
Abstract
Although trigger thumb release is commonly performed, there is no consensus on the optimal skin incision. This study aimed to compare outcomes of four incision techniques, including V-shaped, oblique, transverse and longitudinal incisions. Outcomes included the Michigan Hand Outcomes Questionnaire, satisfaction with the treatment and postoperative complications. The results of 875 patients who underwent trigger thumb release were assessed. All groups demonstrated improvement in self-reported hand function (range of 10–14 points), pain (25–27 points) and aesthetics (4–7 points) from baseline to 3 months postoperatively with no differences between incision techniques. Of the patients, 76% reported good or excellent satisfaction with the outcome of treatment. Satisfaction and complication rates of the different incision techniques were similar. These findings imply that there is no clear benefit of one type of incision over another for trigger thumb release, suggesting that surgeons may use the technique of their preference.
Keywords
Introduction
Although open release of a trigger thumb is one of the most commonly performed operations for hand conditions, there is considerable variation in skin incisions used to approach the A1 pulley (Dijksterhuis et al., 2022). The incision pattern that a surgeon performs most likely depends on their surgical training rather than on evidence, experience and testing of the different incision techniques. Hence, there is no consensus on which incision technique is preferable in terms of patient-reported outcomes and complications (Dijksterhuis et al., 2022).
Two randomized clinical trials have evaluated whether the incision technique affects scar quality and patient-reported outcomes after open A1 pulley release for trigger finger (Kazmers et al., 2019; Kloeters et al., 2016). They found no differences in scar quality and Disabilities of the Arm, Shoulder and Hand (DASH) scores between longitudinal and transverse incisions at 3 and 12 months postoperatively. However, both studies excluded patients with a trigger thumb, which may require a different approach, especially considering the superficial course of the neurovascular bundles. While a longitudinal incision provides good exposure of the A1 pulley and the neurovascular bundle, it may yield a higher risk of scar contracture. In contrast, transverse incisions may reduce scar contractures, but the minimal exposure may pose a higher risk of neurovascular damage. Although both oblique and V-shaped incisions provide good exposure of the A1 pulley and may yield a lower risk of scar contracture, the wide dissection may increase the risk of neurovascular damage (Bell, 2009). Considering that all incision techniques yield both favourable and unfavourable arguments, there is no consensus on the optimal type.
The outcomes of a large cohort of trigger finger and thumb releases were previously reported by our group (Koopman et al., 2022). The aim of the present study was to further analyse the patients from this cohort who had had open A1 pulley release for a trigger thumb release in order to compare patient-reported outcomes and postoperative complications of four incision techniques (i.e. V-shaped, oblique, transverse and longitudinal).
Methods
This is a cohort study of patients who underwent open A1 pulley release for a trigger thumb using data from the Hand-Wrist Study Cohort (i.e. a longitudinally maintained database of patients with hand and wrist conditions), reported according to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement (von Elm et al., 2007). Between January 2013 and May 2020, data were collected as part of routine outcome measurements at Xpert Clinics Hand and Wrist Care, currently comprising 25 locations for hand surgery and hand therapy in The Netherlands, 23 European Board-certified hand surgeons and over 150 hand therapists. The cohort and data collection (Selles et al., 2020; Wouters et al., 2021) and their use in daily clinical care (Feitz et al., 2021) have been described previously. Ethical approval for this study was obtained from the medical ethics review committee of the Erasmus Medical Centre. All patients provided written informed consent to be included in our database.
Participants
Patients were eligible for inclusion if they underwent open A1 pulley release for a trigger thumb. Patients were excluded for the following reasons: (1) they had undergone a previous A1 pulley release of the thumb; (2) they had undergone surgical treatment on the ipsilateral or contralateral hand within 3 months before the A1 pulley release; (3) they underwent an additional procedure during the same session (e.g. carpal tunnel release); (4) the incision technique was unknown; or (5) there were missing data at baseline or 3 months postoperatively.
Treatment
All operations were performed by hand surgeons certified by the Federation of European Societies for Surgery of the Hand, with experience levels ranging from 2 to 5 (Tang and Giddins, 2016). The decision for surgery was based on shared decision-making between the patient and surgeon. Most patients underwent surgery after failed conservative treatment. Indications for surgery typically included active triggering and/or tenderness at the A1 pulley. The release procedures were performed in the operating room under local anaesthesia. The incision technique was based on the surgeon’s preference. Operative records were reviewed, and surgeons were contacted to confirm the incision technique they perform and that this has not changed over time. Incision techniques included V-shaped, oblique, transverse and longitudinal incisions (Figure 1). The wounds were closed using non-absorbable sutures, which were removed 10–14 days postoperatively. All patients were offered standardized postoperative treatment, including a dressing for 3–5 days and three sessions of supervised hand therapy comprising tendon gliding exercises (Huisstede et al., 2014) and scar management. Each patient had a follow-up appointment with their hand surgeon 3 months postoperatively to evaluate the treatment outcome. Additional sessions with the hand surgeon or hand therapist were scheduled when indicated.
