
Abstract
Manugraphy with three different cylinder sizes was used to quantify the contribution of fingers, thumb and palm to grip force in patients with unilateral cubital tunnel syndrome. Forces in the affected and contralateral hands differed by up to 29%. Although grip force is usually maximal when gripping small handles, ulnar nerve palsy resulted in similar absolute grip forces using the 100-mm and 200-mm cylinders. The contact area between the affected hand and the cylinders was reduced by 5%–9%. We noted a high correlation between the contact area and grip force, visible atrophy and permanently impaired sensibility. The load distribution differed significantly between both hands for all cylinder sizes. When gripping large objects, the main functional impairment in cubital tunnel syndrome is weakness in positioning and stabilizing the thumb. Weak intrinsic finger muscles are responsible for loss of force when gripping small objects.
Keywords
Introduction
Although the effect of ulnar nerve dysfunction on total grip force has been investigated previously (Kozin et al. 1999; Power et al. 2019), the individual contributions of the fingers, thumb and palm to the total grip force and load distribution have not previously been studied. We therefore carried out a prospective non-randomized experimental study in patients with cubital tunnel syndrome using manugraphy to determine these forces in the affected and unaffected hands.
Methods
Patients
Patients with a minimum age of 16 years with clinically and electrophysiologically diagnosed unilateral cubital tunnel syndrome who were scheduled for decompression surgery were eligible for this study. Patients were recruited from the outpatient clinic and after admission for surgery at a specialized hand surgery centre (Clinic for Hand Surgery, Rhön Klinikum AG, Bad Neustadt, Germany). The exclusion criteria included disorders affecting grip function, e.g. congenital deformities, sequelae after injury or surgery, rheumatic disease, neurological impairment other than cubital tunnel syndrome, Dupuytren’s disease or degenerative conditions. All patients were seen by a neurologist and had electrophysiological measurements, including a comparison of median and ulnar nerve conduction velocity, to confirm the diagnosis. All patients gave written informed consent before inclusion. The study received approval from the institutional Ethics Committee of the Clinic for Hand Surgery, Rhön Klinikum AG, Bad Neustadt, Germany (approval number 10_2018).
Study investigation
The patients’ demographic and clinical data, including age, sex, affected hand and hand dominance, were recorded. The subjectively perceived functionality of the upper limb was recorded by the Disabilities of the Arm, Shoulder and Hand (DASH) score (Germann et al., 1999). Pain at rest and under effort was ascertained by a numerical rating scale (NRS; 0 = none, 10 = maximum). Visible muscle atrophy was rated as none, slight or pronounced. Loss of sensibility was graded as intermittent or permanent. The presence of Wartenberg’s sign, Froment’s sign, claw deformity and the ability to cross the index and middle fingers were assessed.
Grip forces were measured using the analogue Jamar dynamometer (Sammons Preston, Bolingbrook, IL, USA), an analogue pinch meter (Baseline® Evaluation Instruments, White Plains, NY, USA) and with manugraphy (Manugraphy® system, novel GmbH, Munich, Germany).
For the Jamar dynamometer, handle positions 2 and 3 were used for grip force measurements, in the right and left hands alternately. The mean of three measurements was calculated. The key pinch and tip pinch were each measured three times using the pinch meter, alternating the right and left hands, and the mean values were calculated.
For manugraphy, three different cylinders with circumferences of 100 mm, 150 mm and 200 mm were used in sequence as described previously (Mühldorfer-Fodor et al., 2014) (Figure S1, available online). Sensor mats covering the cylinders measure the force applied to the device and the data are transmitted to the pliance® software in the equipment. Each of the cylinders was gripped with maximum force three times for 5 seconds, separated by a 10-second break, starting with the left hand and followed by the right hand. The mean value of the three sets was calculated. In addition, the pliance® software provided colour-coded 2-D or 3-D graphs resembling a digital handprint and depicting the contact area and the local pressure during gripping. These images and the underlying data allow identification of discrete regions of the hand for separate analysis. For this study, the grip force of the whole hand and the contributions of each finger, thumb, and the thenar and hypothenar regions were analysed. The relative or absolute differences between the affected and the opposite hand were calculated for the total force and for each predefined region of the hand.
