
Abstract
This systematic review analysed the available evidence on the clinical outcomes of total wrist arthroplasty (TWA) in patients with inflammatory and non-inflammatory arthritis. After screening, 12 studies met the inclusion criteria. They involved 359 patients with 378 TWA implants. The results showed that TWA significantly improved Disabilities of the Arm, Shoulder and Hand (DASH)/Quick-DASH scores and pain visual analogue scale scores in both arthritis groups compared with preoperative values. However, there was no statistically significant difference in the outcome scores between the two groups. Three studies reported Patient-Rated Wrist Evaluation (PRWE) scores, and TWA significantly improved PRWE scores in non-inflammatory arthritis but not in inflammatory arthritis, with no significant difference in postoperative outcome scores between the two groups. Although the included studies have limitations, the review suggests that TWA may be a successful treatment for wrist pain in individuals with either inflammatory or non-inflammatory arthritis. However, further high-quality trials are needed to confirm these findings.
Introduction
Total wrist arthroplasty (TWA) has gained popularity as a motion-preserving option for treating wrist pain caused by arthritis. Implants have evolved, but unlike the hip or knee, TWA still lags behind arthrodesis as a first-line treatment (Halim and Weiss, 2017; Melamed et al., 2016).
Classically, the most appropriate candidates for wrist arthroplasty have been those with lower functional demands (Adams, 2013). Older patients with rheumatoid arthritis have therefore been the most common recipients, accounting for 51%–71% of all patients undergoing TWA (Boeckstyns, 2014; Melamed et al., 2016). However, as the use of TWA has grown, so has the breadth of indications, including primary and post-traumatic arthritis, where bone stock and soft tissue preservation are often better. However, the age of these patients may be lower and their functional demands higher, which raises questions about the survivorship of these implants.
While the indications have broadened, which blurs the lines between the types of arthritis considered appropriate, the evidence has remained sparse with no clear consensus to guide decision-making in clinical practice. The aim of the present study was to review the evidence that considers the clinical outcomes of TWA, with a particular focus on comparisons between inflammatory and non-inflammatory arthritis.
Methods
This systematic review was conducted and reported in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analysis statement (Online Table S1) (Page et al., 2021).
Search strategy
The search strategy is detailed in online Appendix S1. MEDLINE, EMBASE, Cochrane Central Register of Controlled Trials (CENTRAL) and Cumulative Index to Nursing and Allied Health Literature were searched from their inception up to October 2022. Relevant studies from the reference lists of identified studies and previous systematic reviews were also considered for inclusion.
Selection of studies
Four authors (HHC, AA, MZ and KB) independently screened paper titles and abstracts for inclusion. Initial screening was based on title and abstract review, followed by full-text review. Disagreements were adjudicated by the senior author (KK).
Eligibility criteria
We included randomized controlled trials (RCTs), non-randomized controlled trials, prospective cohort studies and retrospective case series, with five patients or more, and either published in English or with an appropriate English translation available. The inclusion criteria were as follows:
Population: adult patients (age ≥18 years) after TWA Indications: stratified by arthritis aetiology into: Inflammatory arthritis (including rheumatoid and psoriatic), and Non-inflammatory arthritis (including primary osteoarthritis, post-traumatic, scaphoid nonunion advanced collapse, scapholunate advanced collapse, Kienböck’s disease) Comparison: preoperative patient-reported outcome measures (PROM) score Primary outcome: PROMs, including Disabilities of the Arm, Shoulder and Hand (DASH) or Quick-DASH and Patient-Rated Wrist Evaluation (PRWE) scores Secondary outcomes: pain visual analogue scale (VAS), grip strength (in kg), survival (revision rate)
To allow data pooling, the included studies had to report either a mean or a change from baseline (mean difference) and standard deviation (SD) (Higgins et al., 2022). For studies that did not directly report SD, the SD in each comparison arm was calculated from standard errors, confidence intervals (CI), t-statistics and p-values for differences in means using the Cochrane Handbook Calculation (Higgins et al., 2022).
Data extraction
Data were extracted from the included studies and collated in a standardized data extraction database. The data extracted included study characteristics, aetiology of arthritis (inflammatory vs. non-inflammatory), type of implant, outcome of interest and duration of follow-up.