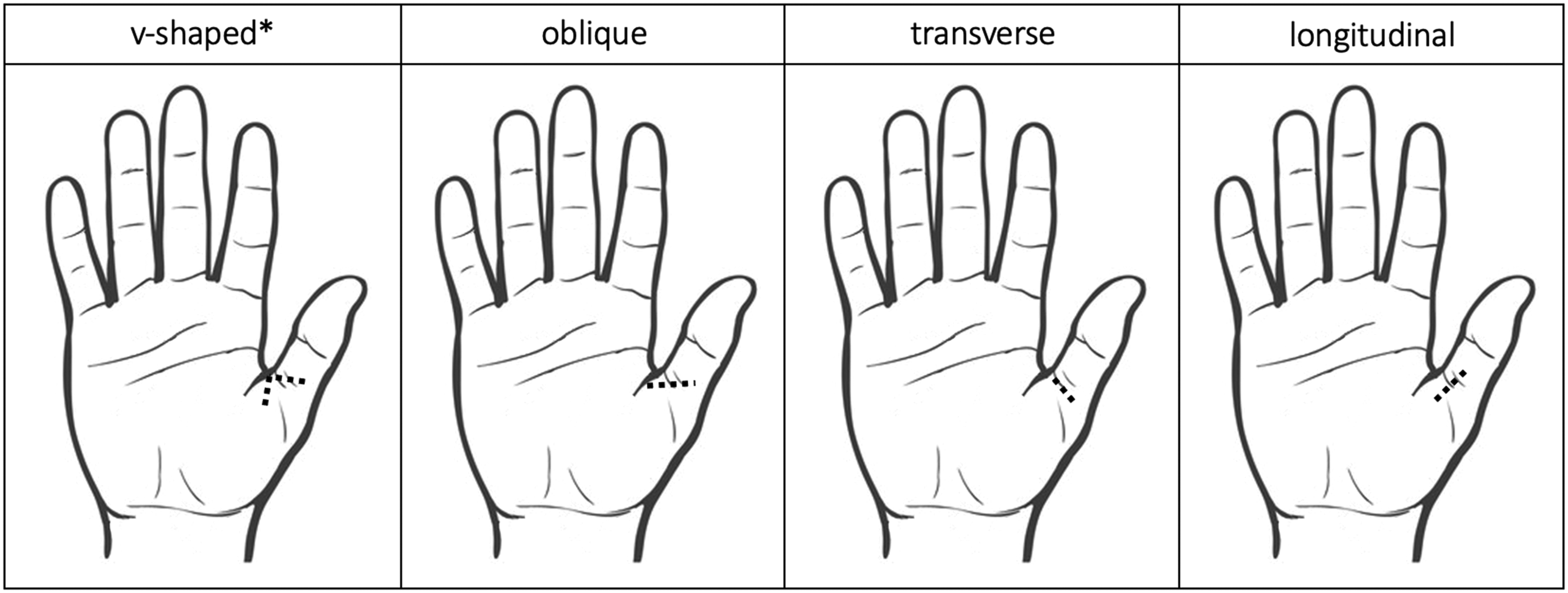
Schematic illustration of the four incision techniques performed in this study. *Depending on the surgeon, the position of the apex could either be radial or ulnar.
Variables and measurements
The primary outcome was the Michigan Hand Outcomes Questionnaire (MHQ) (Chung et al., 1998). All patients were invited to complete the MHQ Dutch language version (Huijsmans et al., 2001) preoperatively and 3 months postoperatively (Selles et al., 2020; Wouters et al., 2021). The MHQ is a validated patient-reported outcome measure evaluating six subdomains with scores in the range of 0–100: overall hand function; activities of daily living; work performance; pain; aesthetics; and satisfaction with hand function. In this study, we only assessed the hand function, pain and aesthetics subdomains of the MHQ as these were considered most relevant. For interpretability, we reversed the scores of the pain subdomain so that higher scores of each subdomain indicate better performance. Previous literature has demonstrated that the minimal important change is 16 points for the pain subdomain and 6 points for the hand function subdomain in patients undergoing trigger thumb release (Hoogendam et al., 2022). Patients were also invited to complete the Satisfaction with the Treatment Result questionnaire (De Ridder et al., 2021) at 3 months postoperatively. This questionnaire evaluates the patient’s satisfaction with treatment results on a 5-point Likert scale. The questionnaire has a good-to-excellent construct validity and high test-retest validity (De Ridder et al., 2021).
Baseline characteristics routinely collected included age, sex, current smoking, type of work, hand dominance, treatment side and symptom duration. In addition, information on previous treatment with steroid injections and the occurrence of complications was extracted from the medical records. In accordance with the International Consortium for Health Outcome Measurement Complications in hand and wrist conditions (ICHAW) guidelines (Wouters et al., 2021), all deviations from the expected treatment course related to the intervention were considered complications. We considered the following as part of the expected treatment course: sutures removed at 10–14 days; hand therapy phased out at 3 months; and no additional treatment recommendations from the 3-month check-up visit onwards. Within the ICHAW guidelines, the severity of a complication (i.e. grade) is based on the invasiveness of the intervention required. The grades are defined as follows: grade 1 = treatment with additional hand therapy, splinting or analgesics; grade 2 = treatment with antibiotics or steroid injections; grade 3A = minor surgical treatment; grade 3B = major surgical treatment; and grade 3C =complex regional pain syndrome. Only the most severe complication was documented in the case of multiple events within the same patient.
Statistical analysis
Univariable comparisons of baseline characteristics between groups were performed with analysis of variance tests and chi-square tests. When expected values were below five for categorical data, Fisher’s exact tests were used. We performed a non-responder analysis comparing baseline characteristics of patients who completed (responders) and those who did not complete (non-responders) the MHQ at 3 months postoperatively using t-tests, Wilcoxon tests and chi-square tests. Effect sizes for the differences were calculated using Cohen’s d for continuous variables and Cliff’s delta for categorical variables. Despite a higher percentage of men among non-responders (effect size 0.06), we found no differences in baseline characteristics (Table S1).