Statistical methods
The R environment was used for statistical computations and graphics generation. The distribution of the data was examined using the Shapiro–Wilk test, homogeneity of variances, histograms and QQ plots. In view of the small number of participants and the skewed distribution for most parameters, non-parametric tests were used for descriptive statistics and comparison between groups. Thus, grip forces are presented as median with 95% confidence interval, range and interquartile range. The Wilcoxon signed-rank test was used to compare paired samples from the affected and healthy hands. After the categorization of data according to atrophy (none/slight/pronounced) or sensibility (intermittent/permanent), the Wilcoxon rank-sum test for unpaired samples was used to identify any significant differences between these groups. All p-values were two-tailed and p-values <0.05 were considered statistically significant.
For investigation of the correlation between the contact area and grip force, the Spearman’s rank correlation coefficient rho was calculated.
Results
Between September 2018 and May 2019, 41 patients underwent surgery for cubital tunnel syndrome. Of them, 27 patients (16 men, 11 women; median age = 59 years; IQR 50–67) were eligible and consented to participate (Table S1, available online). The left and right hands were affected in 14 and 13 patients, respectively. The median DASH score was 41 (IQR 22–53). The median period for symptoms was 12 months (IQR 6–33). Pain at rest (median 3; IQR 0–4.5) and under effort (median 3; IQR 0.5–6) were judged from the NRSs. Atrophy of the hypothenar muscles, the interossei and in the first web space were noted in seven, 16 and 20 patients, respectively, whereas intermittent and permanent loss of sensibility was reported by 11 and 16 patients, respectively. In 13 patients, a positive Froment’s sign was recorded, in five patients a positive Wartenberg’s sign was present and four patients had a claw deformity. In total, 11 patients were unable to cross their index and middle fingers. The median motor nerve conduction velocity of the distal and proximal cubital tunnel was 53 m/s (IQR 45–57) and 41 m/s (IQR 35–46), respectively.
Grip force and distribution of load
All techniques used to assess the grip forces indicated a much lower grip force in the affected hand relative to the unaffected one. These differences were most pronounced when using the Jamar dynamometer and the pinch meter (Figure 1 and Table 1). Furthermore, manugraphy revealed that the median forces generated by all areas in the affected hand, i.e. the thumb, the fingers, and thenar and hypothenar areas, were lower than in the corresponding areas of the healthy hand (Figure 1b–d). However, these changes were not statistically significant for the index finger (100-mm cylinder), small finger (150-mm cylinder), middle finger (200-mm