Risk of bias assessment
Two authors (AA and MZ) independently assessed the risk of bias (ROB) of each included study using the Cochrane Risk of Bias Tool 1.0 (ROBINS-1). Disagreements were resolved by consensus through discussion with a third author (HHC). Seven study quality domains were considered: bias due to confounding; selection of participants into the study; classification of interventions; departures from the intended intervention; missing data; measurement of outcomes; and selection of the reported outcome. The results were presented as both traffic light plots and summary plots using the robvis online tool (McGuinness and Higgins, 2021).
Statistical analysis
Age and duration of follow-up were reported either as means (SD; range) or as median (range) in accordance with the original article. Network plots were formulated to show the relationship between interventions. Direct and indirect comparisons between interventions were combined using a frequentist network meta-analysis (NMA) via a random effects model. The mean difference (MD) with a 95% CI was used to present estimates from the frequentist NMA for continuous data, while an odds ratio (OR) with a 95% CI was used for binary data. The CIs were evaluated for both direct and indirect comparisons, with values including zero (e.g. –1 to 1), indicating no significant difference between means, and CIs including 1 (e.g. 0.5 to 1.5), indicating no significant difference for binary data.
Results
The search yielded 1858 results. After screening and full-text review, 12 studies met the inclusion criteria (Figure 1) (Badge et al., 2016; Boeckstyns et al., 2013; Brinkhorst et al., 2018; Ferreres et al., 2011; Harlingen et al., 2011; Holm-Glad et al., 2022; Holzbauer et al., 2022; Honecker