
Abstract
This study describes mental health and psychosocial screening processes, access to care and interventions provided to children with upper limb musculoskeletal conditions. A cross-sectional e-survey study was conducted of 107 healthcare professionals who work with children with congenital hand and upper limb differences and brachial plexus birth injuries. Of them, 41 (38%) reported that they routinely screen for mental health and psychosocial concerns. Few (12%) reported the use of standardized outcome measures. In total, 51 (48%) healthcare professionals reported that there was a waiting list for mental health services at their institution. Collectively, healthcare professionals were unsatisfied with the staffing, access to care and types of interventions available. Reported barriers to care included the growing need for mental health support, lack of resources and poor continuity of care after referrals. Future research should focus on identifying and validating a mental health screening tool and investigating the processes affecting access to mental health care.
Keywords
Introduction
Children with congenital upper limb differences (CoULD) and brachial plexus birth injury (BPBI) have upper limb impairments that negatively affect their participation in personally and socially meaningful activities (Franzblau et al., 2015). Participation, defined as involvement in life situations (World Health Organization, 2001), is the main goal of care for these children (Lightdale-Miric et al., 2021). Participation not only involves physical health related to upper limb function, but also the developmental capacities, enjoyment and emotional well-being associated with engaging in activities (Coster and Khetani, 2008). The current care of these children with upper limb musculoskeletal (MSK) conditions focuses on physical rehabilitation and reconstructive surgery to improve function and appearance (Coroneos et al., 2017; Lightdale-Miric et al., 2021). Although interventions target physical function, evidence is cumulating that the intersection of physical and mental health affects patient healthcare experiences and outcomes (Purther et al., 2023).
Psychological and social factors may affect participation of children with upper limb MSK conditions. Although most participate in daily activities to the same degree as their peers (Ardon et al., 2012), they use compensatory strategies and/or adaptive aids (Franzblau et al., 2015). Learning to adapt may be challenging, time consuming and/or painful (Franzblau et al., 2015). These children may have lower self-confidence and competence when participating in activities that are physically demanding (e.g. sports and athletics) and avoid challenging activities that require both limbs (Strombeck and Fernell, 2003).
Stigma affecting peer acceptance and relatedness with others may also negatively affect their participation (Carlsson et al., 2018). These social aspects of participation may also lead to worry, anxiety and depression related to limb function and appearance, as well as stress related to decisions regarding upper limb surgery (McDougall et al., 2021). In addition, parental stress, family conflict and poor family functioning have been shown to negatively influence psychological adjustment in children with upper limb MSK conditions (Alyanak et al., 2013).
Programmes focused on fostering psychosocial functioning for children with upper limb MSK conditions and their families exist; however, knowledge of and access to these supports are limited. Camps and family education days are examples of programmes designed to facilitate mutual aid in these children and their families (Ho and Ulster, 2011; Lake, 2010). The therapeutic value of these programmes in improving youth self-esteem and peer relationships has been shown. (Ho and Ulster, 2011; Lake et al., 2021) However, it is unclear if those who are at greatest risk of poor mental health attend such programmes. Coordinated efforts are needed to determine the mental health burden and needs of children with upper limb MSK conditions. The aim of the present study was to describe the screening processes, access to care, and effectiveness of mental health and psychosocial interventions provided to children with upper limb MSK conditions and their families from the perspective of healthcare professionals who provide specialized care in paediatric hand and upper limb programmes.
Methods
Using qualitative and quantitative approaches, a cross-sectional study was conducted to survey healthcare professionals regarding mental health and psychosocial screening processes, access to care, resources and interventions provided to children with upper limb MSK conditions at paediatric hand and upper limb centres worldwide.
Multidisciplinary healthcare professionals who work clinically with children (0–18 years) with a diagnosis of CoULD or BPBI were surveyed. Participant lists generated from international consortiums (e.g. Pediatric Hand Study Group, International Plexus Outcome Study Group: iPLUTO) were compiled and healthcare professionals were contacted via email by the senior author (ESH) on 1 June 2021 with the e-survey (Supplementary file 1). An informed consent statement was provided on the first page, and implied consent was obtained at the start of the survey. The e-survey was re-sent on 29 June and closed on 14 July 2021.