Paired t-tests were used to compare preoperative and postoperative MHQ scores. For between-group comparisons of MHQ scores, we performed analysis of covariance tests. Baseline characteristics (e.g. age, sex, symptom duration, MHQ baseline scores) were included as covariates in the analyses to correct for potential between-group differences. Multivariable logistic regression analyses were used to compare satisfaction with the treatment result and complications between groups (secondary outcomes). We dichotomized patient satisfaction, considering the answering options excellent and good as satisfied and fair, moderate and poor as unsatisfied as recommended by De Ridder et al. (2021). Regarding complications, we only compared the total number of complications between groups as we expected a low number of complications. The overall effect of incision technique was evaluated using analysis of variance tables. When an overall difference in group means was observed, post-hoc Tukey tests were performed to examine specific between-group differences. Model assumptions were checked by plotting fitted values and residuals, QQ plots and variance inflation factors (James et al., 2013).
To determine whether this study was sufficiently powered, we performed a post hoc power calculation for an analysis of covariance test with the MHQ hand function score 3 months postoperatively as the outcome. We aimed to detect a difference of −5 in postoperative MHQ scores for the treatment group with the lowest postoperative score (i.e. oblique incision) and +5 for the treatment group with the highest postoperative score (i.e. longitudinal incision) compared to the mean score. A post hoc power analysis for an analysis of covariance test with four groups, 11 covariates, observed numbers of patients in each group, observed mean and standard deviation, R2 of 0.21 (Koopman et al., 2022) and alpha of 0.05 showed that our study was sufficiently powered (power 99%) to detect this difference (Shieh, 2020). In addition, we performed a linear mixed-model analysis to examine clustering between surgeons as a possible proxy for differences in patient selection or management and found an intraclass correlation coefficient of 0.002. This indicated that the variation mainly exists within surgeons (caused by patient variation) and not between surgeons. Hence, we did not account for clustering per surgeon in our analyses. For all tests, a p-value below 0.05 was considered statistically significant.
Results
After exclusions, we included 875 patients in this study (Figure 2). Most patients were treated using a V-shaped incision (60% of all patients, treated by 13 surgeons), followed by oblique (26%, 7 surgeons), transverse (8%, 6 surgeons) and longitudinal incisions (6%, 2 surgeons). The participants had a mean age of 58 years and 82% were women (Table 1). The median duration of symptoms was 6 months and 57% had undergone previous treatment with steroid injections. We found no differences in baseline characteristics between incision techniques.
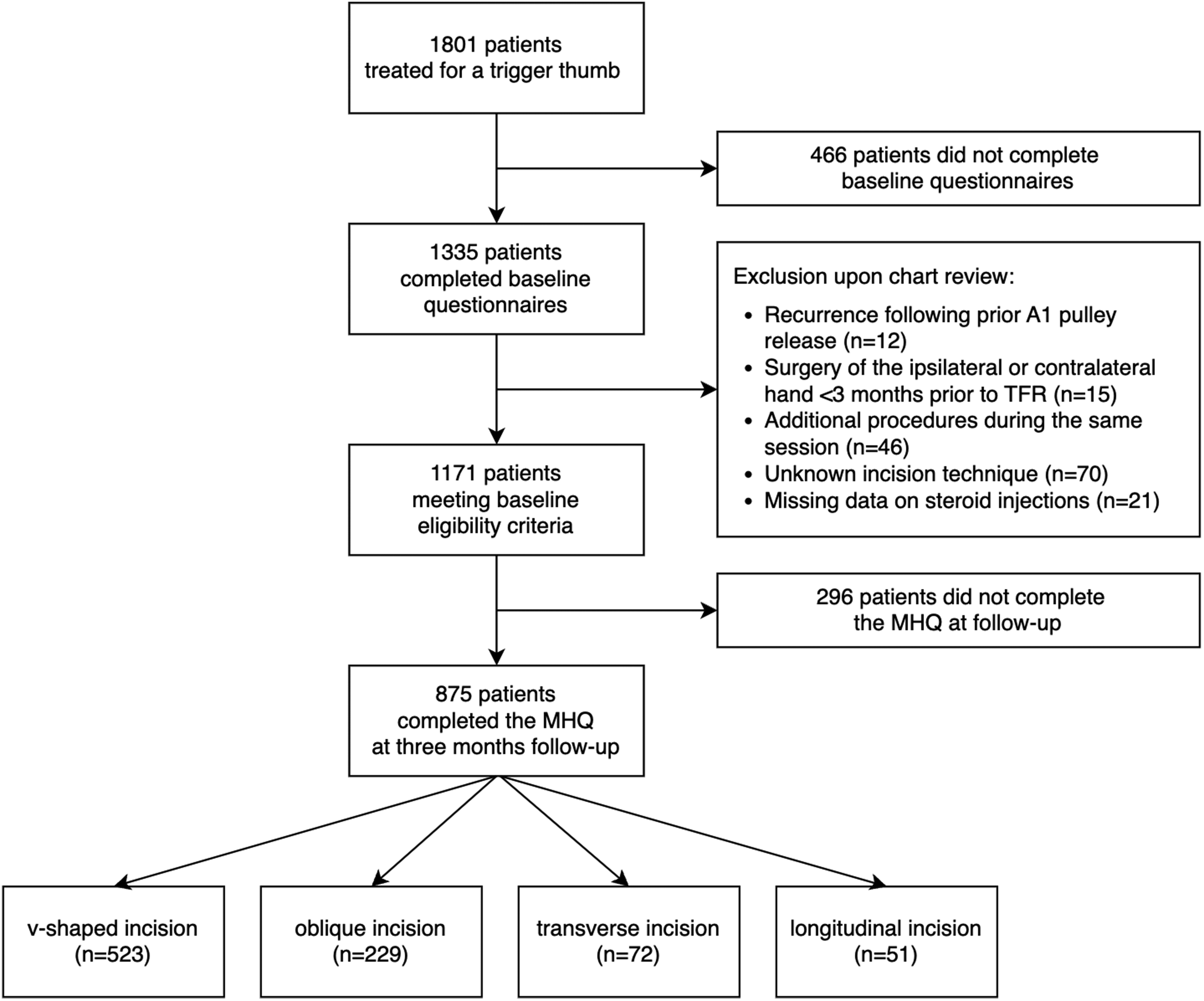
Flow diagram of the study.