et al., 2019; Matsui et al., 2020; Reigstad et al., 2012, 2017; Rossello et al., 2022). Reigstad et al. (2012, 2017) presented their initial results in 2012, followed by a follow-up report in 2017; only data from the 2017 analysis were included in our analysis. A total of 359 patients (sample size range 5–75) with 378 TWA implants were included. The aetiology was inflammatory arthritis in 173 patients and non-inflammatory in the remainder. Table 1 summarizes the characteristics of the included studies.
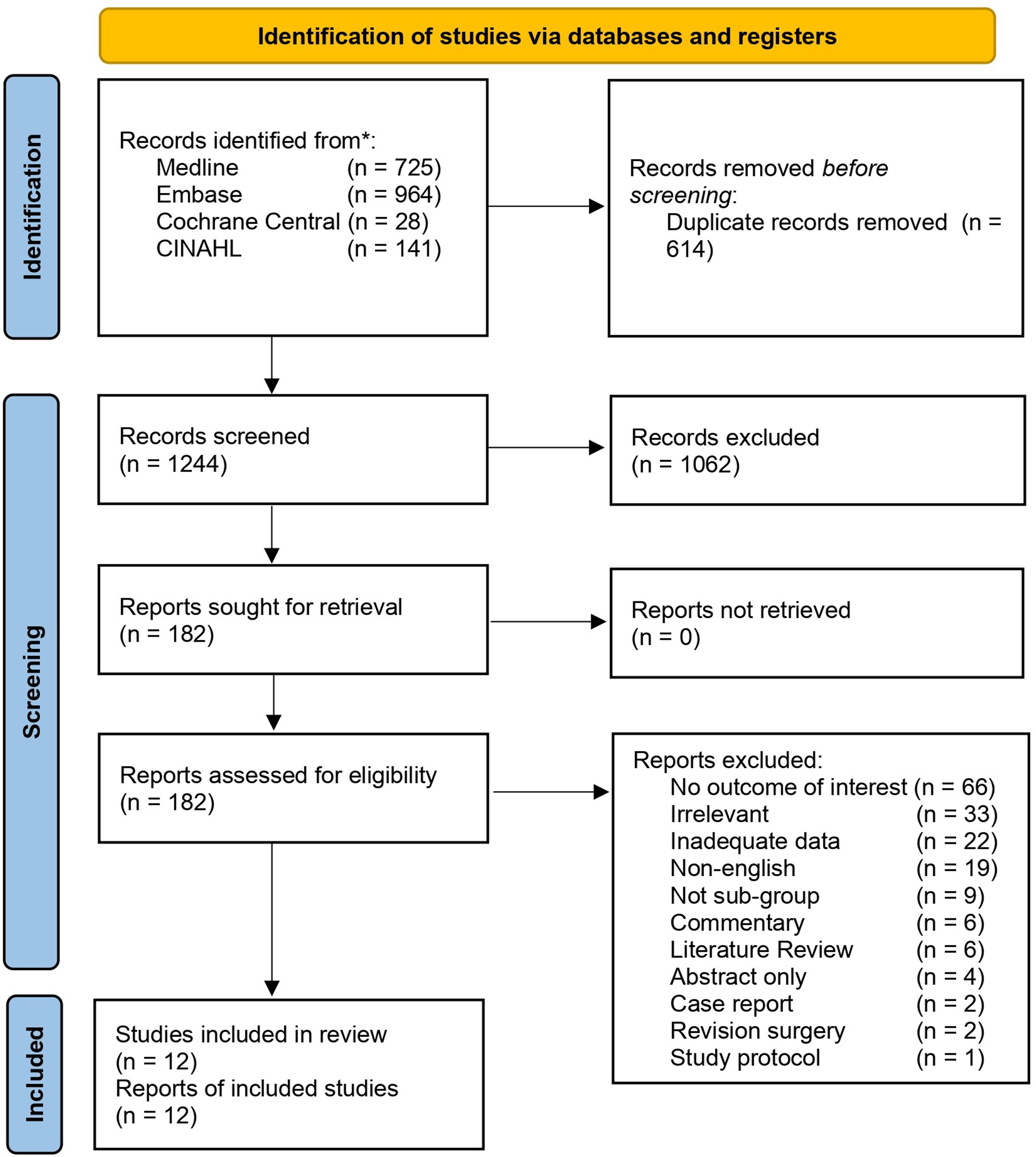
PRISMA flow chart.
Characteristics of studies.
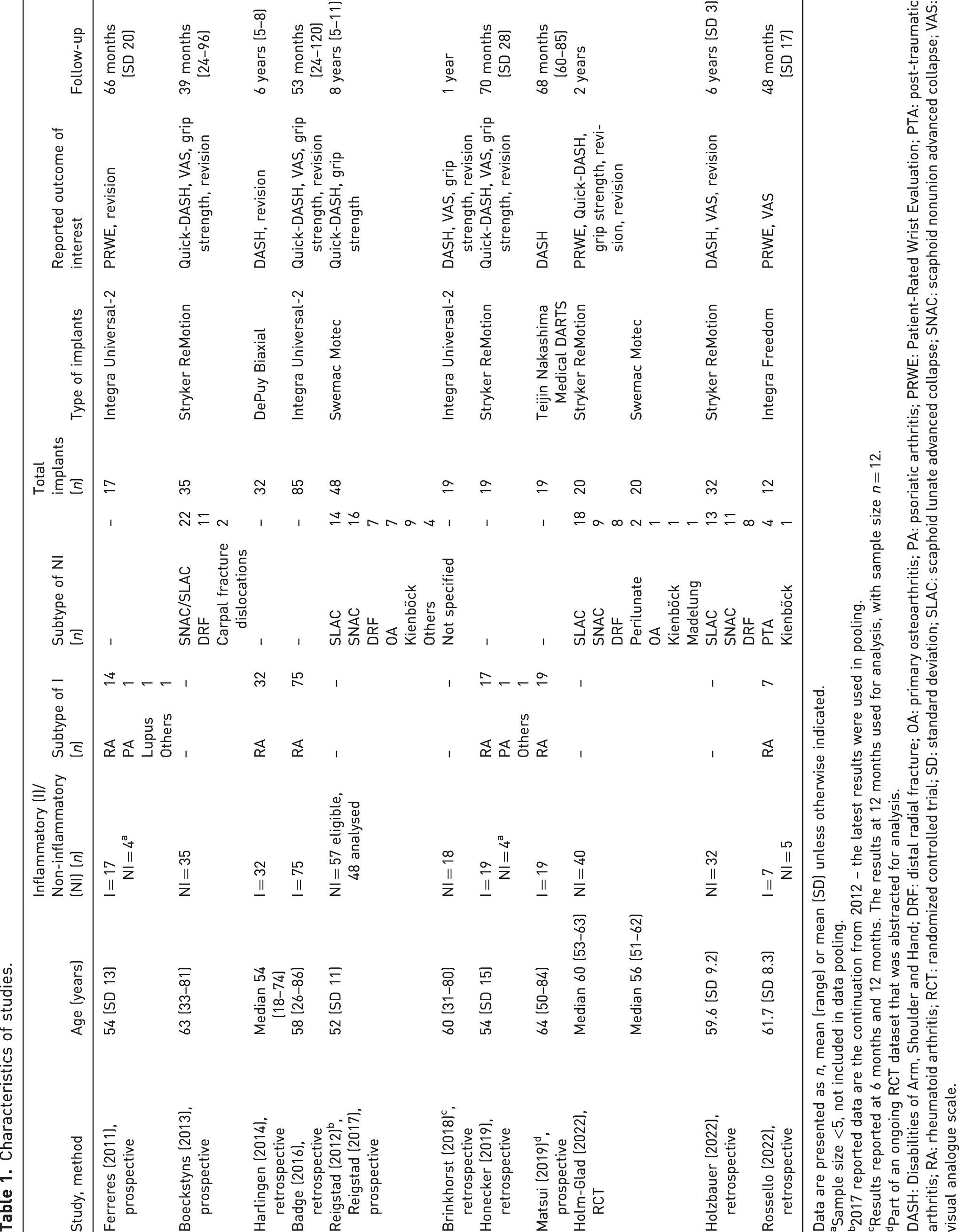
Data are presented as n, mean (range) or mean (SD) unless otherwise indicated.
Sample size <5, not included in data pooling.
2017 reported data are the continuation from 2012 – the latest results were used in pooling.
Results reported at 6 months and 12 months. The results at 12 months used for analysis, with sample size n = 12.
Part of an ongoing RCT dataset that was abstracted for analysis.
DASH: Disabilities of Arm, Shoulder and Hand; DRF: distal radial fracture; OA: primary osteoarthritis; PA: psoriatic arthritis; PRWE: Patient-Rated Wrist Evaluation; PTA: post-traumatic arthritis; RA: rheumatoid arthritis; RCT: randomized controlled trial; SD: standard deviation; SLAC: scaphoid lunate advanced collapse; SNAC: scaphoid nonunion advanced collapse; VAS: visual analogue scale.
ROB analysis
Online Figure S1 show the ROB scores for the included studies. There were five prospective studies, six retrospective studies and one RCT (note that the series by Holm-Glad et al. (2022) was an RCT, but the comparison arms were two different TWA implants; therefore, this was included and analysed as a prospective study using ROBINS-1). Overall, one study was classified as serious ROB, six as moderate ROB and five as low ROB.