The survey (Appendix 1) was developed with closed- and open-ended questions by the senior author (ESH) with feedback from the multidisciplinary team in the Hospital for Sick Children’s hand and upper limb clinic, one parent partner and one youth partner (Manafo et al., 2018). The response scale for the closed-ended questions was a visual analogue scale (VAS) of 0–100 (100 = strongly agree). The open-ended questions allowed participants to describe the types of mental health and psychosocial supports and interventions that are being provided, as well as how these supports are presently used in their respective contexts. Participant demographic information related to profession, country of practice and types of upper limb MSK conditions seen in practice were also collected in the survey. The secure REDCap® survey platform was used to anonymously collect survey data.
The anchored VAS survey responses were analysed descriptively using SPSS Statistics (version 28.0.1.1; IBM Corp., Armonk, NY, USA). After conducting the Shapiro–Wilk test of normality of the data, Mann–Whitney U-test scores were used to conduct a post-hoc test to determine if there was a difference between the survey responses of physicians and allied health professionals regarding the participants’ satisfaction with staffing, accessibility of these services, type of resources available and the perceived effectiveness of available resources. Benjamini–Hochberg adjustment for the multiple comparisons was applied to adjust the significance level (α = 0.05) (Lee and Lee, 2018).
A thematic analysis was conducted on the open-ended survey comments following Braun and Clarke’s reflexive approach (Braun and Clarke, 2006). All data were read iteratively to achieve immersion and enhance overall understanding of the data as a whole before inductive coding by two independent researchers (DP, TH) to capture key concepts or thoughts using conventional content analysis (Hsieh and Shannon, 2005). This initial analysis formed a basis for researchers to collaborate, combine and compare initial codes to be merged into meaningful themes. Qualitative findings were then discussed with the senior author (ESH) and the themes were organized into a tree diagram to present these data visually.
Results
Of the 307 healthcare professionals invited to participate, 109 (36%) completed the e-survey between 1 June and 14 July 2021. Two participants were excluded from the study due to the non-clinical nature of their roles. There were 47 (44%) physicians and 60 (56%) allied health professionals surveyed (Table 1). Participants represented 15 countries across five continents, predominantly from North America (70%), Europe (20%) and Australia (8%).
Participant demographics.
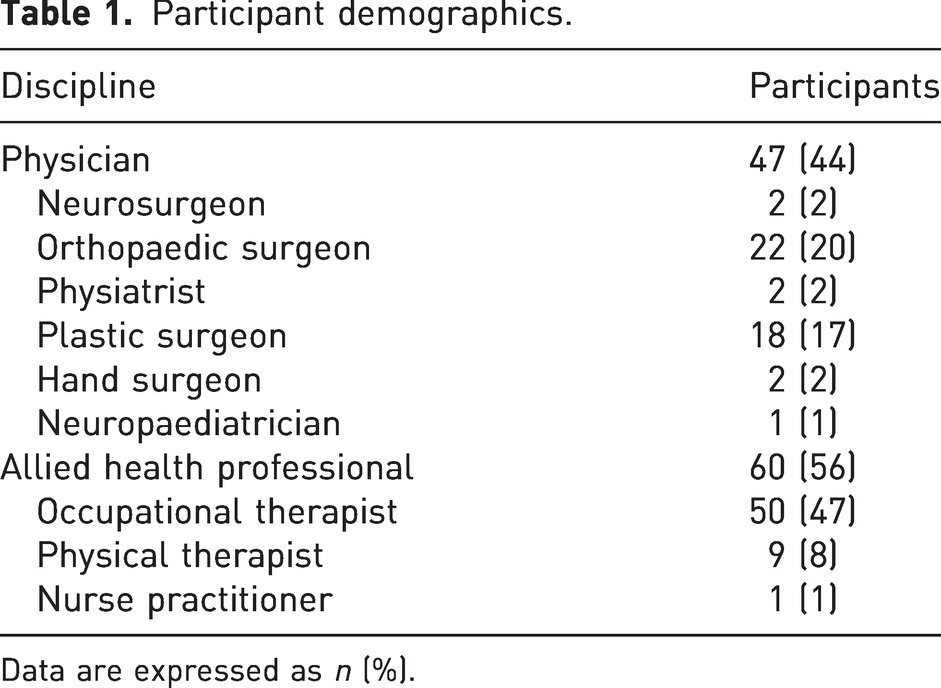
Data are expressed as n (%).