Baseline characteristics according to treatment group.
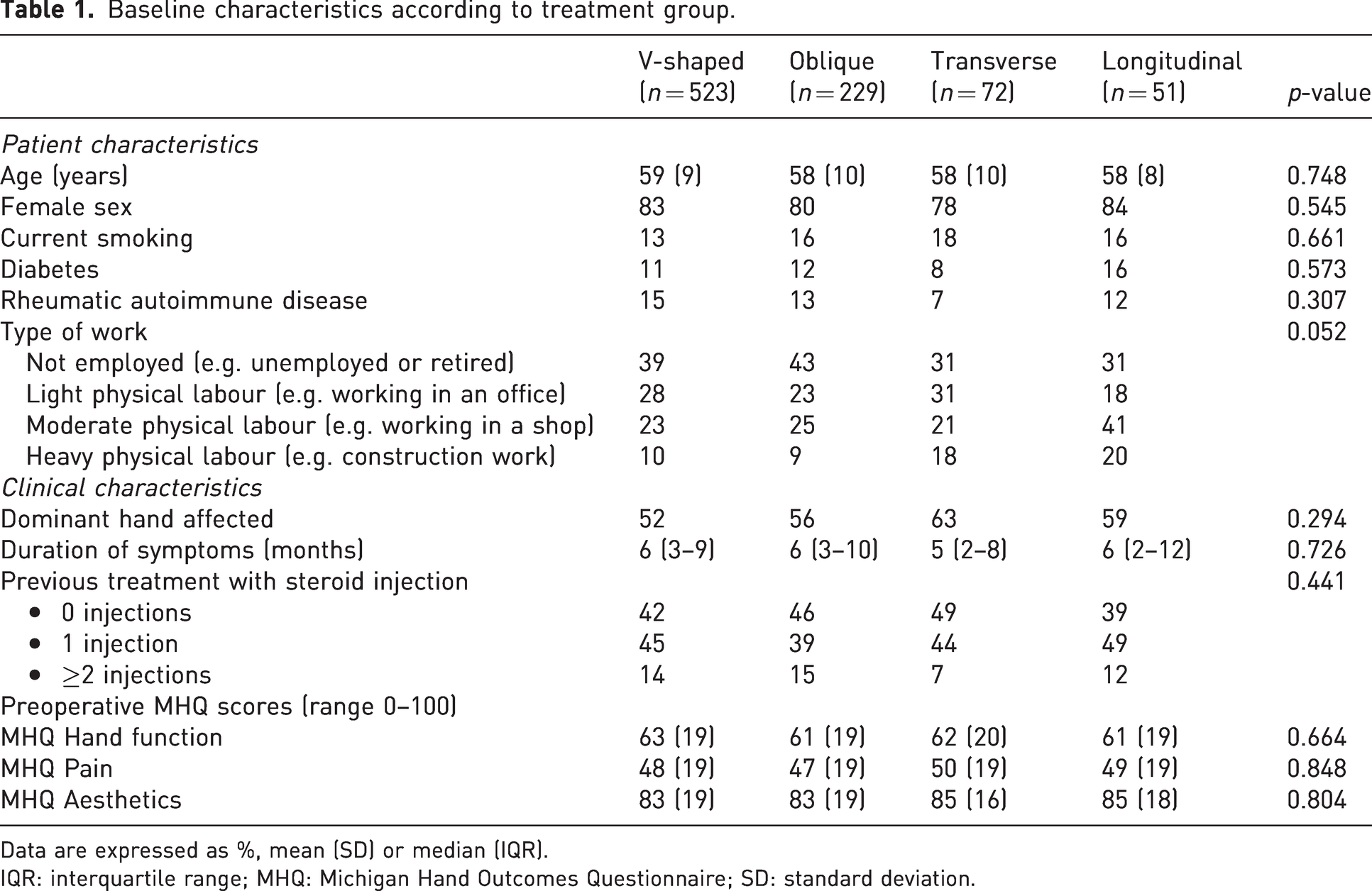
Data are expressed as %, mean (SD) or median (IQR).
IQR: interquartile range; MHQ: Michigan Hand Outcomes Questionnaire; SD: standard deviation.
Michigan Hand Outcomes Questionnaire
Figure 3 shows the change in MHQ scores from baseline to 3 months postoperatively for the different incision techniques. For all treatment groups, there was an improvement in mean hand function scores from baseline to 3 months postoperatively, ranging from 10 to 14 points (p <0.05). There were no differences between the incision techniques (p = 0.370). Regarding pain scores, all treatment groups demonstrated improvement from baseline to 3 months ranging from 25 to 27 points (p <0.05). Again, there were no differences between groups (p = 0.496). For aesthetics, mean improvement was in the range of 4–7 points (p <0.05) with no differences between groups (p = 0.708). The changes in MHQ scores were normally distributed (Figure 4). Overall, 23% of patients reported worse hand function, 11% worse pain and 18% worse appearance of the hand.