DASH or Quick-DASH
In total, 10 studies reported DASH or Quick-DASH scores (Badge et al., 2016; Boeckstyns et al., 2013; Brinkhorst et al., 2018; Harlingen et al., 2011; Holm-Glad et al., 2022; Holzbauer et al., 2022; Honecker et al., 2019; Matsui et al., 2020; Reigstad et al., 2012, 2017). TWA was found to significantly improve DASH or Quick-DASH scores for both indications compared to preoperative baselines. However, when comparing the outcomes postoperatively between inflammatory and non-inflammatory arthritis, there was no statistically significant difference in the indirect comparison of the outcome scores (MD: –0.09, 95% CI: –10.30 to 10.11).
We performed a sensitivity analysis excluding Harlingen et al. (2011) due to the discontinuation of the use of biaxial total wrist prosthesis. The results of the sensitivity analysis were consistent with those of the primary analysis, showing similar effect estimates and confidence intervals for both inflammatory and non-inflammatory arthritis (MD: –3.29, 95% CI: –12.82 to 6.24).
PRWE
Three studies reported PRWE scores (Ferreres et al., 2011; Holm-Glad et al., 2022; Rossello et al., 2022). TWA was found to significantly improve PRWE scores in non-inflammatory arthritis (MD: –47.60, 95% CI: –88.12 to –7.08) but not in inflammatory arthritis (MD: –31.64, 95% CI: –81.05 to 17.77). However, this finding should be interpreted with caution due to the limited number of studies included in this analysis. In the indirect comparison between inflammatory and non-inflammatory arthritis, there was no statistically significant difference in postoperative outcome scores (MD: –15.96, 95% CI: –79.86 to 47.94).
