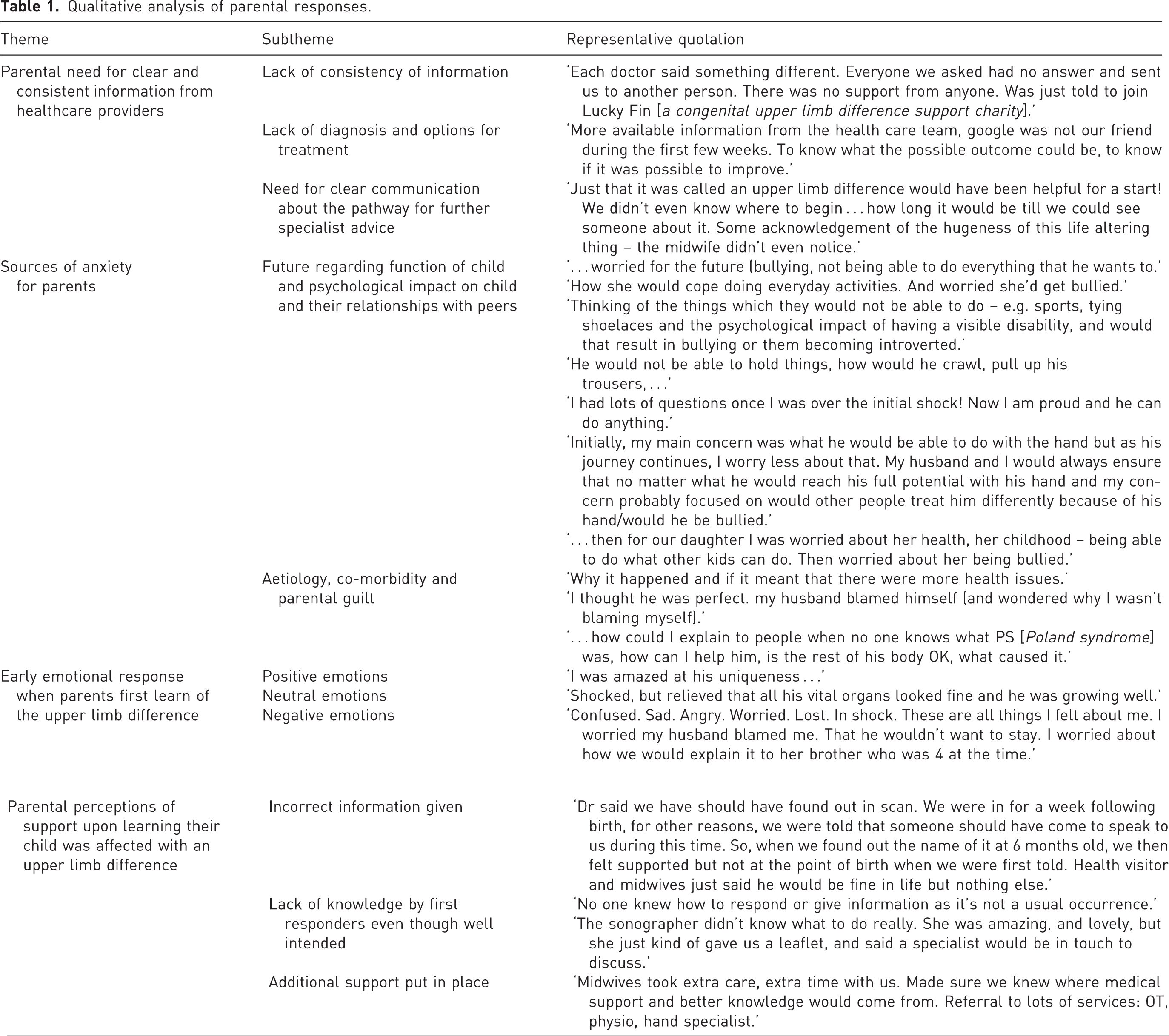
the need for clear and consistent information from healthcare providers at the point of diagnosis and subsequently;
parental anxiety about the future function and psychological impact as well as about the aetiology, co-morbidity and parental guilt;
a variety of early emotional responses on discovery of the upper limb difference for which they were unprepared;
parental perceptions of the available psychosocial support.
Discussion
We conducted a cross-sectional survey of the experiences of parents from the UK and Ireland after an unexpected diagnosis of a CHULD. From our study, more congenital hand anomalies were detected in the postnatal period than in the antenatal period. Parents generally felt unsupported at the initial point of diagnosis. Relevant information was given to only 28% of parents surveyed, mostly by paediatricians.
A previous study investigating parental experiences of ante- and postnatal diagnosis in cleft lip and palate (Berggren et al., 2012) found a lack of quality information at the original sites from which children were referred, with parents being more satisfied by information given by the specialist cleft team. A previous study within the present authors’ institution (Clelland et al., 2022) identified a desire for rather more detailed embryological knowledge and quality information by parents, irrespective of the complexity of limb differences. These studies highlight the need for quality information to be made available to parents of children with congenital anomalies in a timely manner until they can see a specialist. Although we found that 57% of CHULDs are detected postnatally, only 28% of parents were given information relevant to their child’s condition immediately after receiving the news of the limb difference in their baby.