cylinder) and hypothenar area (200-mm cylinder). Considering the diameter of the cylinder as an additional variable, the absolute force loss was greatest for the middle finger, thenar and hypothenar region with the 100-mm cylinder, for the thumb, index finger and thenar area with the 150-mm cylinder, and for the thumb and thenar area with the 200-mm cylinder (Table 2).
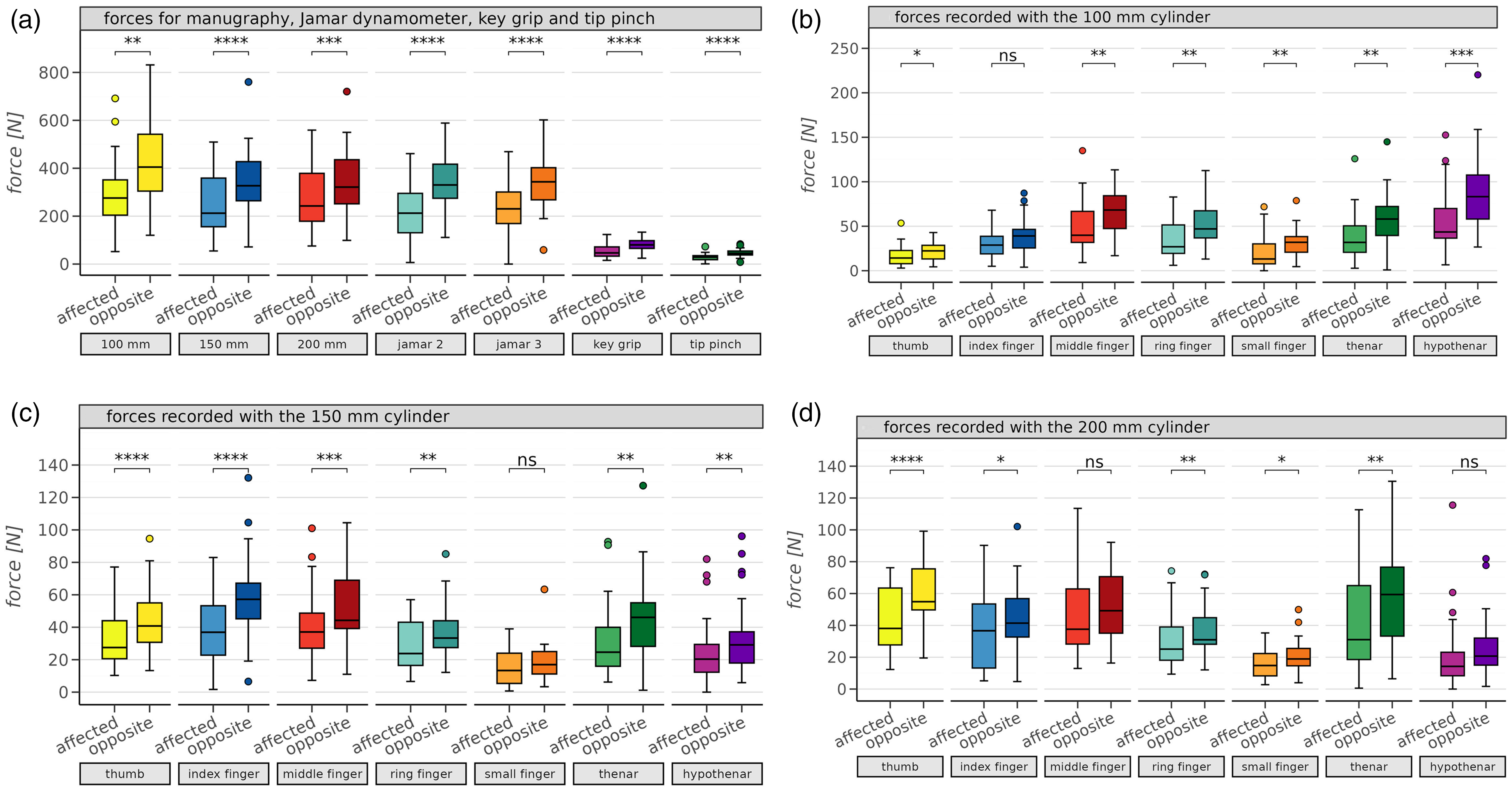
Box plots (median and interquartile range) depicting the grip force of the hand affected by cubital tunnel syndrome and the opposite, healthy hand. The lower whisker shows the minimum, the upper the maximum. Coloured dots represent outliners. (a) Results obtained for total grip forces with manugraphy and Jamar dynamometer together with those reflecting key grip and tip pinch. (b–d) Forces generated by thumb, fingers, thenar and hypothenar areas of the affected and opposite hand recorded with cylinders with circumferences of (b) 100 mm, (c) 150 mm and (d) 200 mm. ns: not significant; *p < 0.05; **p < 0.01; ***p < 0.001; ****p < 0.0001.
Relative differences in the grip forces and contact areas between the affected and opposite hands.
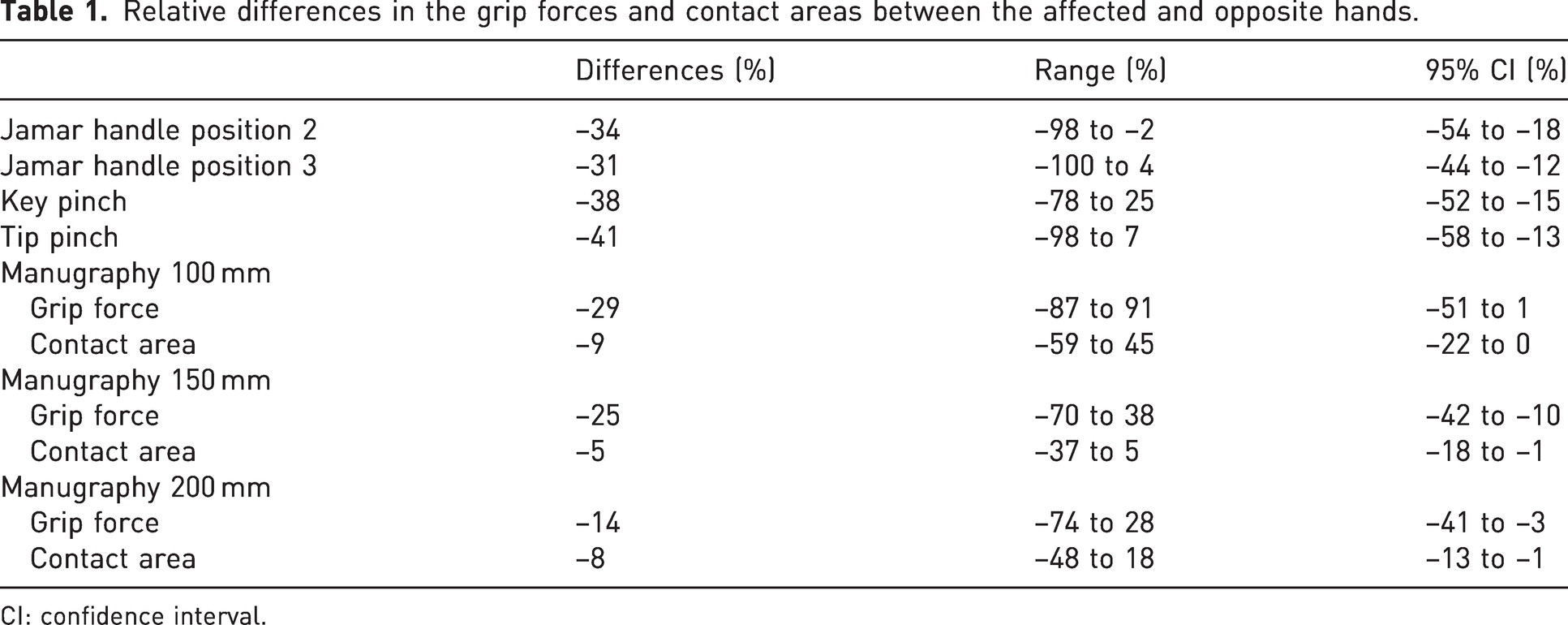
CI: confidence interval.
Differences in load distributions between the affected and opposite hands indicated by absolute force loss in seven hand areas.
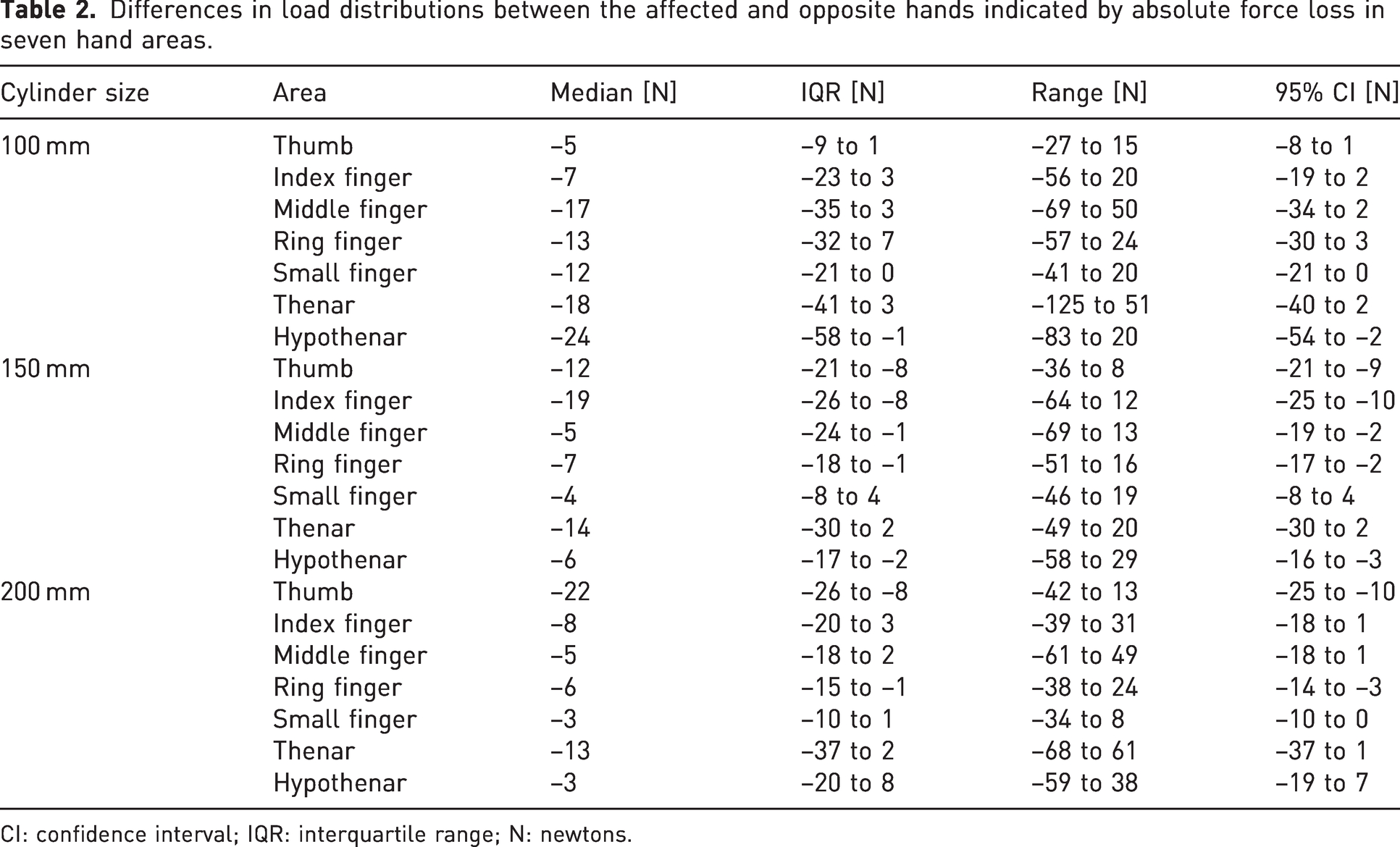
CI: confidence interval; IQR: interquartile range; N: newtons.