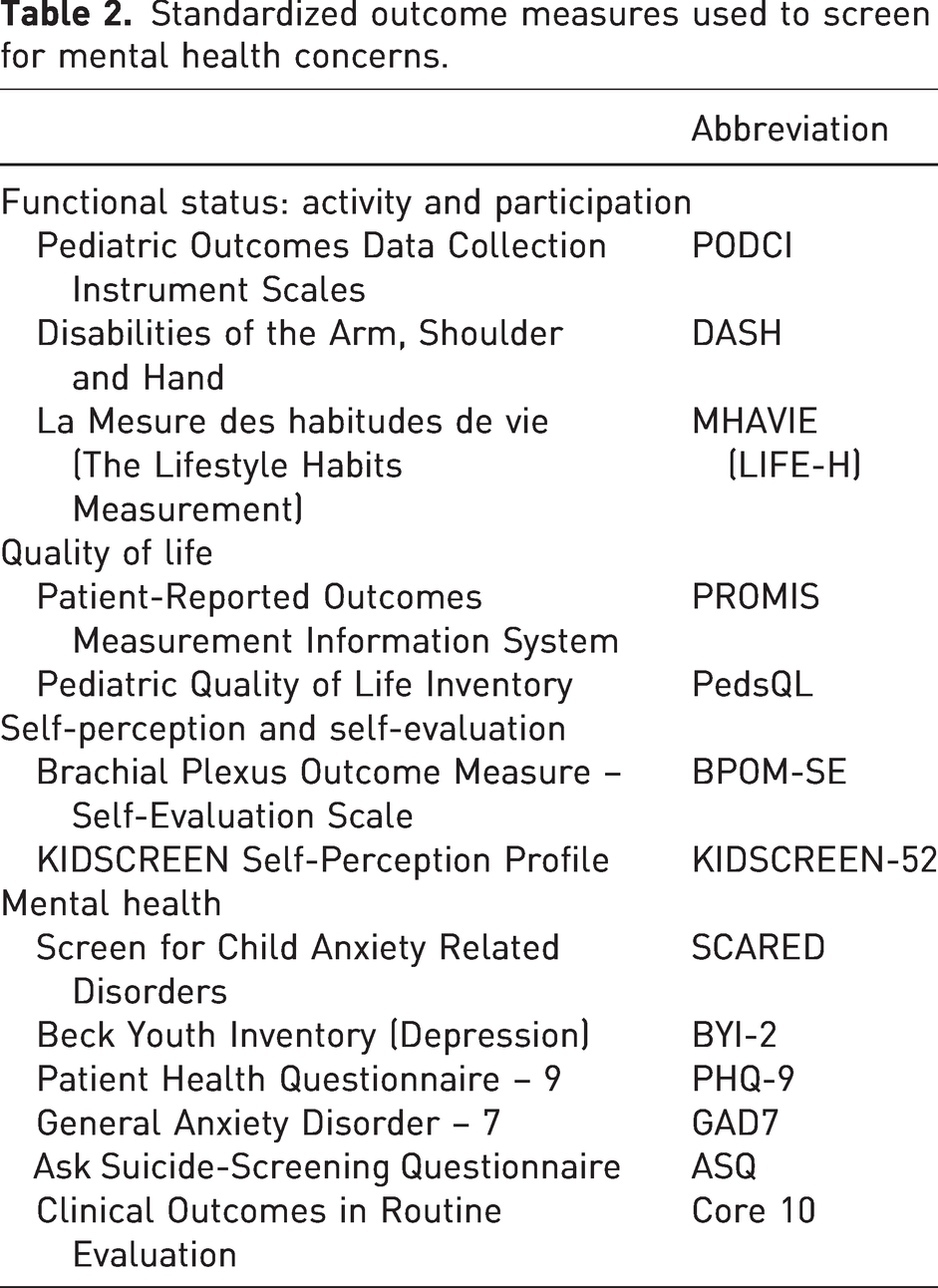
Of the 107 participants who completed the survey, 41 (38%) reported that they routinely screen for mental health and psychosocial concerns in children and adolescents with upper limb MSK conditions. Of the predominant continents represented, the percentage of respondents who routinely screen for mental health concerns were as follows: North America (43%); Europe (18%); and Australia (50%). Of the participants, 13 (12%) used standardized outcome measures to screen for mental health and psychosocial concerns. The reported measures used by these respondents are organized into four categories of patient-reported outcome measures in Table 2: functional status; quality of life; self-perception/self-evaluation; and mental health. All measures were reported once except the Pediatric Outcomes Data Collection Instrument (PODCI), Patient-Reported Outcome Measurement Instrument System (PROMIS) and the Brachial Plexus Outcome Measure (BPOM). As survey respondents were able to report more than one tool, it was noted that four of the mental health measures were provided by one participant.