Pain VAS scale
Six studies reported pain outcomes using the VAS scale (Badge et al., 2016; Boeckstyns et al., 2013; Brinkhorst et al., 2018; Holzbauer et al., 2022; Honecker et al., 2019; Rossello et al., 2022). TWA resulted in a statistically significant improvement in pain VAS scores compared to preoperative baseline in both indications. The indirect comparison between inflammatory and non-inflammatory arthritis showed no statistically significant difference in postoperative pain outcomes (MD: –0.97, 95% CI: –4.45 to 2.50).
Grip strength
Seven studies reported grip strength results (Badge et al., 2016; Boeckstyns et al., 2013; Brinkhorst et al., 2018; Holm-Glad et al., 2022; Honecker et al., 2019; Reigstad et al., 2012, 2017). TWA resulted in a significant improvement in grip strength for patients with both inflammatory and non-inflammatory arthritis compared to preoperative levels. However, the comparison between these two groups did not show a significant difference in postoperative grip strength, with an MD of 2.51 and 95% CIs in the range of –0.22 to 5.25.
Revision rate
In total, 10 studies reported all cases of revision until final follow-up (Badge et al., 2016; Boeckstyns et al., 2013; Brinkhorst et al., 2018; Ferreres et al., 2011; Harlingen et al., 2011; Holm-Glad et al., 2022; Holzbauer et al., 2022; Honecker et al., 2019; Reigstad et al., 2012, 2017). Out of a total of 338 TWA procedures, 34 (10%) were revised after periods of 10 months to 6 years. The reported indications for revision were implant failure (n = 21/34), infection (n = 3/34), inflammation (n = 5/34) and stiffness/pain (n = 5/34). When comparing inflammatory arthritis with non-inflammatory arthritis, there was no significant difference in the odds of revision (OR: 0.54, 95% CI: 0.06 to 4.74).