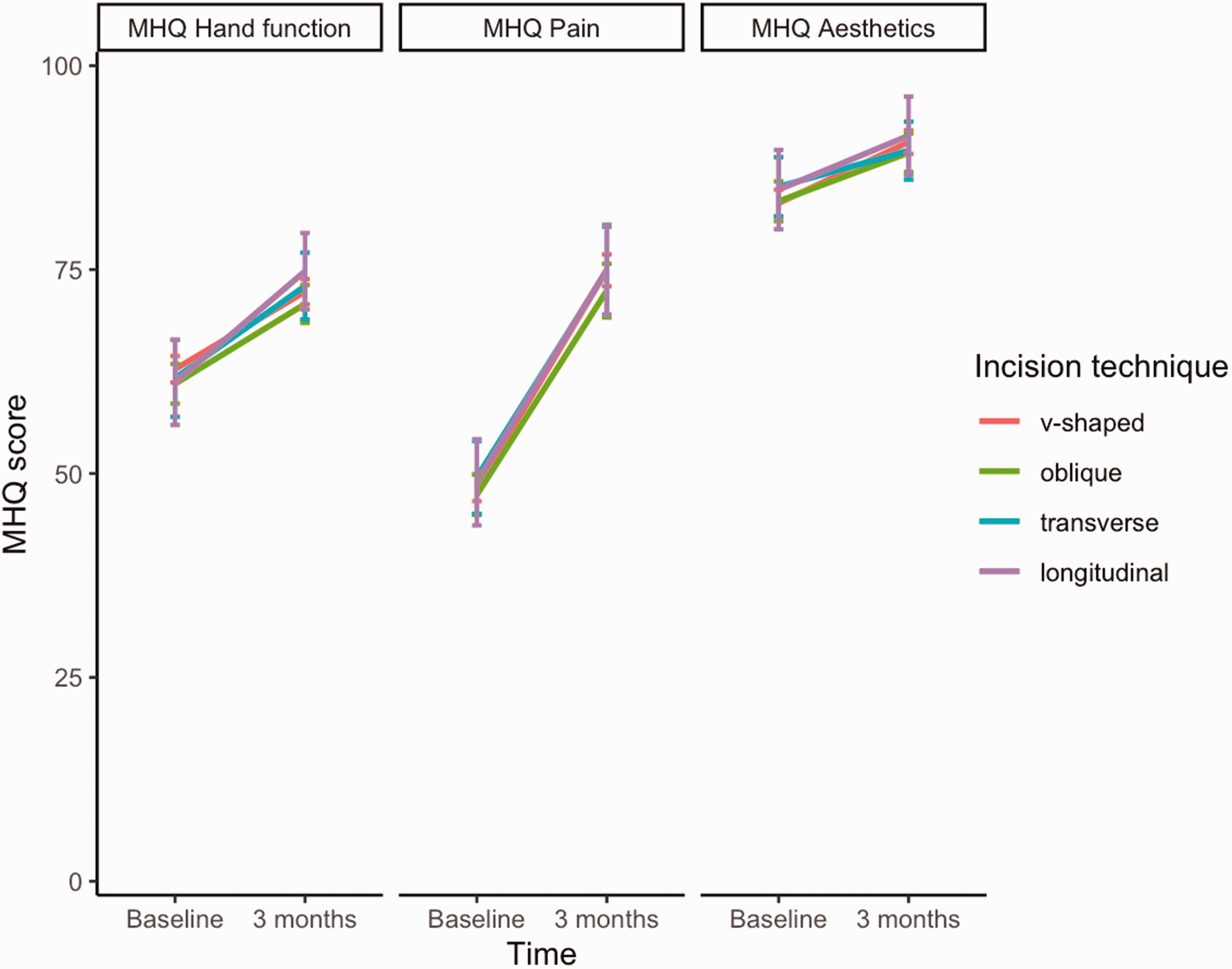
MHQ scores (0–100, higher scores indicate better outcomes) for the hand function, pain and aesthetics subdomains at baseline and 3 months postoperatively according to type of incision. Results are presented as means and corresponding 95% confidence intervals.
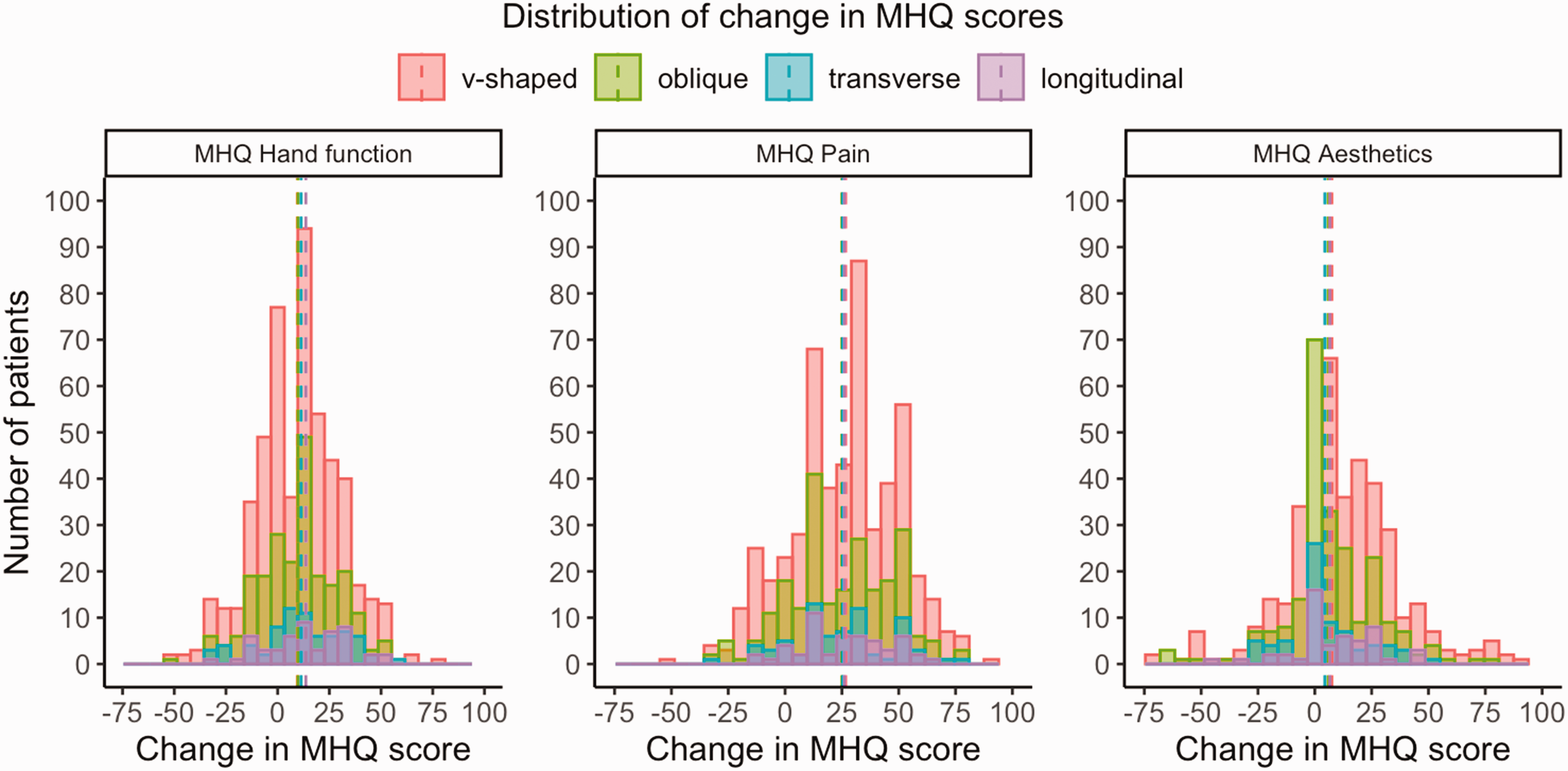
Distribution of change in MHQ scores for the hand function, pain and aesthetics subdomains from baseline to 3 months postoperatively according to type of incision. Positive