Standardized outcome measures used to screen for mental health concerns.
The primary staffing resources to support mental health and psychosocial concerns were social workers and occupational therapists (Table 3). Personnel listed under ‘other’ included physical therapists, behavioural medicine, child life and pain specialists. Most respondents (66%) reported that mental health and psychosocial staffing resources were available by consultation only. The five who responded ‘other’ commented that full-time equivalency (FTE) data were difficult to report or unknown. Of the participants, 51 (49%) reported a waiting list for mental health services at their institution. Most indicated that the length of waiting time for services was less than 6 months (Table 3); however, one-third of participants were unsure of the waiting time for services or that the timing of service provision was dependent on needs, insurance and location. The types of mental health and psychosocial interventions provided at the institutions represented by respondents are also shown in Table 3. In-person medical education during clinic visits, parent-to-parent connections and social work were the more commonly offered interventions.
Mental health and psychosocial support resources.
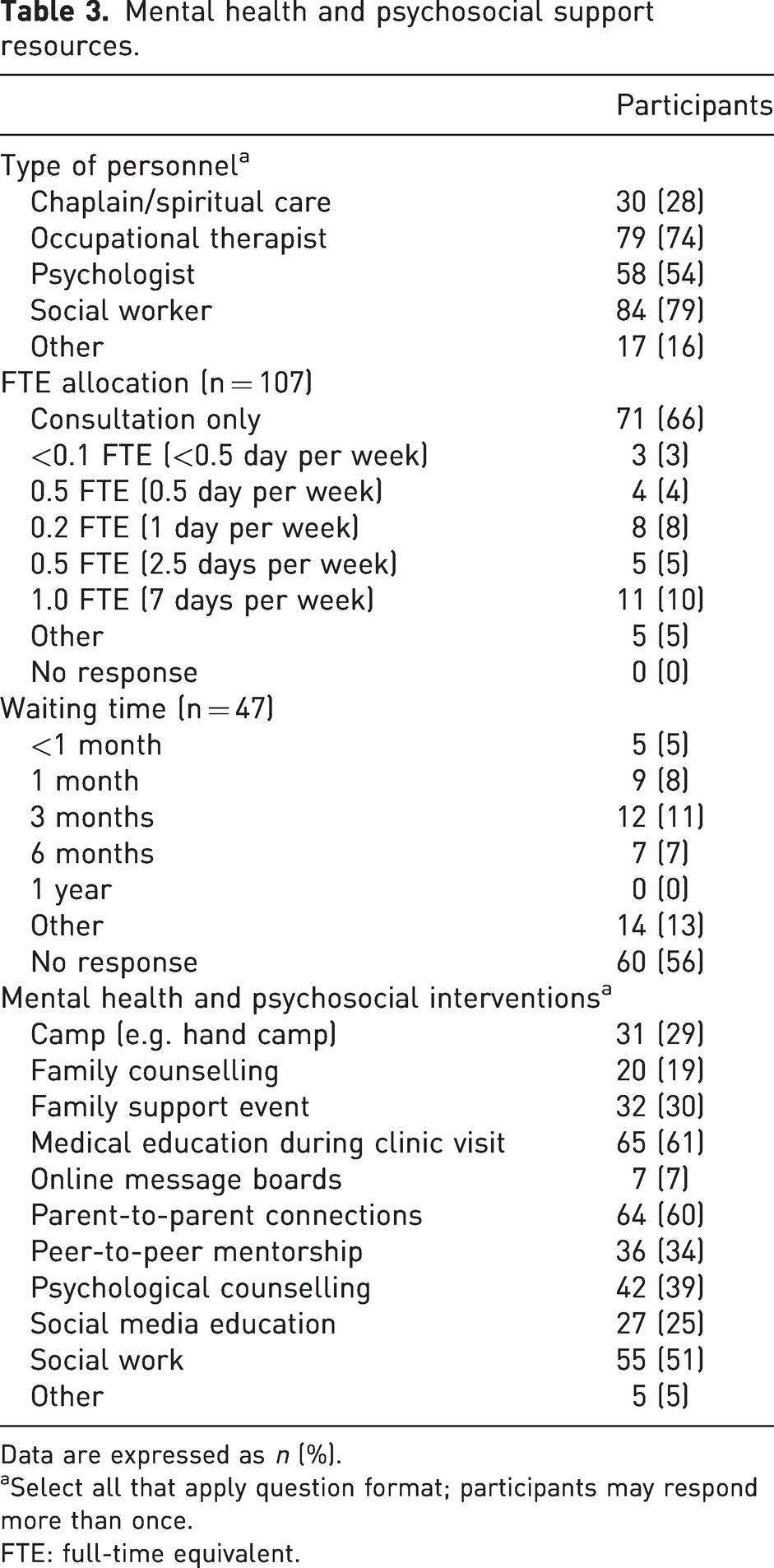
Data are expressed as n (%).
Select all that apply question format; participants may respond more than once.
FTE: full-time equivalent.
Collectively, healthcare professionals reported low satisfaction with staffing, access to care, and type of resources available to support mental health and psychosocial support in children with upper limb MSK conditions (median, range 30.0–32.5) (Table 4). In observing the large variance in these data, a post-hoc analysis was performed to determine whether there was a difference in the scores between physicians (n = 45) and allied health professionals (n = 59). Physicians had significantly higher satisfaction with the effectiveness of current interventions than allied health professionals (Table 4).
Comparison of physician versus allied health responses.