Contact area
Manugraphy revealed a significantly lower contact area in the affected hand compared to the non-affected hand. An example of the contact area when gripping a cylinder is shown in Figure 2. The results of the quantitative analysis are summarized in Table 1 and Figure 3a. There was a high correlation between the contact area and the grip force measured by either manugraphy or the Jamar dynamometer (contact area vs. handle position 2 or 3; rho = 0.86 and 0.91, respectively; p < 0.0001 for both).
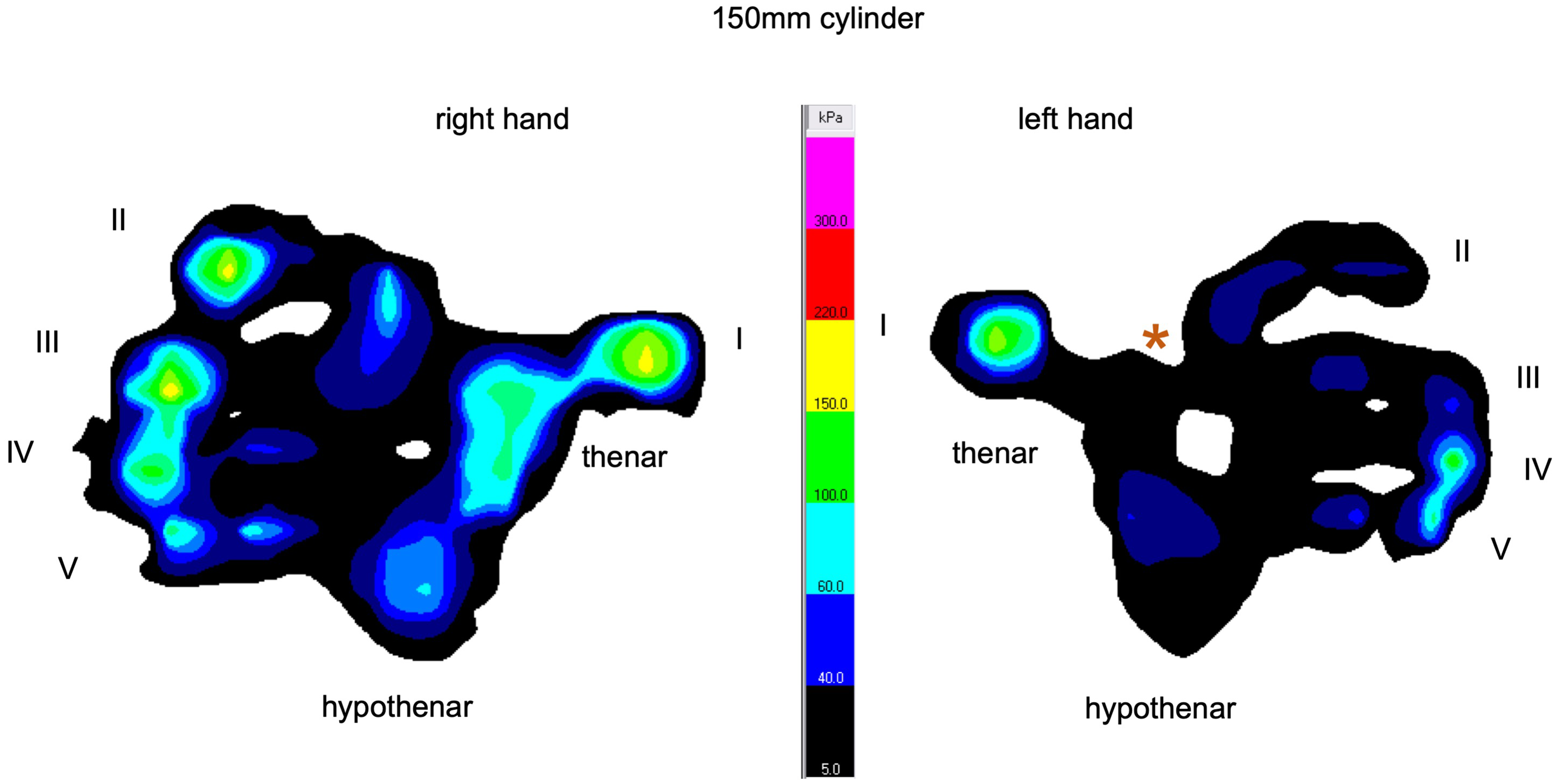
The colour-coded visualization of the load distribution and contact area in cubital tunnel syndrome affecting the left hand and the healthy right hand. Ulnar nerve palsy of the left hand results in significant deficits compromising all areas of the hand. The most notable deficits occur in the regions of the index, middle finger and the thenar area. The first web space does not transfer load; this area is marked with an orange asterisk. I: thumb; II: index finger; III: middle finger; IV: ring finger; V: small finger.
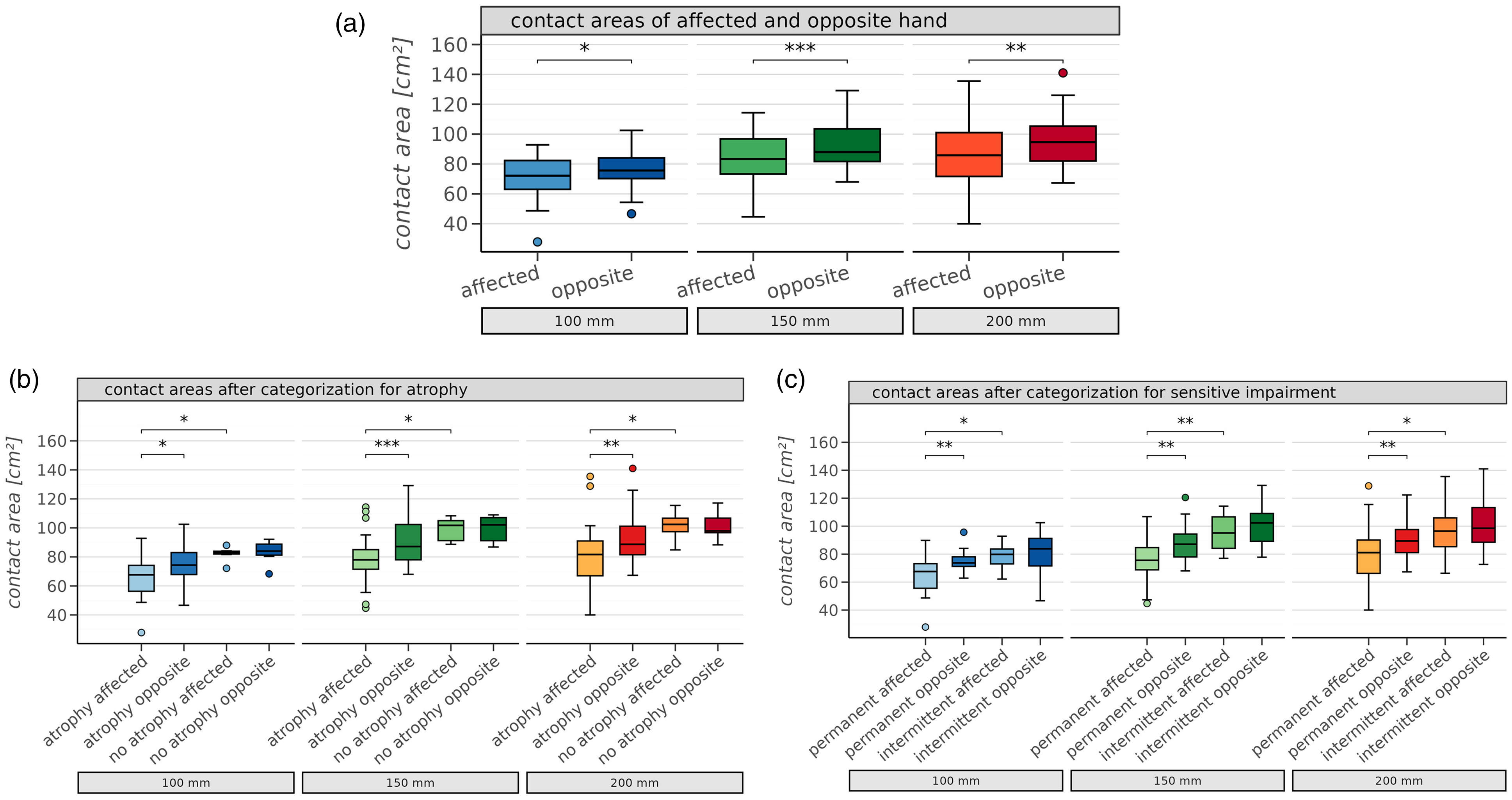
Box plots (median and interquartile range) depicting the total contact areas (cm2) of the affected hand with cubital tunnel syndrome and the opposite, healthy hand (a) in all patients and (b) after categorization for atrophy or (c) sensory impairment. ns: not significant; *p < 0.05; **p < 0.01; ***p < 0.001; ****p < 0.0001