scores indicate an improvement from baseline to 3 months. The dashed lines represent the mean change in MHQ scores.
Satisfaction with treatment
Seventy-six percent of all patients rated their satisfaction with treatment results as excellent or good 3 months postoperatively (Figure 5). We found no difference in satisfaction between the incision types (p = 0.368).
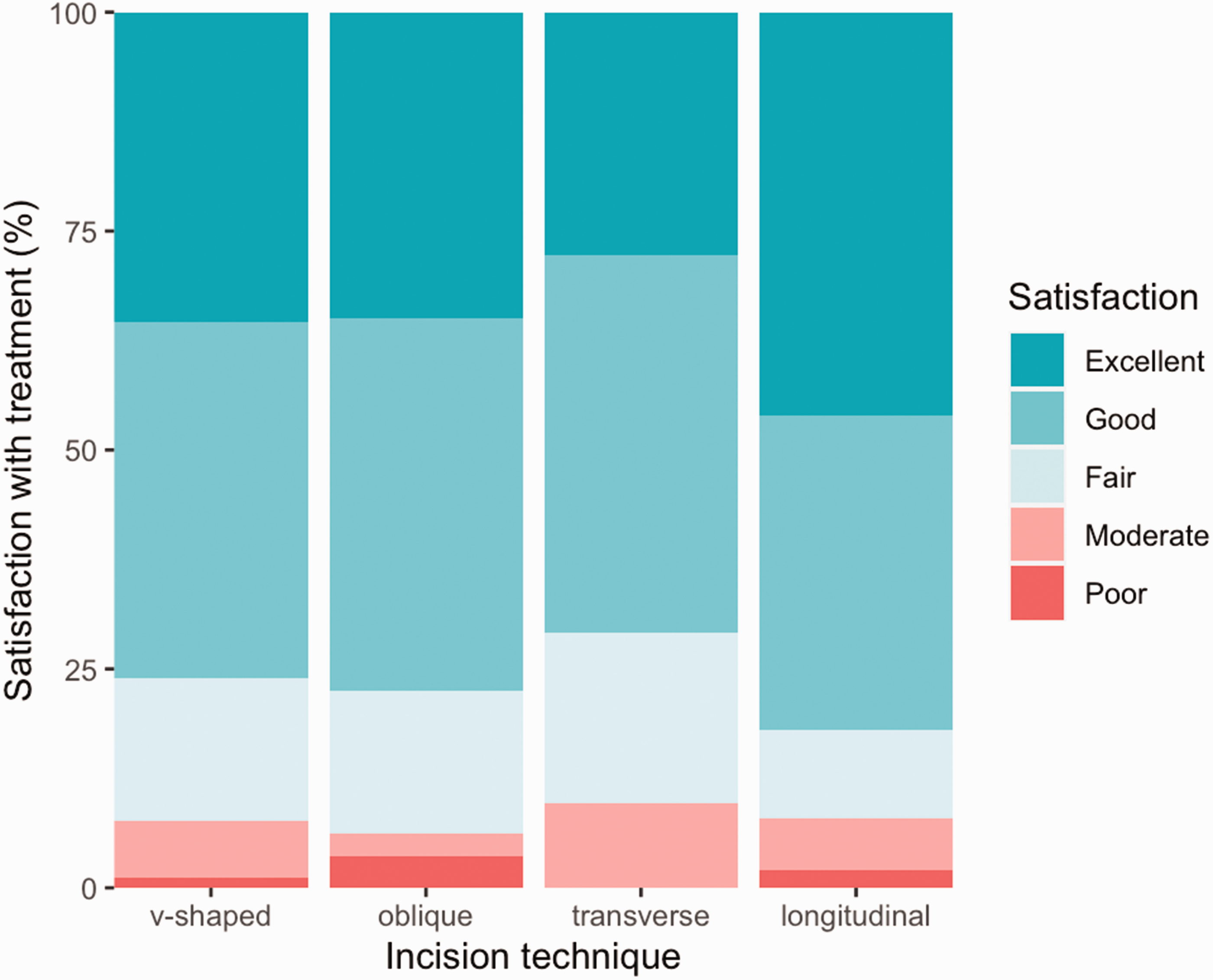
Bar chart of patients’ satisfaction with treatment 3 months postoperatively according to incision type.