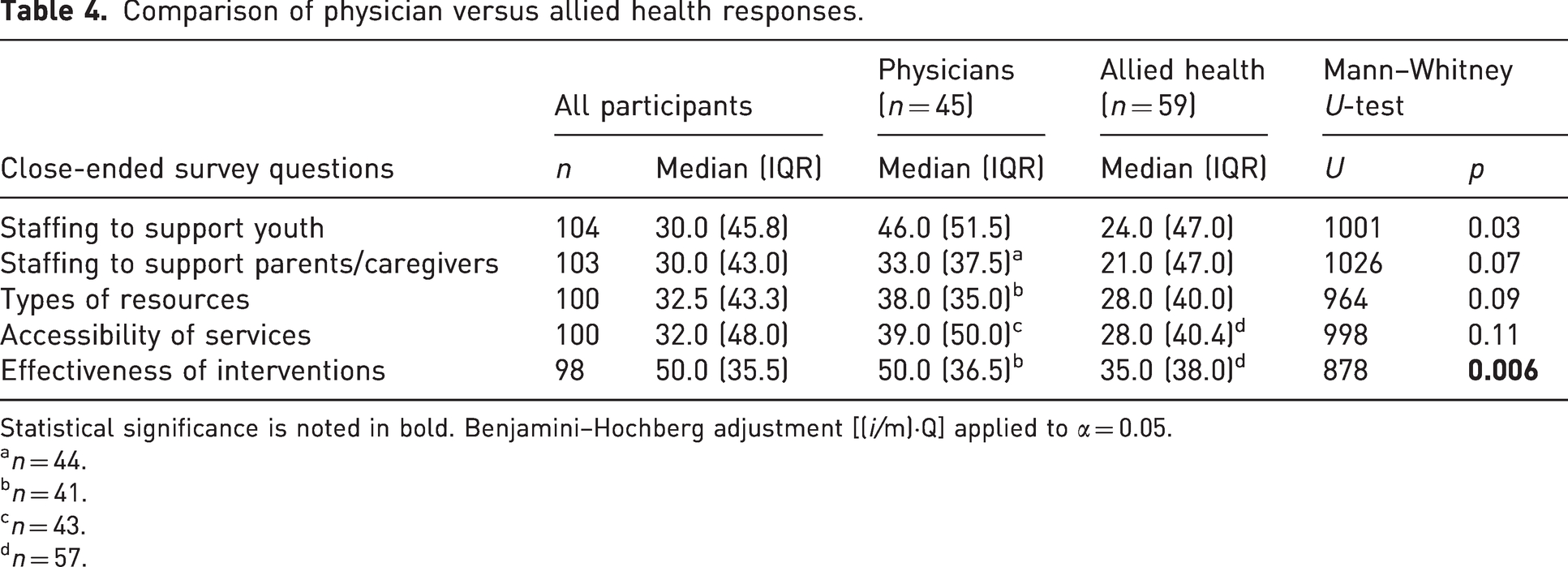
Statistical significance is noted in bold. Benjamini–Hochberg adjustment [(i/m)·Q] applied to α = 0.05.
n = 44.
n = 41.
n = 43.
n = 57.
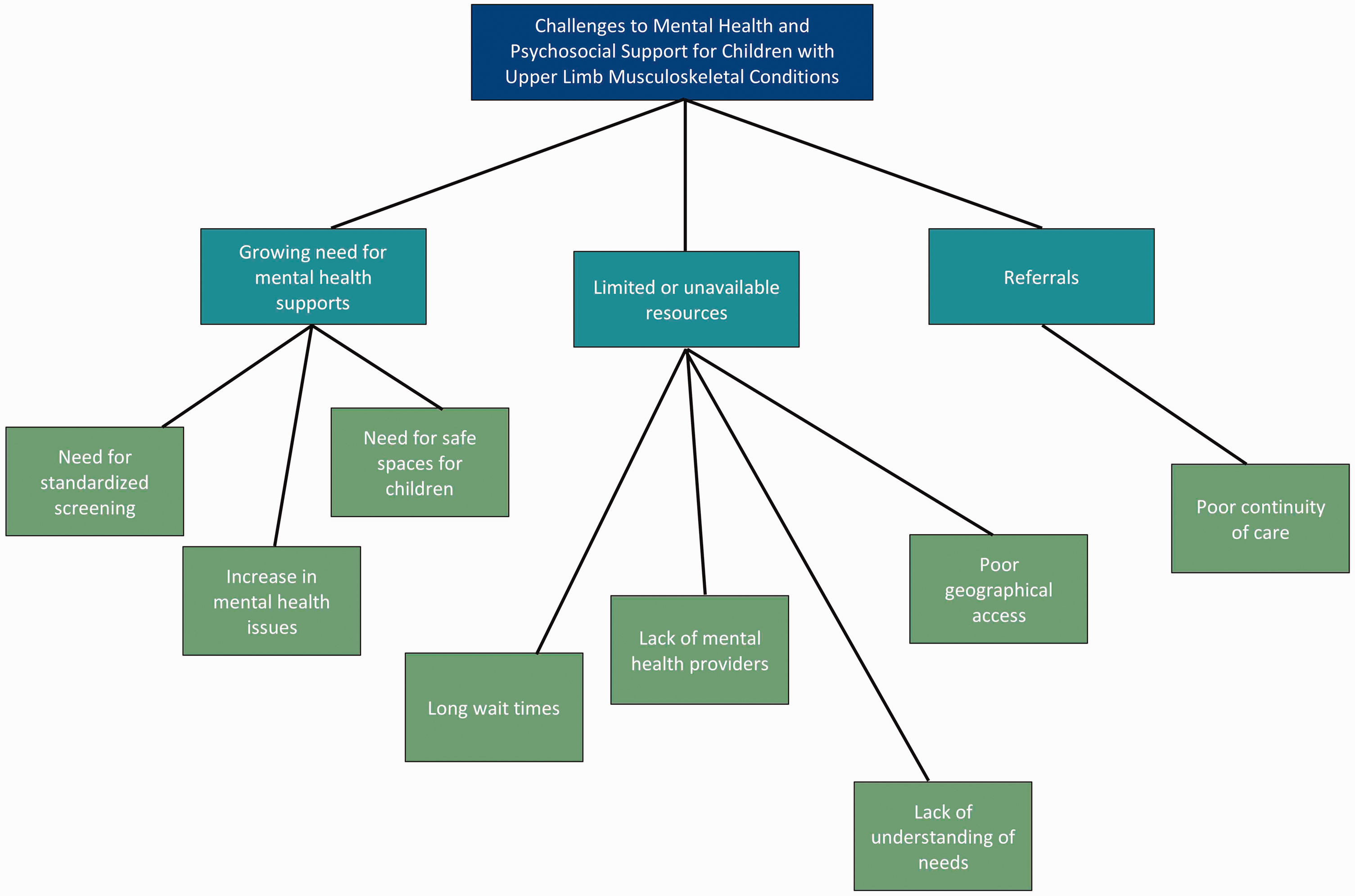
A total of 63 open-ended survey comments were gathered from 50 participants (14 physicians, 36 allied health professionals). A thematic analysis of these data identified three challenges associated with access to and availability of mental health and psychosocial supports for children with upper limb MSK conditions (Figure 1):
Qualitative themes.
Growing need for mental health supports: Participants indicated that there is a growing unmet demand for mental health and psychosocial supports. However, there is currently no standard method of screening for mental health and psychosocial concerns. Some described a lack of opportunities provided for children and families to express their thoughts and feelings. One participant wrote ‘we do not create the brave spaces needed for children to express their worries, negative feelings or disappointment’.
Limited or unavailable resources: Participants highlighted the challenges associated with limited or unavailable mental health and psychosocial support, including staff shortages, long waiting times and limited time available in clinic. Financial concerns also pose a challenge, as these services are often privately funded, which is not always feasible for the families of these children. One participant emphasized this as they described ‘there is a dramatic lack of access to mental health resources in the community especially for those who are uninsured’.
Poor continuity of care after referrals: Influenced by available resources, the overall coordination of care between the healthcare professionals in the hand and upper limb clinic and those providing mental healthcare appears limited. Several participants highlighted the role of the occupational therapist in providing a holistic approach to the children’s care, identifying interpersonal and psychosocial support, although the limited ability to provide mental health services in this role was noted. After mental health concerns are identified, children and families are often ‘referred out’ in the community, seen by ‘another department’ for mental health services, or receive peer-to-peer supports coordinated through community organizations or individual arrangements.
Discussion
The present study explored mental health and psychosocial screening practices, resources, access to care and interventions for children with upper limb MSK conditions and their families. The findings from the healthcare professionals surveyed found that only 38% of children were screened by attending clinicians for mental health and psychosocial concerns. The use of a common standardized tool designed to screen for mental health risks was not found. A qualitative analysis of open-ended text from participants indicates challenges with care processes that affect access to resources and care for mental health and psychosocial support.