The differences between the affected and non-affected hands were most prominent in patients with visible atrophy (Figure 3b), whereas when there was no atrophy, the differences were less. Further, for patients with permanently impaired (or reduced) sensibility, the contact area was significantly lower than in both the healthy opposite hand (p < 0.01) and the affected hand of patients with intermittently impaired sensibility (p < 0.05) (Figure 3c). However, in the latter group of patients, the contact areas of both hands were fairly similar.
Discussion
The manugraphy system includes cylinders that correspond to the handles of tools or bicycles (100-mm circumference), glasses, cups, handrails and handles of motorcycles (150 mm), or bottles, cans and caps on jars (200 mm). Further, grip forces measured by manugraphy and the Jamar dynamometer correlated well although the set-up of both devices differs (Mühldorfer-Fodor et al., 2014).
Intra-individual comparison of the total grip forces revealed a significantly reduced force in the affected hand compared to the healthy hand, which decreases with the increasing diameter of the manugraphy cylinder.
The smaller the object to be gripped, the more flexion of the metacarpophalangeal (MCP) joints is required (Gülke et al., 2010), which is produced by the intrinsic muscles. If MCP flexion is weakened owing to palsy of the interosseous muscles and some of the lumbrical muscles innervated by the ulnar nerve, gripping smaller cylinders becomes more difficult. Our data clearly support that this occurs along with an impaired transmission of force. With increasing cylinder size, less flexion of the MCP joints is needed and the force burden shifts distally toward the fingertips (Mühldorfer-Fodor et al., 2017; Radhakrishnan and Nagaravindra, 1993). Recruitment of the deep finger flexors of the thumb, index and middle finger is not compromised in ulnar neuropathy and thus the force transmitted via the fingertips increases when gripping larger objects. However, when gripping larger objects, the role of the thumb and the radial fingers increases (Mühldorfer-Fodor et al., 2017) but this may be compromised by palsy of the flexor pollicis brevis, adductor pollicis and the first dorsal interosseous muscles in cubital tunnel syndrome. Gripping might be compromised in some patients by an impaired ability to stabilize the thumb, whereas in others it may be a result of intrinsic weakness of the fingers, and in some both factors may be present. Knowledge of these functional relationships may help with choosing individual solutions, e.g. by providing larger handles to those having difficulties with tightly gripping small or medium-sized objects. Conversely, patients who need to grip mainly large objects may profit from a thumb orthosis or even reconstruction of the first dorsal interosseous muscle by tendon transfer (Nemoto et al., 2007).