Complications
Table 2 provides an overview of the complication rates according to the incision techniques. In total, 101 (12%) patients incurred a complication. Most complications were mild, requiring conservative management (4% of all patients), antibiotics (4%) or steroid injections (2%), and 1% of patients required surgical treatment. Indications for reoperation included surgical drainage of an infection (n = 2), recurrent triggering (n = 2), neurolysis of a digital nerve (n = 2) and release of adhesions (n = 1). We observed no difference in complication rates between groups (p = 0.896).
Complication rates (%) according to incision technique.
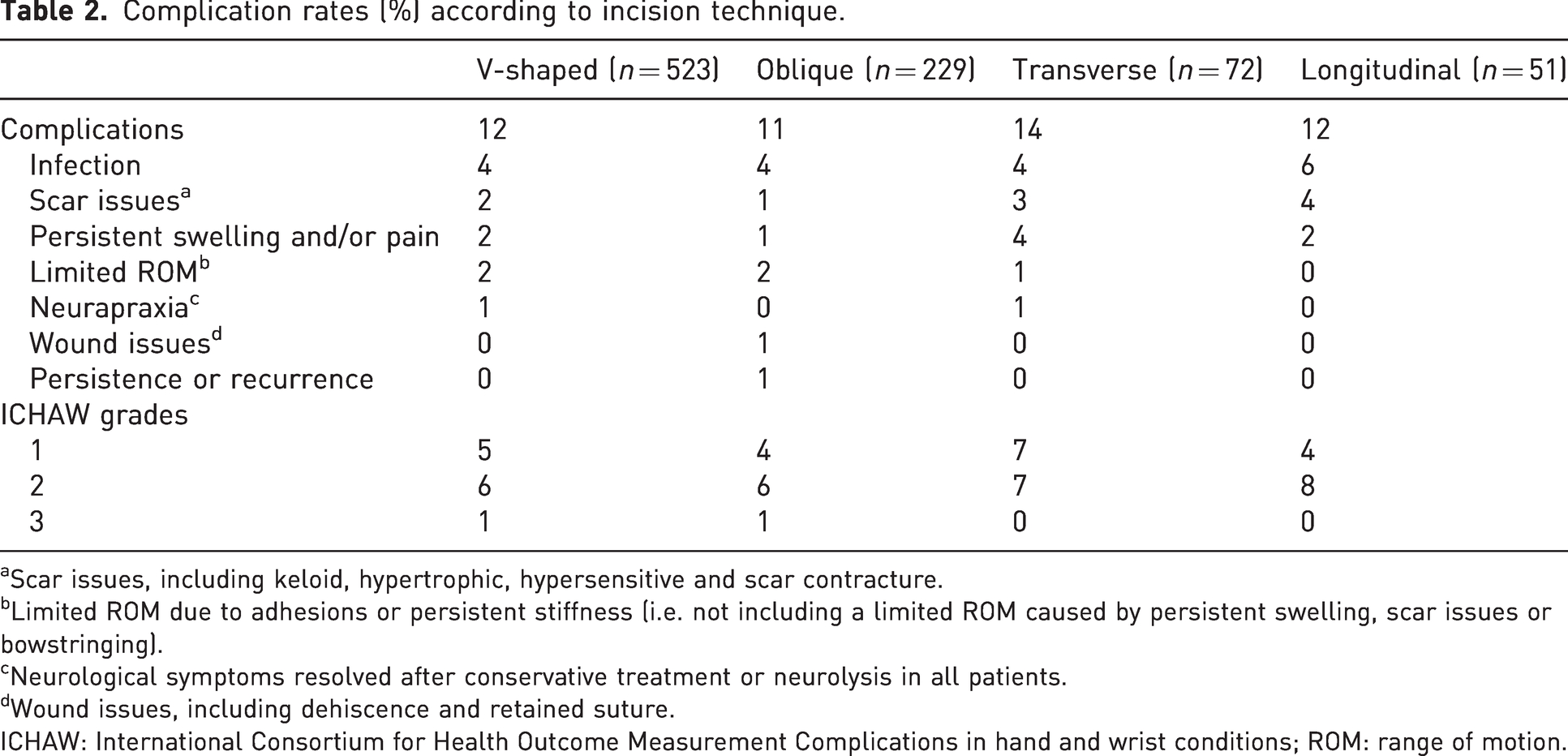
Scar issues, including keloid, hypertrophic, hypersensitive and scar contracture.
Limited ROM due to adhesions or persistent stiffness (i.e. not including a limited ROM caused by persistent swelling, scar issues or bowstringing).
Neurological symptoms resolved after conservative treatment or neurolysis in all patients.
Wound issues, including dehiscence and retained suture.
ICHAW: International Consortium for Health Outcome Measurement Complications in hand and wrist conditions; ROM: range of motion.
Discussion
While all four incision techniques yield both favourable and unfavourable arguments for their use in trigger thumb release, we found that all incision groups demonstrated an improvement in self-reported hand function, pain and aesthetics with no between-group differences. In addition, satisfaction and complication rates were similar between groups. These findings indicate that there is no clear benefit of one incision technique over another for trigger thumb release, suggesting that surgeons may use the technique of their preference.