In addition to being given quality information at the time of diagnosis, parents expressed a need to see someone with more expertise sooner. Just over half (54%) were seen within a specialist clinic within 3 months. Although many were referred to a specialist within 6 months, many parents felt that the centre where they first learned of the CHULD was ill-equipped to provide the support they required at that time, including mental health support for their own wellbeing. Although it is understandable that a frontline healthcare professional will not be equipped to give this information, their approach is crucial to how the vulnerable parents manages their initial anxieties and wellbeing and thus their ability to support their own child with limb differences.
A spectrum of emotions was experienced by parents. These included positivity about the ‘uniqueness’ of their child and relief when there was an isolated CHULD without major organ dysfunction, to negative feelings of sadness, anger and self-blame. This may be in keeping with a recent qualitative analysis of interviews of children with CHULD that reported that they often feel ‘special’ and that their surgical scars confer a degree of bravery (McDougall et al., 2021). Some parents commented that even an awareness of the support for families with new upper limb differences provided by Reach would have brought comfort. It is conceivable that early information from reliable resources may have resulted in fewer searching for information themselves than the 93% we report. However, most parents still went through a grieving experience after a diagnosis, as it affected their wish for a perfect child. Furthermore, the qualitative responses showed concerns and anxieties about how the child would function later in life, how other family members would respond and whether the child would face bullying. Similar themes were shown previously in a study of 40 patients and their parents by Franzblau et al. (2015) in which individual stressors were identified. They reported that a mix of positive and negative coping strategies were adopted by families; however, the effects of early information giving was not explored.
In a recent study by the Australian Hand Difference Registry, 21% of CHULDs were detected antenatally (O’Keefe et al., 2022), in contrast to 41% in this study. This may be explained by a degree of recall bias, given that there were similar ultrasonography programmes. Berggren et al. (2012) reported in their cleft lip and palate cohort that those who learned of the diagnosis postnatally would have preferred to learn antenatally. In contrast, we found that parents who learned of the difference before birth would still like to have known antenatally but those who learned postnatally preferred to learn within the postnatal period. Perhaps there is no good time to be given a diagnosis; knowing about a diagnosis before birth allowed the parents to be more prepared for the child’s arrival and to seek antenatal and genetic investigations and counselling. A recent systematic review that included three articles assessing parental anxiety in prenatal congenital diagnoses found that antenatal counselling can significantly reduce this anxiety (Marokakis et al., 2016). Conversely, learning about the diagnosis in the postnatal period may allow the parents to have a less stressful pregnancy. The level of anxiety may also be less for some as they can be assured that there is an isolated congenital hand difference in an otherwise healthy baby, after the child had been born and checked by a paediatrician.
Ideally, a child born with a CHULD should be seen as soon as possible by a specialist to provide the best professional advice to parents. Furthermore, an early consultation allows surgery to be planned and treatment started, if necessary. A recent UK consensus (Jester, 2023) suggested reference timings for congenital hand procedures, with some procedures recommended from 12 months but others earlier. Early specialist diagnosis would allow these targets to be met. Some conditions, e.g. radial dysplasia, would also benefit from splinting from the time of birth to facilitate subsequent surgery.
The present study has some limitations. First, although the data were obtained from all regions of the UK and Ireland, most participants were those already known to Reach or other charities. There may be underrepresentation of affected families who are not involved with such a charity and who may have different experiences within the healthcare system. Second, as the results were parent-reported, there may be inaccuracies in the diagnoses and recall bias, as previously noted. The information about diagnoses was omitted as these were not clinician-reported, with many diagnoses being unknown.
We can identify three key areas of improvement within the healthcare system that should provide reassurance and ameliorate the distress, feelings of isolation and self- blame experienced by parents who receive the unexpected news that their child has a CHULD. They are:
streamlining diagnostic pathways from the time of diagnosis to referral to the congenital hand specialist surgeon; provision of relevant early information for parents and frontline healthcare professionals; psychological support for parents pending the specialist appointment.
Because of the rarity of these conditions, most healthcare professionals other than congenital hand surgeons dealing with congenital disorders may only see one or two cases during their careers. Therefore, it is incumbent on specialist upper limb surgeons to make sure that the first responders are equipped with the right knowledge, positive attitude and information about charities such as Reach, so that they may support new parents faced with an infant with a visible hand and upper limb difference.
Supplemental Material
sj-pdf-1-jhs-10.1177_17531934241249014 - Supplemental material for Parental experience after diagnosis of a congenital upper limb difference: a national survey
Supplemental material, sj-pdf-1-jhs-10.1177_17531934241249014 for Parental experience after diagnosis of a congenital upper limb difference: a national survey by Andrew D. Clelland, Ruth Lester, Órla Duncan and Wee L. Lam in Journal of Hand Surgery (European Volume)
Footnotes
Acknowledgements
We would like to thank Deborah Bond and Kate Hoare, previous Reach.org employees, for their assistance in developing and distributing the survey. We would also like to thank the trustees of Reach.org for their support. We also give a massive thank you to all the parents who took the time to respond to the survey.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
This study was completed in accordance with the Helsinki Declaration as revised in 2013. Ethical exclusion was obtained after completion of the Health Research Authority ethical advice tool.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by The British Society for Surgery of the Hand through an Educational Bursary (18/10/2021). This body had no input in the study design, implementation, interpretation or publication of this study. This work was presented at the International Federation of Societies for Surgery of the Hand in London in 2022 and the 2023 World Symposium on Congenital Malformations of the Hand and Upper Limb.
Informed consent
Participation in the survey was optional. An explanation for the use of data collected was provided on the cover letter. Participants could quit at any point until submission, after which anonymous data were collated and included for analysis.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.