We conducted a sensitivity analysis by excluding Harlingen et al. (2011). The results of the sensitivity analysis were consistent with those of the primary analysis, showing similar ORs and CIs for both inflammatory and non-inflammatory arthritis (OR: 0.62, 95% CI: 0.05 to 7.41). Table 2 summarizes the results of direct and indirect comparisons according to indications.
Summarized results of direct and indirect comparisons according to indications.
CI: confidence interval; DASH: Disabilities of Arm, Shoulder and Hand; I: inflammatory arthritis; NI: non-inflammatory arthritis; MD: mean difference; OR: odds ratio; PRWE: Patient-Rated Wrist Evaluation; VAS: visual analogue scale.
Complications
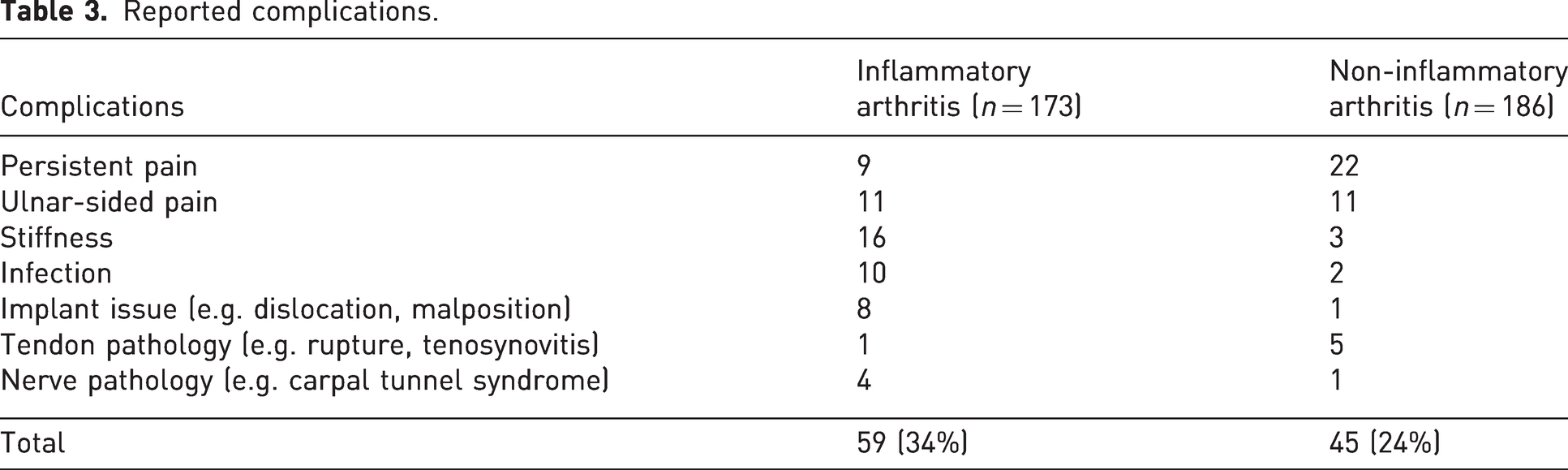
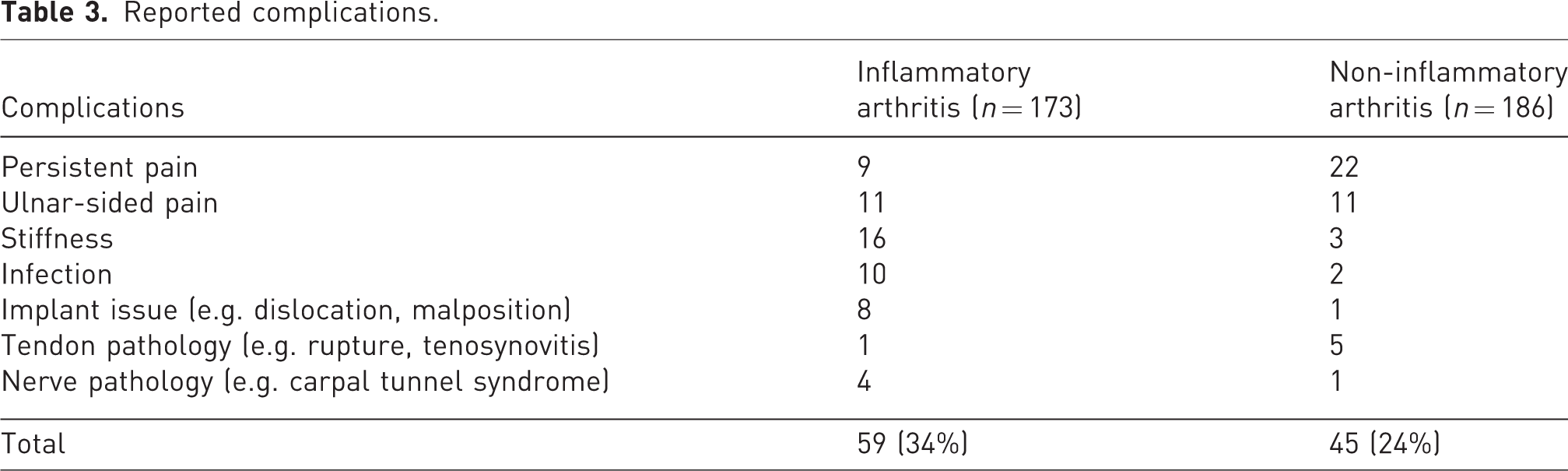
Table 3 displays the complications reported by all the included studies. Patients with inflammatory arthritis were more likely to experience stiffness, infection and implant-related problems. Conversely, patients with non-inflammatory arthritis were more likely to experience persistent wrist pain.
Reported complications.
Discussion
Early generations of TWA prostheses were associated with notable complications and poor survival, with first-generation implants, such as the Universal one, having a mean 10-year survival rate of 40% (Boeckstyns, 2014). As implant technology continues to evolve, the latest fourth-generation implants – including Universal-2/Freedom (Integra, Plainsboro, NJ, USA), Maestro (Biomet, Warsaw, IN, USA), Motec (Swemac Orthopaedics AB, Linköping, Sweden) and ReMotion (Small Bone Innovation, Morristown, PA, USA) – have been designed to improve outcomes. Motec, for example, has demonstrated a mean survival of 86% at 10 years, although this is still some distance from the >95% 10-year survival of hip and knee arthroplasty (Bayliss et al., 2017).