Our study aligns with previous studies, demonstrating good outcomes after A1 pulley release with a low proportion of severe complications (Bruijnzeel et al., 2012; Everding et al., 2015; Ng et al., 2020; Nikolaou et al., 2017; Stirling et al., 2020; Strigelli et al., 2019).
In our cohort, the majority of patients were treated with a V-shaped or oblique incision. While longitudinal incisions are frequently used for A1 pulley release of the fingers, some discourage their use for trigger thumb release as there may be a higher risk of scar contractures. In contrast, a transverse incision provides less exposure for longitudinal release of the pulley and may increase the risk of damage to the superficial neurovascular bundles. Other than a very small proportion of patients with neurapraxia that resolved after conservative treatment or neurolysis (0.8%), there were no cases of neurovascular damage. In addition, we found a low proportion of scar issues requiring the prescription of additional treatment (e.g. silicone gel sheet) in all groups and no differences in self-reported aesthetics between groups. Although these findings suggest no substantial differences in scar quality, it should be acknowledged that we did not evaluate scar quality using a validated scar assessment instrument (e.g. Observer Scar Assessment Scale (Singer et al., 2007)). While such an instrument may have added to this study as it is more sensitive to detect small differences in scar quality, we believe that the proportion of patients experiencing considerable scar issues (i.e. requiring additional treatment) may be more relevant from the patient’s perspective.
The strengths of this study include the large sample with prospectively collected data. In addition, surgery was performed by 28 surgeons at 25 different clinics. As a result, the outcomes of this observational cohort are highly representative of actual daily practice, resulting in more generalizable findings. A limitation of the observational design of this study is the relatively high number of patients lost to follow-up, which is inherent to the registration system used. In our practices, patients are invited to voluntarily complete questionnaires at set times during follow-up, and reminders are sent twice. Our comparative analysis of baseline characteristics between responders and non-responders only demonstrated that non-responders were more often men. However, considering the small effect size (0.06), we do not believe this impacts our findings. Second, one could argue that the lack of randomization between the incision techniques poses a risk for selection bias. However, as surgeons typically used one incision technique for their patients, we believe that the incision technique was mainly based on surgeon preference rather than selection bias. Furthermore, since we found no differences in baseline characteristics between groups and our analyses demonstrated no between-group differences after correcting for baseline characteristics, we advocate that the non-randomized comparison seems valid.
Supplemental Material
sj-pdf-1-jhs-10.1177_17531934241232341 - Supplemental material for Incision techniques for trigger thumb release: a comparison of outcomes of four types of skin incision
Supplemental material, sj-pdf-1-jhs-10.1177_17531934241232341 for Incision techniques for trigger thumb release: a comparison of outcomes of four types of skin incision by Jaimy E. Koopman, Jeroen M. Smit, Robbert M. Wouters, Ruud W. Selles, J. Michiel Zuidam, Hand-Wrist Study Group Caroline A. Hundepool in Journal of Hand Surgery (European Volume)
Footnotes
Acknowledgements
The authors thank all patients who participated and allowed their data to be anonymously used for the present study. In addition, we acknowledge all caregivers and personnel of Xpert Clinics, Xpert Handtherapie and Equipe Zorgbedrijven for assisting in the routine outcome measurements that are the basis for this manuscript.
Hand-Wrist Study Group collaborators
Richard A. M. Blomme, MD, Jeronimus (Jeroen) M. Smit, MD, PhD, Kennard Harmsen, MD, Gertjan Halbesma, MD, Guus M. Vermeulen, MD, PhD, Johannes (Hans) P. de Schipper, MD, Jeroen H. van Uchelen, MD, PhD, Oliver T. Zöphel, MD, PhD, John S. Souer, MD, PhD, Lisa E. Lopez, PT, CHT-NL, Alexandra Fink, PT, CHT-NL, MSc, Rob van Huis, PT, CHT-NL, Pierre-Yves A. A. Pennehouat, PT, CHT-NL, Marietta Bertleff, MD, Karin Schoneveld, PT, CHT-NL, MSc, Grada D. Arends, PT, CHT-NL, Reinier Feitz, MD, PhD, Lisa Hoogendam, BSc, Steven E. R. Hovius, MD, PhD, Yara Eline van Kooij, PT, CHT-NL, MSc, Jaimy E. Koopman, MD, Mark J. W. van der Oest, MD, PhD, Willemijn A. de Ridder, PT, CHT-NL, MSc, Ruud W. Selles, PhD, Liz-Tipper Sikking, Harm P. Slijper, PhD, Marloes H. P. ter Stege, MSc, Joris S. Teunissen, PhD, Robbert M. Wouters, PhD, PT, CHT-NL, Nina L. Loos, BSc, Nienke H. A. Mendelaar, MD, Lyse van Wijk, BSc, Ward R. Bijlsma MD, PhD, Joost W. Colaris, MD, PhD, Liron Duraku, MD, PhD, Egberta Petronella, Adriana (Brigitte) van der Heijden, MD, PhD, Caroline A. Hundepool, MD, PhD, Jelle M. Zuidam, MD, PhD
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Ethical approval of this study was obtained from the Medical Ethics Review Committee of the Erasmus Medical Centre (MEC-2018-1088).
Informed consent
Written informed consent was obtained from all participants before the study.
Supplementary Material
Supplementary Table 1. Non-responder analysis comparing baseline characteristics of patients who did (responders) and did not (non-responders) complete the Michigan Hand Outcomes Questionnaire (MHQ) 3 months postoperatively. Significance testing was performed using independent sample t-tests, Wilcoxon tests and chi-square tests. Effect sizes for the differences were calculated using Cohen’s d and Cliff’s Delta. We found that non-responders were more often male (effect size 0.06).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.