In healthy hands, the contact area increases with increasing cylinder size as the hand is spread on the cylinder. This relationship was still maintained with cubital tunnel syndrome even though the contact area was significantly reduced compared to the opposite hand. It can be speculated that the reduction of tissue bulk in the hand by muscle atrophy might be the most relevant factor for loss of contact area (Figure 2). Palsy might also affect the ability to align all areas of the hand with the cylinder surface. Seo and Armstrong (2008) have reported that there is a correlation between hand size and grip force, but the influence of a pathological reduction of contact area, comparing both hands in one individual, has not previously been investigated. For all cylinder sizes, atrophy was associated with a significant loss of contact area, but grip force was similar to the healthy side when no atrophy was evident. Quantification of the contact area may be helpful for objective, measurable assessment of atrophy and to verify grip force loss; for example, when there is doubt about claims of incapacity for work or military service or in claims for financial compensation. Recording a lower grip force in combination with an almost unchanged size of contact area may suggest a suboptimal effort in grip force testing (Mühldorfer-Fodor et al., 2018; 2023).
Permanent loss of sensibility correlated significantly with the contact area and therefore with grip force. Among the 16 patients with permanent loss of sensibility, all but two had visible atrophy and one without atrophy had a claw deformity. In cases of intermittent loss of sensibility, there was no significant change in contact area, even though seven patients had a visible atrophy. In line with a recent report from Carteron et al. (2016), not only muscle weakness but also missing sensory feedback during gripping may reduce grip force. As a clinical consequence, simply asking about permanent or intermittent loss of sensibility will help to estimate the severity of cubital tunnel syndrome and the need for timely surgical treatment.
The most common features of cubital tunnel syndrome are the sensory deficits in the ring and small fingers, the Wartenberg’s sign and a claw deformity of the ulnar digits. The contribution of each part of the hand varies with the size of the object being gripped (Mühldorfer-Fodor et al., 2017). This explains why ulnar nerve palsy has a variable effect on the grip forces and load distributions for the three sizes of manugraphy cylinder. As the palm and fingers are most important when gripping small objects, the middle finger, thenar and hypothenar areas had the highest loss of grip force with the 100-mm cylinder. With increasing cylinder size, the contribution of the thumb and radial fingers increases. As a result, the effect of weakened muscles of the first web space is seen with the 150-mm and 200-mm cylinders, and also with losses of key and tip pinch forces of 38% and 41%, respectively. These findings are supported by earlier studies (Bultmann, 2009; Power et al., 2019; Zengin et al., 2017).
The limitations of this study include a lack of discrimination between the dominant and non-dominant hands when measuring grip force. The dominant hand can produce higher forces than the non-dominant side (Cai et al., 2018). Mühldorfer-Fodor et al. (2017) found that the load-distributions in the dominant and non-dominant hands are similar when gripping manugraphy cylinders. Only two patients in the study were left-handed and one of them had the left hand affected with cubital tunnel syndrome. For the rest of the right-handed patients, the right and left hands were equally affected, so handedness might not have influenced the study results to any extent. Another limitation was that the degree of ulnar nerve impairment varied among patients. This might be the reason that we found the median loss of grip force was less than in the study of Kozin et al. (1999).
Supplemental Material
sj-jpg-1-jhs-10.1177_17531934231198660 - Supplemental material for Force loss and distribution of load in the hands of patients with cubital tunnel syndrome
Supplemental material, sj-jpg-1-jhs-10.1177_17531934231198660 for Force loss and distribution of load in the hands of patients with cubital tunnel syndrome by Angelina Garkisch, Kristina Rohmfeld, Dagmar-Christiane Fischer, Karl-Josef Prommersberger and Marion Mühldorfer-Fodor in Journal of Hand Surgery (European Volume)
Supplemental Material
sj-pdf-2-jhs-10.1177_17531934231198660 - Supplemental material for Force loss and distribution of load in the hands of patients with cubital tunnel syndrome
Supplemental material, sj-pdf-2-jhs-10.1177_17531934231198660 for Force loss and distribution of load in the hands of patients with cubital tunnel syndrome by Angelina Garkisch, Kristina Rohmfeld, Dagmar-Christiane Fischer, Karl-Josef Prommersberger and Marion Mühldorfer-Fodor in Journal of Hand Surgery (European Volume)
Footnotes
Declaration of conflicting interests
The authors declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
The study gained approval from the institutional Ethics Committee and was conducted in accordance with the guidelines proposed in the Declaration of Helsinki (approval number 10_2018).
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Written informed consent was obtained from all participants before the study.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.