Other systematic reviews have presented overall complication and implant survival rates, without identifying the optimal indications to guide which patients will benefit most from TWA – in particular, whether TWA is equally effective in patients with inflammatory and non-inflammatory arthritis (Zijlker et al., 2022). We found no significant differences in PROMs, pain scores, grip strength and revision rates after TWA between patients with inflammatory and non-inflammatory arthritis. These findings challenge the prevailing dogma that only certain cohorts of patients can benefit from TWA.
A limitation of this study was the variable quality of the underlying evidence, with most studies having a moderate ROB. As a result, some studies had to be excluded due to the poor quality or quantity of reporting. This included one large study comparing inflammatory and non-inflammatory indications, although their findings were consistent with ours (Herzberg et al., 2012). There was also heterogeneity in the type of implant used in the included studies. However, other reviews have shown broadly similar outcomes across the fourth-generation implants, suggesting an improvement across the board in outcomes across differing indications (Zijlker et al., 2022). In addition, an international study of over 100 TWA patients with a 2-year follow-up showed comparable satisfaction between patients with non-rheumatoid and rheumatoid aetiologies (Herzberg et al., 2012). Finally, due to the limitations of the available data, the suitability and outcomes of wrist arthroplasty in younger and more physically active individuals remains an unresolved issue (Berber et al., 2018).
As implants and survivorship continue to evolve, complication rates should continue to decrease, and TWA will continue to challenge wrist arthrodesis as the reference standard for patients with disabling wrist arthritis.
Supplemental Material
sj-jpg-1-jhs-10.1177_17531934231199317 - Supplemental material for A systematic review and network meta-analysis of outcomes after total wrist arthroplasty in inflammatory and non-inflammatory arthritis
Supplemental material, sj-jpg-1-jhs-10.1177_17531934231199317 for A systematic review and network meta-analysis of outcomes after total wrist arthroplasty in inflammatory and non-inflammatory arthritis by Han Hong Chong, Mate Zabaglo, Aqua Asif, Khalis Boksh and Kunal Kulkarni in Journal of Hand Surgery (European Volume)
Supplemental Material
sj-jpg-2-jhs-10.1177_17531934231199317 - Supplemental material for A systematic review and network meta-analysis of outcomes after total wrist arthroplasty in inflammatory and non-inflammatory arthritis
Supplemental material, sj-jpg-2-jhs-10.1177_17531934231199317 for A systematic review and network meta-analysis of outcomes after total wrist arthroplasty in inflammatory and non-inflammatory arthritis by Han Hong Chong, Mate Zabaglo, Aqua Asif, Khalis Boksh and Kunal Kulkarni in Journal of Hand Surgery (European Volume)
Supplemental Material
sj-pdf-3-jhs-10.1177_17531934231199317 - Supplemental material for A systematic review and network meta-analysis of outcomes after total wrist arthroplasty in inflammatory and non-inflammatory arthritis
Supplemental material, sj-pdf-3-jhs-10.1177_17531934231199317 for A systematic review and network meta-analysis of outcomes after total wrist arthroplasty in inflammatory and non-inflammatory arthritis by Han Hong Chong, Mate Zabaglo, Aqua Asif, Khalis Boksh and Kunal Kulkarni in Journal of Hand Surgery (European Volume)
Supplemental Material
sj-pdf-4-jhs-10.1177_17531934231199317 - Supplemental material for A systematic review and network meta-analysis of outcomes after total wrist arthroplasty in inflammatory and non-inflammatory arthritis
Supplemental material, sj-pdf-4-jhs-10.1177_17531934231199317 for A systematic review and network meta-analysis of outcomes after total wrist arthroplasty in inflammatory and non-inflammatory arthritis by Han Hong Chong, Mate Zabaglo, Aqua Asif, Khalis Boksh and Kunal Kulkarni in Journal of Hand Surgery (European Volume)
Footnotes
Acknowledgements
The authors would like to thank Pip Divall, Clinical Librarian of University Hospital of Leicester NHS Trust, UK for her assistance in conducting literature search for this meta-analysis.
Declaration of conflicting interests
The authors declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.