The lack of routine screening among healthcare professionals in this study who work at specialized paediatric hand and upper limb clinics is not surprising as the primary point of care for these children follows a biomedical diagnosis-driven model (Wade and Halligan, 2017). These ambulatory surgical clinics involve multidisciplinary teams that specialize in care of the physical sequelae of these children. The use of functional status and quality of life measures is prioritized. Subsequently, the mental well-being component of these measures can be used to screen for the psychosocial and psychological adjustment of their patients. In this study, a standardized mental health screening tool specific to children with upper limb MSK conditions was not identified. Generic mental health measures were identified that have been validated on surgical patients (Papadopulos et al., 2015); however, further research is needed to explore their use with children with upper limb MSK conditions and the feasibility of implementing these tools in specialized hand and upper limb clinics.
This study found a difference between physicians and allied health professionals with respect to the perceived effectiveness of mental health and psychosocial interventions. These findings may have been influenced by differing perspectives on the definition of mental health. Some healthcare professionals may equate the presence or absence of mental disorder as the basis of mental health, while others may see mental health as a continua of mental health and disorder (Keyes, 2010). As such, a participant’s satisfaction with mental healthcare and effectiveness of available interventions may be influenced by their mental health framework. Another consideration is that programme-level expectations may influence healthcare professionals’ perceptions of what services should be offered (Nilsen, 2015). Some may feel that mental healthcare is best screened and managed by external care partners. Overall, these findings illustrate that further research is needed to investigate multidisciplinary healthcare professionals’ practice beliefs and behaviours related to mental health and psychosocial service delivery for children with upper limb MSK conditions.
The findings from this study are beneficial in understanding mental health services in paediatric hand and upper limb clinics; however, there are some limitations. We aimed to use a broad recruitment strategy involving international healthcare professionals to increase the potential pool of participants. This approach may have lowered our response rate. Our response rate of 36% is reflective of present trends in email survey response rates; however, a targeted multi-mode approach (e.g. multiple and personalized contact) of a smaller participant pool may have been more strategic (Sheehan, 2001). In addition, many participants in this study were from Canada and the United States, which indicates that these findings represent a predominantly a North American perspective. As shown by the descriptive difference in mental health and psychosocial support screening practices in Europe, further research is needed to compare international perspectives. Lastly, data regarding the institution in which participating healthcare professionals practice were not collected; therefore, it is unclear if physicians and allied health professionals from the same institutions completed the survey.
Children with upper limb MSK conditions may have mental health and psychosocial concerns that may not be identified due to the lack of screening and access to mental health and psychosocial support resources. Future research is needed to validate a mental health screening tool for this population and investigate healthcare delivery beliefs and practices among multidisciplinary healthcare professionals regarding supporting mental health and psychosocial needs of these children and families.
Supplemental Material
sj-pdf-1-jhs-10.1177_17531934231214138 - Supplemental material for Mental health and psychosocial support for children with upper limb musculoskeletal conditions
Supplemental material, sj-pdf-1-jhs-10.1177_17531934231214138 for Mental health and psychosocial support for children with upper limb musculoskeletal conditions by Deanna Persaud, Tamsen Hutchison, Samantha J. Anthony, Kristen M. Davidge, Howard M. Clarke and Emily S. Ho in Journal of Hand Surgery (European Volume)
Footnotes
Acknowledgements
The authors would like to thank Diba Vahidi Ferdosi for her contributions in coordinating and managing the survey data for this study. Part of this study was presented at the International Federations of Societies of Surgery of the Hand and International Federations of Societies of Hand Therapists Conference in June 2022 and the American Society of Hand Therapists Annual Meeting in October 2022.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was partially funded by the University of Toronto Departments of Family and Community Medicine, Rehabilitation Sciences, and Psychiatry Cass Family Grants for Catalyzing Access and Change.
Ethical approval
Approval from the Research Ethics Board was obtained from the Hospital for Sick Children (REB No. 1000075069) and the University of Toronto (No. 41063). All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2008 (5).
Informed consent
Informed consent was obtained from all participants for being included in the study.
Supplementary file 1
Appendix – Survey
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.